
Abstract
Background:
Increased posterior tibial slope (PTS) has been identified as a risk factor for failure after anterior cruciate ligament (ACL) reconstruction. Correction of PTS may improve outcomes after revision ACL reconstruction. There are conflicting reports demonstrating the measurement of the PTS on standard short knee (SSK) radiographs versus full-length lateral (FLL) radiographs including the entire tibia.
Purpose/Hypothesis:
To compare PTS measurements between SSK and FLL radiographs in patients who failed primary ACL reconstruction. It was hypothesized that there would be high variability between the SSK and FLL radiographic measurements.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
The medial and lateral PTS were measured on the SSK and FLL radiographs of 33 patients with failed primary ACL reconstructions. All measurements were performed by 2 trained independent observers (A.A.M., J.S.), and inter- and intraobserver reliability were calculated using the intraclass correlation coefficient (ICC). Measurements recorded by the observer with the higher intraobserver ICC were used for comparison of the PTS on SSK versus FLL radiographs.
Results:
Both the inter- and the intraobserver reliability values of the PTS measurements were excellent. There was a significant difference in mean PTS on the medial plateau as measured on the SSK and FLL radiographs (11.2°± 5.3° vs 12.5°± 4.6°; P = .03), with the FLL radiographs demonstrating higher PTS. There was also a significant difference in the mean PTS on the lateral plateau as measured on SSK versus FLL radiographs (10.7°± 4.3° vs 12.2°± 4°, respectively; P = .01), with the FLL radiographs demonstrating higher PTS. Notably, 66.67% of the absolute measurements for PTS on the medial plateau differed by ≥2°, with variability as high as 8.5°.
Conclusion:
Results indicated that FLL and SSK radiographs are not interchangeable measurements for PTS associated with failed ACL reconstruction. Because FLL radiographs demonstrate less variability than SSK radiographs, we recommend obtaining them to evaluate these complex patients.
Keywords
Increased posterior tibial slope (PTS) has been identified as a risk factor for both short-term and long-term failure after anterior cruciate ligament (ACL) reconstruction. ‡ Recent literature has demonstrated correction of PTS may improve outcomes after revision ACL reconstruction by decreasing ACL graft strain and subsequent rerupture.4,8,12,20,21 Attention has been given to assessing this single plane deformity; however, conflicting reports exist demonstrating different ways to measure the PTS on standard short knee (SSK) radiographs versus full-length lateral (FLL) radiographs that include the entire distal lower extremity.1,16,18-21 PTS has previously been defined as the angle between the tibial plateau and the mechanical axis of the tibia from the midpoint of the plateau to the midpoint of the tibiotalar joint. 6 Others have attempted to measure PTS using the more common knee radiograph using a variety of different anatomic references along the proximal tibia. Dejour et al 5 used the midpoint between the anterior and posterior cortices just distal to the tibial tubercle and 10 cm below that point. Faschingbauer et al 6 compared PTS on full-length tibial radiographs to lateral knee radiographs at 3 different lengths up to 20 cm distal to the tibial plateau. Yoo et al 25 compared the full-length mechanical axis to 5 different anatomic reference points. Furthermore, some have advocated for the utilization of advanced imaging such as computed tomography (CT) 26 or magnetic resonance imaging (MRI)9,11 to measure PTS, though these are not as routinely available or obtained for all patients.
The purpose of this study was to compare PTS measurements between SSK and FLL radiographs in a failed primary ACL reconstruction cohort. We hypothesized that variability would exist between the PTS measurements obtained using FLL versus SSK radiographs.
Methods
The protocol for this study received institutional review board approval. All patients who were evaluated with a failed ACL reconstruction by a single, high-volume revision ACL surgeon (W.R.L.) from August 2016 to February 2021 were reviewed. Patients with long-standing anteroposterior hip-knee-ankle (HKA) radiographs, FLL radiographs including the knee and ankle, and standard anteroposterior/SSK radiographs were included. Patients with incomplete imaging, imperfect lateral radiographs (defined as >5-mm posterior femoral condylar obliquity), open physes, prior osteotomy or tibial fracture, or metabolic bone disorder were excluded.
From an initial cohort of 187 patients who had failed ACL reconstruction, 33 complete sets of radiographs in 33 patients were included in the study (Figure 1). There were 21 male and 12 female patients, with a mean age of 30 years (range, 15-55 years).
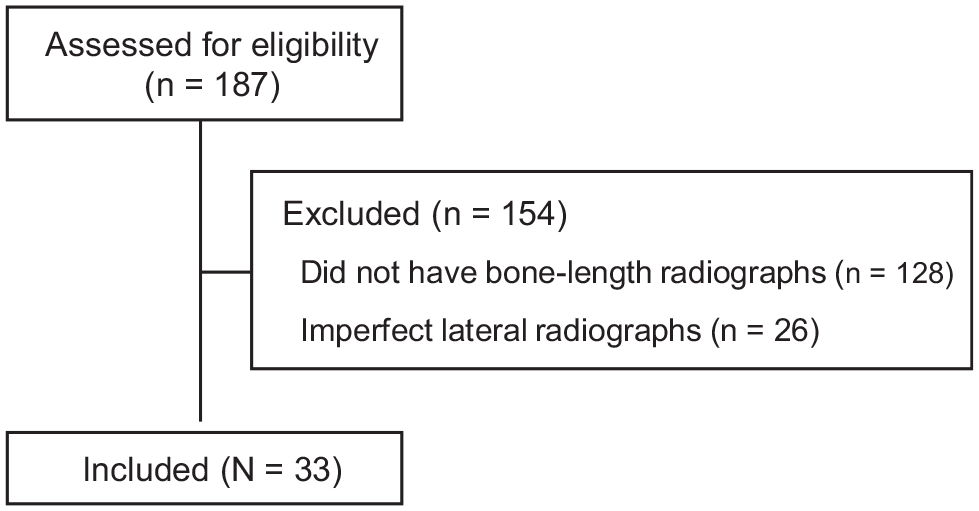
Patient Inclusion Process Flowchart.
Radiographic Measurements
Measurements for coronal plane deformity were obtained by drawing the mechanical axis line from the center of the femoral head to the center of the tibial plafond on standing anteroposterior radiographs. A line passing through the center of the knee joint (bisecting the tibial spines) was denoted as neutral, through the medial compartment (varus angulation) as a negative integer, and through the lateral compartment (valgus angulation) as a positive integer. Coronal plane alignment was quantified using a mechanical tibiofemoral axis line by measuring the angle created by a line drawn from the center of the femoral head to the center of the distal femur and a line from the center of the tibial plateau to the center of the tibial plafond. The PTS was measured on the SSK and FLL radiographs using previously published methods.6,23 PTS on the radiographs was measured using the technique described by Utzschneider et al, 23 in which the angle created by the tangent to the tibial plateau and a line connecting the anterior and posterior tibial cortices 5 cm and 15 cm distal to the knee joint were then averaged (Figure 2A). PTS on the FLL radiographs was measured as the angle formed by the tangent of the tibial plateau to a line drawn from the center of the tibial plateau and the center of the tibial plafond (Figure 2B). 6 Using picture archiving and communication system imaging archive software (Fujifilm), the PTS values for the medial tibial plateau and lateral tibial plateau were calculated separately.

Representative posterior tibial slope measurements from (A) a standard short knee radiograph and (B) a full-length lateral knee radiograph of the same patient.
The measurements were obtained by 2 independent observers (A.A.M., J.S.) who were trained in measuring knee radiograph angles. Both observers performed repeat measurements of a random subset of 20 patients 4 weeks after the first measurements to calculate intra- and interobserver reliability.
Statistical Analysis
The intra- and interobserver reliability of the radiographic measurements were measured with the intraclass correlation coefficient (ICC). The means and standard deviations of the PTS for the medial and lateral tibial plateaus were calculated using the measurements from the observer with the highest intraobserver reliability; data were reported in this manner as opposed to averaging the 2 observers’ measurements, as we felt this was the more accurate representation. Paired t tests were used for the comparison of PTS measurements between the SSK and FLL conditions. All analyses were performed in STATA (Version 17; StataCorp), with an alpha level of .05, indicating statistical significance at P < .05.
Results
The intra- and interobserver reliability for the medial and lateral PTS measurements are shown in Table 1. The interobserver reliability ICC for coronal alignment on HKA was 0.966 (95% CI, 0.933-0.985), indicating excellent reliability. The intraobserver reliability ICCs were 0.941 (95% CI, 0.858-0.977) and 0.967 (95% CI, 0.874-0.989) for observers 1 and 2, respectively, indicating excellent reliability.
Intraobserver and Interobserver Reliability for the PTS Measurements

Data are reported as intraclass correlation coefficient (95% CI). FLL, full-length lateral; HKA, hip-knee-ankle; PTS, posterior tibial slope; SSK, standard short knee.
Measurements for the medial and lateral PTS according to radiographic view are shown in Table 2. There was a statistically significant difference in the mean PTS on the medial plateau as measured on SSK versus FLL radiographs (11.2°± 5.3° vs 12.5°± 4.6°, respectively; P = .03). There was also a statistically significant difference in the mean PTS on the lateral plateau as measured on SSK versus FLL radiographs (10.7°± 4.3° vs 12.2°± 4°, respectively; P = .01). Further analysis indicated that 66.67% of patients (22/33) had an absolute difference in PTS of ≥2° between the medial plateau FLL and SSK films, and 63.64% of patients (21/33) had an absolute difference of ≥2° between the lateral plateau FLL and SSK films (Figure 3). In addition, 33.33% of patients (11/33) had a PTS of ≥12° on lateral plateau SSK compared with 57.58% (19/33) using the lateral FLL. Similarly, 45.46% of patients (15/33) had PTS of ≥12° on medial plateau SSK compared with 54.55% (18/33) using the medial FLL.
PTS Measurements on SSK and FLL Radiographs

Data are reported as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). PTS, posterior tibial slope; SSK, standard short knee; FLL, full-length lateral.

The absolute difference in the posterior tibial slope (PTS) measurements between the standard short knee (SSK) and full-length lateral (FLL) radiographs according to frequency (number of patients).
Discussion
The most important finding of this study was that two-thirds of the study patients had a ≥2° difference in the PTS as measured between the SSK and FLL radiographs. This finding raises concern with interchangeably using PTS measurements from both short-segment and full-length radiographs.
Several studies have compared short-segment knee radiographs to full-length radiographs with the aim of streamlining clinical practices to avoid obtaining long-leg radiographs and minimizing patient radiation exposure. Yoo et al 25 compared the accuracy of various measurement methods on standard knee radiographs to the mechanical axis as defined by the line connecting the midpoints of the tibial plateau and the tibial plafond. They found that the proximal anatomic axis (defined as the line connecting midpoints of outer cortical diameter at 5 cm and 15 cm distal to the knee joint) most closely paralleled the sagittal mechanical axis, with a mean difference of 0.2°. Utzschneider et al 23 introduced a new method of measuring PTS on short-leg films in which the mean of the slopes of anterior and posterior tibial cortices was calculated at 2 points distal to the knee joint. This method was found to have the highest correlation with 0.6 mm–slice 3-dimensional CT scan when using both long (15 cm distal to the joint; r = 1.0) and short (10 cm; r = 0.98) radiographs. The authors 23 suggested that this method could be the most useful for routine clinic short-leg films, as it avoids the increased radiation exposure when obtaining full-length radiographs or CT scans. Our results demonstrated, on average, greater slope measurements when using long-leg radiographs, with significant differences at both the medial and lateral tibial plateau (P = .03 and .01, respectively).
It is unclear whether increased PTS at the lateral or medial plateau plays a greater role in recurrent ACL injury. It has been hypothesized that a flatter medial slope with increased lateral slope may cause increased rotational movement of the knee, resulting in increased strain on the ACL graft. 10 Additionally, a recent study found a significant difference in average PTS using full-length radiographs depending on whether the anatomic or mechanical axis was used.3,15 Furthermore, some authors advocate for the use of CT or MRI for the calculation of slope. Naendrup et al 17 compared the mean tibial slope in patients undergoing revision ACL reconstruction and found differences of up to 5.4° between radiographs, CT scans, and MRI. Jahn et al 14 found that although both plain radiographs and MRI showed good-to-excellent intraobserver agreement, the mean PTS was significantly larger on radiographs as compared with MRI. They advised caution when comparing studies measuring PTS using different imaging modalities. The results of our study indicate that caution should be used even when using the same imaging modality.
Studies have demonstrated anterior closing-wedge proximal tibial osteotomy to be an effective procedure to correct the deformity in the revision setting.4,12,20 The results of our study have altered our practice and recommendations in patients with ACL rupture. We recommend obtaining HKA and FLL radiographs on all patients for baseline. The SSK and FLL can be compared, and if equivalent, SSK can be used in follow-up after osteotomy is performed to determine correction and healing without repeating the FLL. The methods we utilized for PTS evaluation showed excellent intra- and interobserver reliability. Our results supported our hypothesis that variability exists between FLL and SSK radiographs such that the 2 radiographic views cannot be used interchangeably. Our study also demonstrated variability between the 2 views as high as 8.5°. This amount of variability is concerning such that if it is overlooked, it may contribute to undercorrection or even no appreciation of increased PTS as a contributing factor necessitating correction.
Limitations
Our study has several limitations. First, it may be difficult to identify the medial and lateral tibial plateaus accurately and reproducibly on plain radiographs; however, the ICC values we obtained showed excellent agreement. Second, only 33 of the 187 eligible patients had complete imaging including full-length standing anteroposterior and lateral imaging with acceptable rotation. This is likely due to our evolving understanding of not only PTS but also the presence of coronal plane malalignment in patients presenting with a failed ACL reconstruction. Additionally, this was a radiographic analysis study, and it was not designed to conclude which radiographic technique is more relevant to the diagnosis and treatment of ACL patients with elevated PTS. Last, using the measurements from the observer with the highest intraobserver reliability rather than averaging the 2 observers’ measurements as done more often may be considered a limitation of this study. We did not use the averaging method because of our concern for its being less likely to reflect the true measurements.
Conclusion
Study results indicated that PTS measurements obtained on FLL radiographs were not interchangeable with those obtained on SSK radiographs with respect to analysis associated with failed ACL reconstructions, as two-thirds of the study patients had a ≥2° difference in PTS between the SSK and FLL radiographs. Because full-length radiographs demonstrate less variability than SSK radiographs, we recommend obtaining them to evaluate these complex patients.
Footnotes
Final revision submitted August 22, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.A.M. has received education payments from MedInc of Texas. W.R.L. has received consulting fees from Arthrex and MedInc of Texas, nonconsulting fees from Arthrex, royalties from Arthrex, and hospitality payments from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Texas Health Science Center at Houston (reference No. HSC-MS-20-0891).