
Abstract
Background:
The epidemiology of musculoskeletal injuries at the Australian Open, Wimbledon, and US Open tennis tournaments has been investigated in recent studies; however, there is no published literature on the incidence of musculoskeletal injuries at the French Open.
Purpose:
To describe the incidence, location, and type of musculoskeletal injuries in tennis players during the French Open tournament from 2011 to 2022.
Study Design:
Descriptive epidemiology study.
Methods:
A review was performed of all injuries documented by a multidisciplinary medical team during the French Open from 2011 to 2022. All musculoskeletal injuries that occurred during the main draw of the female and male singles or doubles matches were included. Descriptive statistics were used to summarize the data. Injury locations were grouped into regions as well as into upper limb, trunk, and lower limb.
Results:
In total, there were 750 injuries in 687 tennis players, resulting in a mean of 62.5 injuries per tournament; however, there were no obvious trends in injury incidence over the time frame evaluated. The number of injuries in female and male players was similar (392 vs 358, respectively). The most common injury regions were the thigh/hip/pelvis (n = 156), ankle/foot (n = 114), and spine (n = 103). The most common injury types were muscle-related (n = 244), tendon-related (n = 207), and joint-related (n = 163), and the most affected muscles were the adductors (n = 45), rectus abdominis (n = 38), and lumbar muscles (n = 25).
Conclusion:
Over the 12-year period from 2011 to 2022 female and male players experienced similar numbers of musculoskeletal injuries, with most injuries occurring in the lower limbs compared with the upper limbs and trunk.
The Grand Slam tournaments are the most prestigious tennis tournaments around the globe, comprising the Australian Open, French Open (Roland Garros), Wimbledon, and US Open. The epidemiology of musculoskeletal injuries at the Australian Open, 7 Wimbledon, 11 and US Open 21 have been investigated in 3 previous studies, with varying results. Two of these studies7,11 found that female players experienced more injuries than male players, while the other study 21 did not reach this conclusion. The most common injury location varied across studies, from the shoulder to the wrist, groin, knee, and ankle,7,11,21 with location differing according to sex in 2 of the studies.7,11 Furthermore, 2 studies11,21 found fluctuations in injury rates across the time frames evaluated, without identifying any trend or pattern, while the other study 7 found injury rates increased over time. The contrasting findings reported across tournaments could be due to differences in climate, time of year, and/or type of court surface, which is known to affect game length.3,10,17,19
There is no published literature on the incidence of musculoskeletal injuries at the French Open, which is the only Grand Slam tournament held on a clay court. Therefore, the purpose of the present study was to describe the incidence, location, and type of musculoskeletal injuries in tennis players during the French Open tennis tournament from 2011 to 2022. It is important to understand the injury epidemiology of this tournament, as it will allow medical staff to anticipate injuries and design more specific prevention programs.
Methods
The French Open is played over 3 weeks (1 week of qualifying followed by 2 weeks of main draw matches) at the end of May and beginning of June each year, except for in 2020 when it was played in September/October due to the COVID-19 pandemic. There are 128 female players and 128 male players in the main draw, who play in ≥1 of the following categories: men's singles, women's singles, men's doubles, women’s doubles, and mixed doubles. A multidisciplinary team is available on-site throughout the French Open to provide medical care, and this group includes a specialist radiologist for ultrasound imaging, a general practitioner to manage non-musculoskeletal injuries, and a team of sports medicine practitioners to manage musculoskeletal injuries. Cases that cannot be treated on-site are referred to an off-site specialist.
Injury Classification
A retrospective review of all injuries was performed during the French Open tennis tournaments from 2011 to 2022 as recorded by the multidisciplinary team in an electronic medical database. Injuries were defined as any lesion for which a player required medical consultation by a tournament physician during the French Open. We reviewed all musculoskeletal injuries of female and male players that occurred during the main draw tournaments (singles, doubles, and/or mixed doubles), including both practice sessions and matches. Musculoskeletal injuries that occurred during the week of qualifying as well as all non-musculoskeletal injuries were excluded.
The patient demographics (age, sex, nationality, and dominant side) and injury data including date of injury, injury category (musculoskeletal or non-musculoskeletal), injury location (shoulder, elbow, spine, etc), and injury type (muscle-related, tendon-related, joint-related, etc) were recorded from the medical database. It is important to note that the injury type was sometimes recorded as undiagnosed; this meant that the source of pain was not identified and further tests were not performed, most likely because the athlete did not want them.
Data Analysis
Descriptive statistics were used to summarize the data. Injury locations were grouped into regions (thigh/hip/pelvis, ankle/foot, spine, knee/lower leg, shoulder/upper arm, wrist/hand, abdomen/chest, elbow/forearm, and head) as well as into 3 categories (upper limb, trunk, and lower limb). Chi-square and Fisher exact tests were performed to check for differences between female and male players in the distribution of injury locations, injury regions, injury categories, and injury types. Scatter plots and bar charts were created to analyze the change in the number of injuries across the 12-year study period. Pie charts were created to analyze the distribution of muscle, tendon, and joint injuries. P <.05 was considered significant. Statistical analyses were performed using R, Version 4.1 (R Foundation for Statistical Computing).
Results
During the French Open from 2011 to 2022, a total of 750 musculoskeletal injuries in 687 tennis players were recorded (Table 1). The total number of injured players per tournament varied between 42 and 69, with a mean of 62.5 injuries per tournament across the 12-year period. Of the 687 injured tennis players, most had only 1 injury per tournament (n = 628; 91.4%), while some had 2 injuries (n = 52; 7.6%), 3 injuries (n = 6; 0.9%), or 4 injuries (n = 1; 0.1%). The injured tennis players had a mean age of 27.2 ± 5.4 (range, 15-44 years), and the number of injured female and male players was similar over the 12-year period (358 vs 329, respectively). There were considerable fluctuations in the incidence of injured players over the 12-year period, but there were no obvious increasing or decreasing trends for the whole cohort or for each sex (Figure 1). It is worth noting that more female players were injured in 2015 compared with the rest of the years and compared with male players that same year; also, less female and male players were injured in 2020 and 2021, during the COVID-19 pandemic, compared with other years.
Characteristics of Injured Tennis Players During the French Open, 2011-2022
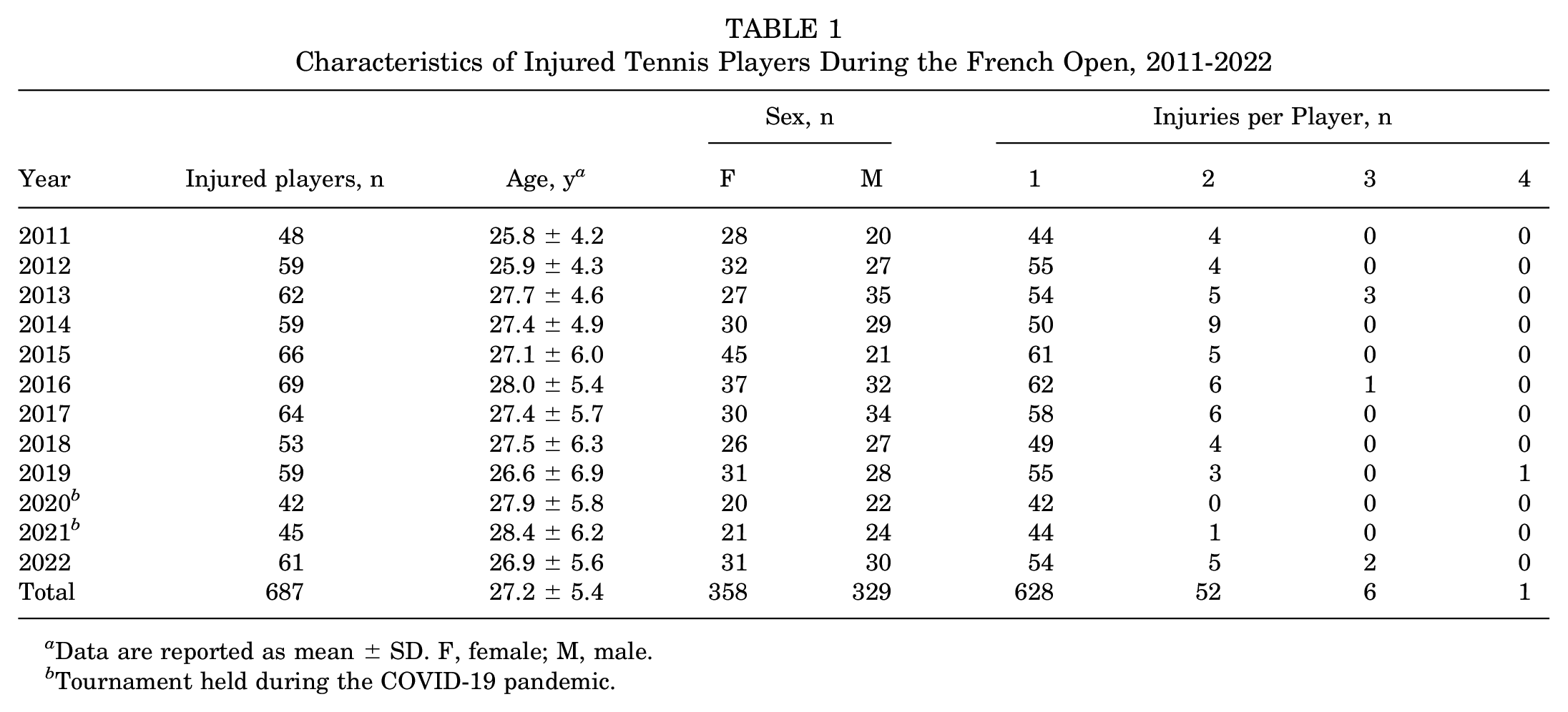
Data are reported as mean ± SD. F, female; M, male.
Tournament held during the COVID-19 pandemic.

Number of injured tennis players (solid line), female tennis players (dashed line), and male tennis players (dotted line) during the French Open, 2011-2022.
The most common injury locations were the thigh (n = 92; 12.3%), shoulder (n = 89; 11.9%), and knee (n = 78; 10.4%) (Table 2). When injuries were grouped into regions, the most common injured regions were the thigh/hip/pelvis (n = 156; 20.8%), ankle/foot (n = 114; 15.2%), and spine (n = 103; 13.7%) (Figure 2). When injuries were grouped into 3 location categories, lower limb injuries (n = 366; 48.8%) were more common than upper limb injuries (n = 218; 29.1%) and trunk injuries (n = 166; 22.1%). There were significant sex-based differences in the distribution of injury locations (P = .037) and injury regions (P = .010); however, there were no significant differences between the sexes when grouping injuries into lower limb, upper limb, and trunk (P = .646).
Location and Type of Musculoskeletal Injuries During the French Open, 2011-2022 a

Data are reported as number of injuries (%).

Injuries stratified by location during the French Open, 2011-2022.
The most common injury types were muscle-related (n = 244; 32.5%), tendon-related (n = 207; 27.6%), and joint-related (n = 163; 21.7%) (Figure 3). There were no significant sex-based differences in the distribution of injury types (P = .524). Of the 244 muscle injuries, the most common involved the adductors (n = 45; 18.4%), rectus abdominis (n = 38; 15.6%), and lumbar muscles (n = 25; 10.2%) (Figure 4A). Of the 207 tendon injuries, the most common involved the infraspinatus or supraspinatus tendons (n = 41; 19.8%), patellar tendon (n = 24; 11.6%), and Achilles tendon (n = 24; 11.6%) (Figure 4B). Of the 163 joint injuries, the most common involved the lumbar joints (n = 38; 23.3%), patellofemoral joint (n = 17; 10.4%), and hip joint (n = 11; 6.7%) (Figure 4C).

Injuries stratified by type during the French Open, 2011-2022.

(A) Muscle-related injuries, (B) tendon-related injuries, and (C) joint-related injuries during the French Open, 2011-2022.
Further analysis evaluating injury types per region indicated that the most common injury type was muscle-related for the thigh/hip/pelvis (n = 108) and abdomen/chest (n = 53). It was tendon-related for the shoulder/upper arm (n = 53; 57.0%), ankle/foot (n = 47), elbow/forearm (n = 28), and wrist/hand (n = 26) and joint-related for the knee/lower leg (n = 35) (Table 3).
Cross-Table of Injury Location and Injury Type a

Data are reported as number of injuries (%). Missing 1 bony injury at the head.
Discussion
The findings of the present study indicated that over the 12-year period from 2011 to 2022, there were a total of 750 injuries in 687 tennis players throughout the French Open tournaments, resulting in a mean of 62.5 injuries per tournament. The total number of injured female and male players was similar (358 vs 329, respectively); however, there were no obvious trends in the number of injured players over the time frame evaluated. Most injuries occurred at the lower limbs (n = 366) compared with the upper limbs (n = 218) and trunk (n = 166). The most common injury types were muscle-related (n = 244), tendon-related (n = 207), and joint-related (n = 163), and the most affected muscles were the adductors (n = 45), rectus abdominis (n = 38), and lumbar muscles (n = 25). This data allows medical staff to anticipate injuries and design specific prevention programs that target the most commonly injured muscles, tendons, and joints.
The epidemiology of musculoskeletal injuries in tennis players has been extensively reported,1,2,4,6,9,12-16,18 with a number of reviews published within the past 20 years.2,14,18 However, there are only 3 published studies that describe the injury epidemiology of Grand Slam tournaments, including the Australian Open, 7 Wimbledon, 11 and US Open. 21 Interestingly, the findings of these 3 studies are not in complete agreement with each other or with the present study, which could be due to differences in the time periods evaluated, as there is little to no overlap between the present study (2011-2022) and those of the Wimbledon 11 (2003-2012) and US Open 21 (1994-2009) studies. Two of the studies7,11 found that female players experienced significantly more injuries than male players, while the other study 21 and the present study found similar injury rates between sexes. In addition, 2 of the published studies11,21 and the present study found no trend in injury rates across the time frames evaluated, while the other study 7 found injury rates to increase over time. Furthermore, there was disagreement regarding the most common injury location, which involved the shoulder and knee respectively for women and men in the Australian Open, 7 the shoulder and thigh in the French Open, the wrist and groin in Wimbledon, 11 and the ankle in the US Open. 21 Interestingly, all 4 studies agree that players sustained more injuries in the lower limbs than in the trunk and upper limbs7,11,21 and that the most common injury types were muscle-related 7 or muscle- and tendon-related.11,21
The contrasting findings reported across Grand Slam tournaments could be due to differences in climate and time of year, which affect the air temperature and humidity and may affect the physical condition of the player, as well as the type of court surface. Clay is a soft material with a low friction coefficient, which results in lower loading and greater sliding distances, especially compared to hard courts, 5 this may lead to players’ experiencing more evenly distributed loads over time, possibly reducing the player's risk of injury. 23 Published studies22,23 have shown that greater sliding distances are accompanied with later occurrence of peak knee flexion, suggesting longer time spent braking and a greater requirement for muscular control, which may increase the likelihood of fatigue. The present study found that the most common injury type on clay was muscle-related and that the muscles more commonly involved in injuries were the adductor muscles, which are heavily used during sliding. Further studies should evaluate whether clay is a safer surface, in terms of injury incidence and severity, as compared with grass and hard courts.
Court surface is known to affect match length3,10,17,19; in fact, a recent meta-analysis 17 found a longer rally duration on clay (mean, 7.1 seconds; 95% CI, 6.2-8.1 seconds) compared with grass (mean, 4.3 seconds; 95% CI, 3.1-5.9 seconds) and hard court (mean, 5.6 seconds; 95% CI, 4.9-6.5 seconds). Longer rally durations should result in longer matches, and this could be expected to result in higher injury rates. However, this does not seem to be the case, since the mean number of injuries per tournament were 70.0 during the main draw of Wimbledon (grass) between 2003 and 2012, 58.4 during the main draw of the Australian Open (hard court) between 2011 and 2016, and 76.2 during the qualifiers and main draw of the US Open (hard court) between 1994 and 2009. In comparison, the present study found a mean number of injuries per tournament of 62.5 during the main draw of the French Open (clay) between 2011 and 2022; when removing the 2 years affected by the COVID-19 pandemic (2020 and 2021), the mean injury rate increased to 66.2.
In the 2015 French Open tournament, the number of injured female players was considerably greater compared with the rest of the years and compared with male players that same year. The most common injury location for women in 2015 was the wrist/hand (21%), which was double compared with the rest of the years (10.7%). During the 2015 tournament, there was a heatwave with temperatures reaching 33.9°C, but we are uncertain as to whether this could have caused the increase in injuries.
It is important to note that during the 2020 and 2021 tournaments, there were considerably fewer injuries recorded compared with the rest of the years. These years coincided with the COVID-19 pandemic, during which there were no spectators at the tournament. Although there were no changes or restrictions to medical care during COVID-19, it is possible that players with minor injuries did not go to the medical room, a large but closed room usually full of people, as they wanted to decrease their risk of exposure to the virus. In addition, during 2020, the French Open was postponed to the end of September, just 3 weeks after the US Open, which could have contributed to improved physical condition.
Limitations
This retrospective study has a number of limitations. First, the demographics of the non-injured players were not available; therefore, it was not possible to evaluate whether certain demographics were associated with a higher risk of injury. Second, the number of matches played, number of sets played, and match length were not recorded for each player; therefore, it was not possible to calculate the injury rate per match/set/time exposure. Furthermore, the total number of matches played at the tournament (including the main draw and qualifying rounds) before the injury occurred was also not available, which could have been used to study the effect of previous matches played on injury rates. A previous study has shown that there is a significant increase in medical withdrawal rates beyond the fourth match played. 8 Third, the present study did not classify injuries according to the Orchard Sports Injury and Illness Classification system, 20 rendering direct comparisons with the previous Grand Slam studies difficult. Fourth, the type of injury was not established at the time of medical consultation in 61 (8.1%) of cases and was therefore reported as undiagnosed. Finally, we do not know the severity of the injuries or whether they occurred during singles or doubles matches.
Conclusion
Over the 12-year period from 2011 to 2022, there were a total of 750 musculoskeletal injuries in 687 tennis players throughout the French Open tournaments. The number of injured female and male players was similar, with most injuries occurring at the lower limbs compared with the upper limbs and the trunk, and the most common injury type was muscle-related, followed by tendon-related and joint-related. This data allows medical staff to anticipate injuries and design specific prevention programs that target the most commonly injured muscles, tendons, and joints.
Footnotes
Acknowledgements
The authors are grateful to Babette M. Pluim, Brian Hainline, Carolyn Broderick, and Remi Azemar for their help with data collection as well as to Luca Nover for his help with data analysis. The authors are grateful to Clinique Trenel for providing funding for data analysis and manuscript writing.
Final revision submitted September 20, 2023; accepted October 5, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.