
Abstract
Background:
Hamstring strains are common among elite athletes, but their effect on return to the same level of play in American football has been incompletely characterized.
Purpose:
Data on National Collegiate Athletics Association Division I college football players with acute hamstring strains were gathered to identify the effects these injuries have on both return to play and athletic performance regarding velocity, workload, and acceleration.
Study Design:
Case Series; Level of evidence, 4.
Methods:
Injury data for a single Division I football team were prospectively recorded over a 4-year period. Players wore global navigation satellite system and local positioning system (GNSS/LPS) devices to record movement data in practices and games. The practice and game data were cross-referenced to evaluate players with isolated acute hamstring strains. Comparisons were made regarding players’ pre- and postinjury ability to maintain high velocity (>12 mph [19.3 kph]), maximal velocity, triaxial acceleration, and inertial movement analysis (IMA). There were 58 hamstring injuries in 44 players, of which 25 injuries from 20 players had GNSS/LPS data.
Results:
Players were able to return to play from all 25 injury incidences at a mean of 9.2 days. At the final mean follow-up of 425 days, only 4 players had reached preinjury function in all measurements; 12 players were able to return in 2 of the 4 metrics; and only 8 players reached their preinjury ability to maintain high velocity. For those who did not achieve this metric, there was a significant difference between pre- and postinjury values (722 vs 442 m; P = .016). A total of 14 players were able to regain their IMA. Players who returned to prior velocity or acceleration metrics did so at a mean of 163 days across all metrics.
Conclusion:
While players may be able to return to play after hamstring strain, many players do not reach preinjury levels of acceleration or velocity, even after 13.5 months. Further studies are needed to confirm these findings, assess clinical relevance on imaging performance, and improve hamstring injury prevention and rehabilitation.
Hamstring strains are a well-known cause of disability in American football players. It has been reported that they encompass 12% to 24% of all injuries at the high school and college level and are believed to be the most common type of muscle strain in athletes.9,20,28,31,35 Heiser et al 15 reported that hamstring strains occur at a rate of 7.7% per player-year in college football players. At the professional level, hamstring injuries account for 46% of practice injuries and 22% of preseason injuries, and hamstring strains have been found to be the most common lower extremity injury representing a 1-season risk of 9%. 12 Mack et al 24 found a 1-season risk of lower extremity injuries in National Football League players to be 41% with the majority of these being hamstring strains. An epidemiological study of 25 National Collegiate Athletic Association (NCAA) sports demonstrated that college football players sustained 35.3% of all hamstring injuries. 10 Despite the frequency of these injuries, there are limited data on return-to-play performance after hamstring strains in American football. Epidemiological studies have evaluated timing and rates of return to play for elite athletes with hamstring injuries, but postinjury athletic performance is not well-characterized.10,11,22 Studies in sprinters have demonstrated that even with 90% recovery of function they did not feel ready to return to full activity. 1 Another study evaluating Australian football players found that over one-third of players with hamstring injuries had residual signs of injury on magnetic resonance imaging (MRI) at 6 weeks. 7 Determining the natural progression of hamstring injuries and monitoring level of performance is critical in identifying safe and adequate return to play.
Wearable technology such as global navigation satellite system and local positioning system (GNSS/LPS) devices allows for objective measurements of an athlete’s movement. Multiple studies have demonstrated this to be a reliable and valid means of assessing athletic performance.8,16,18,29,32,37 This technology has been used heavily in Australian football, rugby, and soccer.13,17,21,23,26,27,31,34,37,38 More recently, GNSS/LPS data have been used in American football to evaluate their correlation with soft tissue injuries. 22 In this study by Li et al, 22 players were evaluated in the preseason and regular season for soft tissue injuries, which were then associated with the workload for the week on injury. They found that soft tissue injuries were associated with an acute increase in workload over the course of a month. However, the use of wearable technology to provide objective measurements on postinjury performance and return to play has been less studied.
The purpose of this study is to use objective GNSS/LPS data from wearable technology to determine the effect of hamstring muscle and tendon strains on (1) timing of return to play and, more specifically, the (2) ability to return to preinjury athletic performance as measured by velocity, workload, and acceleration. These findings may provide objective information on the impact of this common injury on return-to-play performance.
Methods
Certified athletic trainers for a single NCAA Division I football team prospectively recorded injury data on all players from September 2016 through August 2020. All starting players wore GNSS/LPS devices that prospectively recorded their movement data during practices and games in a separate database (Catapult Sports), demonstrated in Figure 1. Data recording began before the start of the practice or game and ran continuously until the practice or game was completed. The protocol for this study received institutional review board approval.

Wearable global navigation satellite system and local positioning system devices. The Catapult compression vest sits between the scapula with straps over the shoulders and underneath the axilla.
The electronic medical record was queried for all players who sustained an acute hamstring strain using the hamstring database codes of TMHX (hamstring strain), THMR (hamstring strain grade 3), KTHX (hamstring tendon injury), and THMB (biceps femoris strain grades 1-2). Players identified with acute hamstring injuries from the medical records were cross-referenced with the Catapult database to identify which players had both pre- and postinjury data. Return to play was determined by the date recorded in the medical records when the athlete was cleared to practice without restrictions. If the player had multiple injuries, the injuries were included as separate occurrences. We excluded 33 injuries for a final sample size of 25 injuries among 20 players (Figure 2).

Patient selection flowchart. Of the initial 58 injuries identified in the electronic medical record database, 25 injuries in 20 players were included for analysis. GNSS/LPS, global navigation satellite system/local positioning system.
Players were equipped with Catapult S5 units (Catapult Sports) assessing GNSS data at a sampling frequency of 10 Hz. The same units included LPS to capture triaxial acceleration assessing the magnitude and vector of movement at a sampling frequency of 100 Hz. The devices were placed between the players’ scapulae. The devices calculated maximal player “load,” maximal velocity (miles per hour [mph]), inertial movement analysis (IMA) (m/s), and distance (m) at which the player maintained a high velocity (>12 mph [>19.3 kph], as defined by the Catapult software).
Per the Catapult website, player load is defined as the instantaneous rate of change of acceleration divided by a scaling factor. It is the square root of the sum of the squared instantaneous rate of change in acceleration in 3 vectors (x, y, and z axes), using the internal triaxial accelerometer. 19 It is calculated as follows:

This metric has been validated as a way to quantify an athlete’s workload.4,6,28,33 For clarity in this article, we refer to this load as total triaxial acceleration.
The IMA uses data from a triaxial accelerometer and a triaxial gyroscope to graphically evaluate every movement the athlete makes in 3 dimensions, taking into account activities such as jumping or changing direction, without use of the Global Positioning System. In this study, high IMA was defined as a cumulative event count or change of speed in any direction >3.5 meters per second, arbitrarily set by the Catapult software.
The above metrics were immediately uploaded to a secure server after the activity. Pre- and postinjury maximal values were identified for each metric through review of the Catapult database. For the 4 players with multiple injuries, preinjury maximum was identified as the new maximum between their injuries. For example, if a player had 2 injuries, the preinjury maximum for his second injury would be the maximal value achieved between the first and second injury. This would also be the postinjury maximum for the player’s first injury.
Statistical Analysis
Paired 2-tailed t tests were used to compare pre- and postinjury maximums for (1) ability to maintain high velocity (>12 mph), (2) maximal velocity, (3) total triaxial acceleration, and (4) IMA. Additionally, we evaluated mean time to return to play, ability to return to previous level in each performance category, and the significance of pre- and postinjury levels for the players who did not return to their preinjury maximums.
Results
Players were able to return to play in all 25 injury incidences. The mean return to play was 9.2 days. However, after a mean follow-up of 425 days, only 4 (16%) of the 25 cases were able to reach preinjury maximal function in all measurements: total triaxial acceleration, IMA, maximal velocity, and ability to maintain high velocity. In fact, only 12 (48%) of the 25 cases were able to return to preinjury levels in 2 of the above metrics. Four of the players were unable to achieve any of their preinjury levels in any of the metrics. There was no correlation with player position, with 1 defensive back, 2 linebackers, and 1 tight end being unable to achieve any metric.
Of the individual values, the ability to maintain high velocity (>12 mph [>19.3 kph]) was the most consistently impaired. In only 8 cases were the players able to reach their preinjury function. The mean distance at which a player maintained a high velocity was decreased by 81.96 meters per session. In comparison, 14 of 25 cases were able to achieve preinjury IMA with a mean increase of 2.16 meters per second postinjury (Table 1).
Change in Catapult Parameters From Pre- to Postinjury Maximums a

A negative value means a decline in function or decreased ability. Boldfacedrows identify the 4 cases that were able to meet or exceed all 4 preinjury metrics. IMA, inertial movement analysis.
High velocity was defined as >12 miles per hour (>19.3 kilometers per hour).
When evaluating the difference between pre- and postinjury values of players who did not reach their preinjury function, there were significant differences in all 4 metrics (Figure 3). The greatest difference was seen in ability to maintain high velocity, defined as >12 mph or 55% of maximal velocity (722 vs 442 m; P = .016).
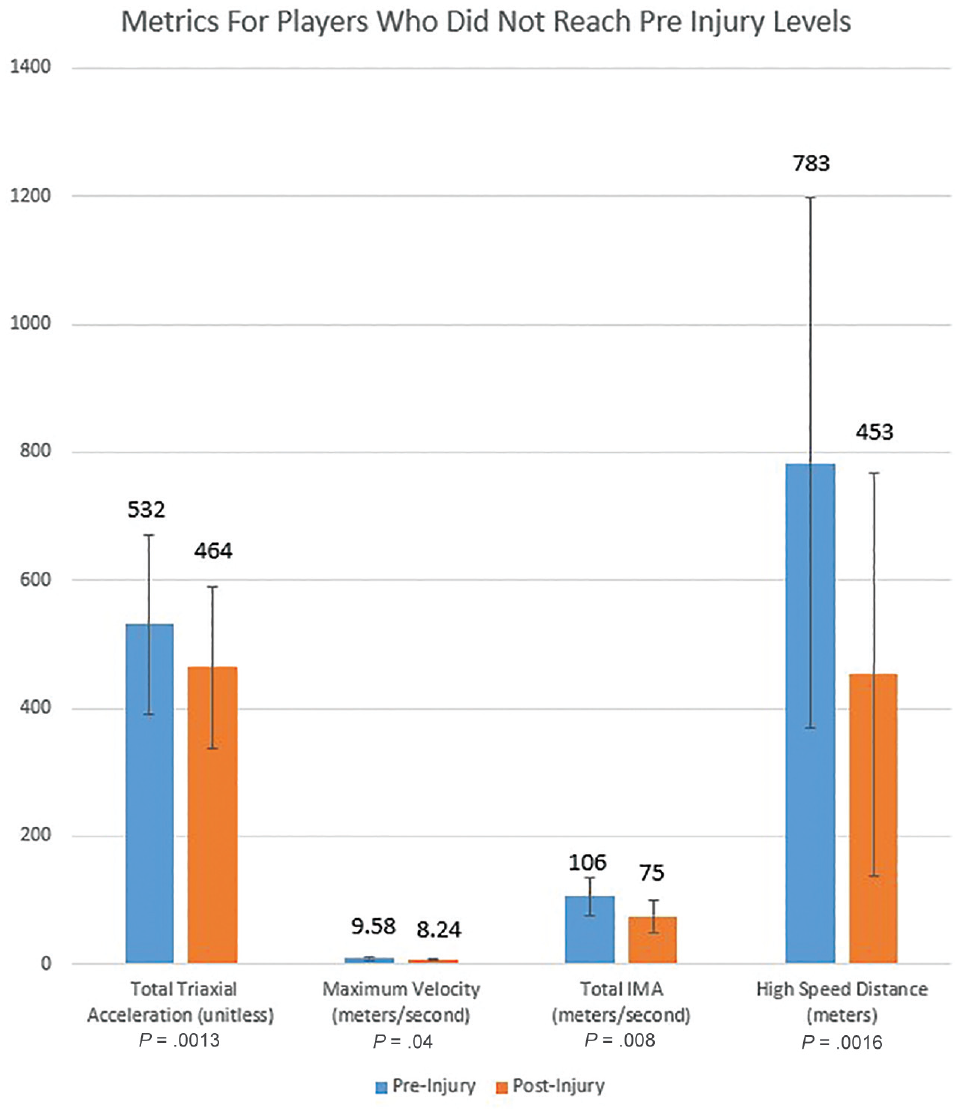
Change in metrics among players who did not reach preinjury metrics. All differences were statistically significant (P < .05), with the greatest difference seen in the distance the player could maintain a high velocity (>12 mph). IMA, inertial movement analysis.
For players who returned to preinjury function, total triaxial acceleration took the longest mean time to return to previous level, with a mean of 204 days. It took a mean of 189 and 185 days for players to return to their maximal velocity and IMA, respectively. The quickest metric to return was the patient’s ability to maintain high velocity, with a mean of 85 days. Simplified, this was a mean of 166 days across all metrics.
Discussion
Our study demonstrated a mean return to play of 9.2 days after hamstring strain. However, many players who were cleared for return to play were unable to reach their preinjury performance levels of acceleration or velocity, even almost 14 months after the injury. Even within a small sample size, significant differences were found in those patients that could not reach preinjury levels.
Our data on return to play are in line with previous data on elite-level football players. Elliot et al 11 demonstrated a mean of 13.2 days lost per athlete for this injury. Similarly, Cohen et al 5 demonstrated a mean of 11.3 practices and 2.6 games missed for professional football players. In other sports, a significantly longer return to play has been seen with a mean of 16 weeks in track sprinters compared with 31 weeks in “stretching” sports such as dancing.2,3 Previous studies have also looked at injury characteristics, such as the location of maximal tenderness or MRI findings, and have found that more proximal injuries and those involving the proximal tendon had a significantly longer time to return to preinjury levels.2,7,14,30
While many studies have looked at overall return-to-sport rate after hamstring injuries and the timing for return to the field, few studies have used objective measurements to determine return to preinjury performance.2,7,14,25,26,30,33,36 To our knowledge, there are limited studies that evaluate the effect of hamstring injury on postinjury athletic workload, acceleration, or velocity in the cleared athlete. Our data showed that despite an early and high rate of return to play of <10 days on average, the majority of players did not reach their preinjury performance until much later. Maintenance of high velocity, maximal velocity, IMA, and triaxial acceleration were routinely impaired and often preinjury levels were not achieved by time of final follow-up of 425 days (>1 season). Those who did achieve their prior levels took a mean 166 days, or almost 6 months.
High-speed distance was the most consistently impaired metric, as only 8 of 25 injuries recovered to preinjury values. For those who did not recover, the postinjury distance was almost half that preinjury distance. Counterintuitively, those players who did recover this metric did so at a mean of 85 days, which was much faster than the other metrics. This may be because these 8 players had less severe hamstring injuries than the players that were all included in time-to-return means for the other metrics.
These performance metrics could potentially be used to guide safe return to play. For example, maximal velocity may prove to be a key variable in determining a player’s readiness to return to sport. Askling et al 1 previously demonstrated that sprinters (an aptitude that can be extrapolated to some positions in football) sustained their hamstring injuries at high-speed sprinting. It is notable that the most profoundly affected metric in our study was the ability to sustain high-speed velocity, which may indicate incomplete recovery from injury and/or a protective adaptation to prevent reinjury.
Limitations
While this study provides a new approach to evaluating a player’s recovery from a hamstring strain, there are clear limitations. Despite obtaining data over a 4-year period, we included only a small cohort of 25 injuries, as the other injured players were not starters and thus did not wear the GNSS/LPS devices. Our findings may thus not be reproducible, and the cohort was too small to allow for subgroup analyses on player position. Additionally, given the retrospective nature of our study and the use of the athletic trainers’ medical record database, there were limitations in identifying specific details such as grade of injury, location of injury/tendon involvement, severity, use of advanced diagnostic modalities previously described in literature (ultrasound and MRI). As has been shown in prior studies, proximal injuries or those involving the tendon may be more severe than mid- or distal injuries, and thus our sample may be too heterogeneous. Furthermore, we did not differentiate between practice and game data, as all sessions were included. For ease of calculation, the pre- and postinjury maximums were used to determine return to previous level of performance, but these may also have been affected by fitness level or undocumented injuries. We identified 7 players (9 injuries) who had a separate lower extremity injury after their hamstring injury that may have confounded their ability to return to their preinjury maximal metrics. And finally, this specific wearable technology and its proprietary metrics do not yet have clear validation in return to sport after injury, thus limiting the reliability of our findings.
Despite these limitations, this study offers important information on return to play after hamstring injuries, for both coach, player, and medical staff expectations. Athletes who suffer in-season acute hamstring strains should be advised that while they may return to play quickly, they will have athletic deficits from their baseline that may not resolve in a single season. Our study adds to the increasing value of wearable technology on evaluating player performance and response to injury. Validation of our findings in a larger, more thorough prospective data set would allow for details on injury location, severity, and timing to be better correlated with player role and GNSS/LPS data and potentially provide guidance on injury prevention and rehabilitation.
Conclusion
While players may be cleared for return to play after hamstring strain, many players do not reach preinjury levels of acceleration or velocity, even after 13.5 months. Further studies are needed to confirm these findings, assess clinical relevance on imaging performance, and improve hamstring injury prevention and rehabilitation.
Footnotes
Final revision submitted September 27, 2023; accepted October 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.M.H. has received a grant from Arthrex and education payments from Arthrex, Saxum Surgical, and Smith & Nephew. A.O.G. has received education payments from Summit Surgical and hospitality payments from Arthrex and Zimmer Biomet Holdings. C.Y.K. has received education payments from Summit Surgical and hospitality payments from Arthrex. M.S.H. has received consulting fees from Linvatec; education payments from Summit Surgical and Arthrex; and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval of this study was obtained from the University of Washington (ref No. STUDY00010024).