
Abstract
Background:
Most studies regarding medial meniscus posterior root tear (MMPRT) report total Knee injury and Osteoarthritis Outcome Score (KOOS) subscale values as important patient-reported outcomes, but there are few symptom-specific characterizations of patients with MMPRT.
Purpose/Hypothesis:
The purpose of this study was to characterize the prevalence and severity of symptoms and functional limitations among patients with MMPRT based on item-level KOOS responses. It was hypothesized that patients with MMPRT would show similar symptoms to those of other meniscal tear types, with items from the KOOS pain subscale forming a majority of the most severe and prevalent symptoms.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The records of 1466 patients with medial meniscus root tear between January 2017 and December 2021 at a single institution were reviewed. KOOS subscale scores and item-specific responses from initial evaluation were collected for each patient. Each KOOS item was scored on a scale from 1 (none/least severe) to 5 (extreme/most severe). Median and mean item-level responses were calculated and ranked in order of most to least severe. For statistical analysis, item-level prevalence rates were calculated as the proportion of patients reporting at least mild symptoms and ranked from most to least prevalent.
Results:
Included were 61 patients with MMPRT verified on magnetic resonance imaging (MRI). The most severe items according to item-level KOOS response were as follows: awareness of knee problem (mean, 4.62 [95% CI, 4.47-4.78]), difficulty jumping (mean, 4.06 [95% CI, 3.73-4.39]), difficulty twisting or pivoting (mean, 4.04 [95% CI, 3.76-4.32]), difficulty kneeling (mean, 3.98 [95% CI, 3.65-4.31]), and modification of lifestyle (mean, 3.94 [95% CI, 3.69-4.20]). The most prevalent items were knee stiffness later in the day, pain going up- or downstairs, difficulty ascending stairs, difficulty getting in and out of the car, difficulty twisting or pivoting, awareness of knee problem, and modification of lifestyle, with all patients reporting at least mild symptoms for each. Of the 11 most severe and prevalent symptoms, 8 came from the KOOS-Pain item-specific responses.
Conclusion:
Pain-related items made up a majority of the most severe and most prevalent symptoms as identified by the item-specific KOOS responses. However, meniscal symptoms commonly seen in other tear types, such as clicking and knee stiffness, were still quite prevalent in patients with MMPRT.
Medial meniscus posterior root tears (MMPRTs) have biomechanical consequences that mimic total meniscectomy because of disruption of meniscal hoop stress resistance and increased tibiofemoral joint contact pressures.1,27 As a result of these changes, MMPRT has been linked to the development of bone marrow edema, spontaneous osteonecrosis of the knee (SONK), and osteoarthritis.19,31,37,40-42 Surgical root repair is a promising treatment option that can restore meniscal function for these patients.4,6,14,23,26,27,29,39 As such, early recognition of MMPRT is important in order to discuss treatment options with patients and avoid long-term degenerative changes.
The typical presentation of MMPRT is believed to be much like that of any meniscal tear, with 2 notable exceptions: more severe pain than usual and a more abrupt onset.15,22 However, definitive diagnosis of MMPRT generally relies on magnetic resonance imaging (MRI) and arthroscopic findings, 5 and it is unclear if there are specific symptoms of MMPRT that can aid in its diagnosis.4,20
The Knee injury and Osteoarthritis Outcome Score (KOOS) summary subscale scores and item-specific responses have been used to describe the clinical presentation of patients with other meniscal injuries.16,35 To our knowledge, there are no KOOS item-specific characterizations of the MMPRT phenotype. Such characterizations would be helpful for clinicians to recognize the profile of patients with MMPRT and set expectations regarding the typical symptoms experienced by patients with MMPRT.
In this study, we aimed to describe the KOOS item-specific presentation of MMPRT and report the most severe and prevalent symptoms and functional limitations in patients with MMPRT. We hypothesized that patients with MMPRT would have symptoms similar to those of other meniscal tear types, with items from the KOOS pain subscale forming a majority of the most severe and prevalent symptoms.
Methods
Patient Population
After receiving institutional review board approval for the study protocol, we reviewed the records of 1466 patients with medial meniscus root tears identified using International Classification of Diseases, 9th and 10th Revision diagnosis codes (for tear of medial cartilage or meniscus of knee; other meniscal derangements, unspecified medial meniscus; and other meniscal derangements, posterior horn of medial meniscus) between January 2017 and December 2021 at a single institution. Included in this study were patients with MRI-verified MMPRT, defined as a complete radial tear within 5 mm of the posterior bony attachment of the medial meniscus. Excluded were patients with incomplete tear on MRI review; concomitant ligamentous, bone, or other meniscal injury; no baseline KOOS questionnaire; MRI obtained outside the study period; diagnosis of established SONK on MRI review; previous ipsilateral knee surgery; and MRI of insufficient quality. Informed consent was not obtained due to the retrospective nature of the study.
Outcome Measures
Baseline descriptive characteristics were collected for each patient, including age, sex, body mass index (BMI), race, household income, and tobacco use. Data were also collected regarding the timeline of KOOS scoring relative to symptom onset.
Individual patient responses to all KOOS questionnaire items were collected at the time of initial evaluation. The KOOS is a validated 42-item questionnaire that assesses patients’ opinion about the symptoms and function of their knee.8,32 Each of the 42 items are classified into 1 of 5 subscales: Pain (9 questions), Symptoms (7 questions), Function in Activities of Daily Living (ADL) (17 questions), Function in Sport and Recreation (Sport/Rec) (5 questions), and Knee-Related Quality of Life (QOL) (4 questions). Responses to each item are scored on a scale from 1 (none/least severe) to 5 (extreme/most severe), and summary subscale scores are calculated based on an aggregate of the item-specific responses within each subscale. Scores are transformed to a scale from 0 (representing extreme knee problems) to 100 (representing no knee problems), as is common in orthopaedic assessment scales and generic measures.
Statistical Analysis
Statistical analysis was performed with SPSS Statistics Version 29 (IBM Corp). Descriptive statistics and independent t tests were used to report KOOS subscale scores and assess differences by sex. For the primary analysis, median and mean item-specific responses were calculated as a measure of item severity. Item-level responses were treated as continuous variables when calculating means and medians. All items were ranked from most to least severe according to median response, as the item-level data for this project were not normally distributed (P < .001, Shapiro-Wilk test). When needed, the mean value was used to reconcile equivalency. The prevalence of each KOOS item was also calculated. When calculating prevalence, the presence of a symptom or functional limitation was defined as response options 2 through 5 (ie, all except “none/least severe”). All items were ranked from most to least prevalent.
We performed a subanalysis wherein KOOS item responses were grouped as either symptoms (all items from the Pain and Symptoms subscales) or functional limitations (all items from the ADL, Sport/Rec, and QOL subscales) according to the methods described by Skou et al. 35 Items related to symptoms and to functional limitations were ranked separately according to severity and prevalence.
Results
Patient Characteristics
After applying exclusions to the original 95 patients, 61 patients were included in the sample (34 patients were excluded for incomplete tear on MRI review [n = 9]; concomitant ligamentous, bone, or other meniscal injury [n = 8]; no baseline KOOS questionnaire [n = 5]; no MRI obtained in study period date range [n = 4]; diagnosis of established SONK on MRI review [n = 3]; previous ipsilateral knee surgery [n = 3]; and MRI of insufficient quality [n = 2]) (Figure 1). The mean age of the sample was 54.15 ± 8.38 years, and 72.13% (44/61) of patients were female. The mean BMI of the patients was 32.21 ± 7.38 kg/m2. Overall, 70.49% (43/61) of patients had right-sided injuries. On average, patients were initially evaluated at 75.61 ± 111.34 days after symptom onset. Other characteristics can be found in Table 1.

Flow diagram of patient selection. KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear; MRI, magnetic resonance imaging; SONK, spontaneous osteonecrosis of the knee.
Characteristics of the Study Patients (N = 61) a
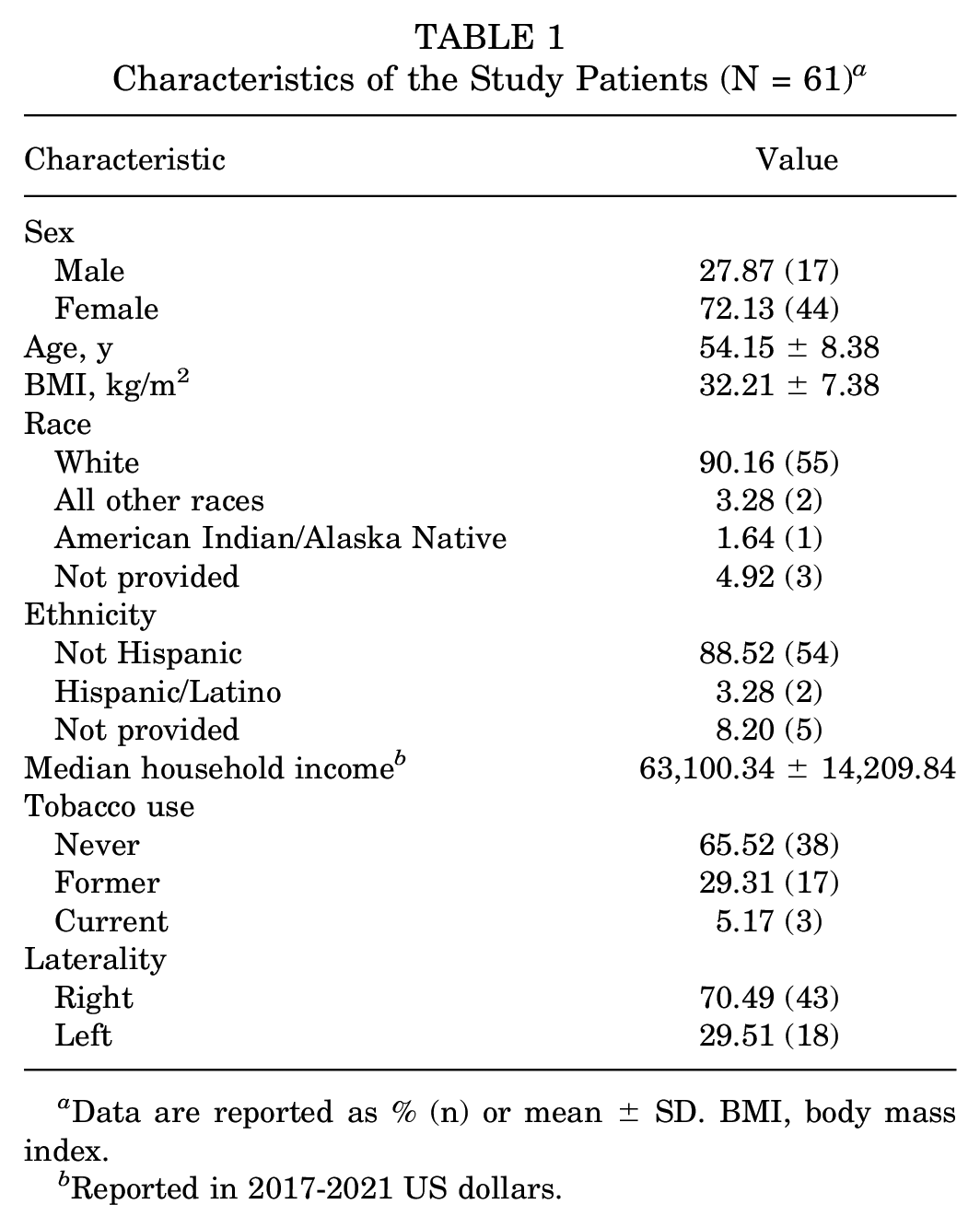
Data are reported as % (n) or mean ± SD. BMI, body mass index.
Reported in 2017-2021 US dollars.
KOOS Summary Subscale Scores
Among patients with MMPRT, the mean KOOS subscale values in order of most to least severe were QOL (25.0 ± 16.7), Sport/Rec (25.6 ± 24.0), Pain (46.3 ± 14.0), Symptoms (49.4 ± 17.9), and ADL (51.7 ± 15.9). There were no statistically significant differences by sex for any of the summary subscale scores (Table 2).
Comparison of KOOS Subscale Values According to Sex a

Data are reported as mean ± SD. Missingness ranged from 7 to 10 patients. ADL, Function in Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Knee-Related Quality of Life; Sport/Rec, Function in Sport and Recreation.
KOOS Item-Specific Responses
The most severe item-specific KOOS responses were awareness of knee problem (mean, 4.62 [95% CI, 4.47-4.78]), difficulty jumping (mean, 4.06 [95% CI, 3.73-4.39]), difficulty twisting or pivoting (mean, 4.04 [95% CI, 3.76-4.32]), difficulty kneeling (mean, 3.98 [95% CI, 3.65-4.31]), and modification of lifestyle (mean, 3.94 [95% CI, 3.69-4.20]) (Table 3). The most prevalent item-level KOOS responses were knee stiffness later in the day, pain while going up- or downstairs, difficulty ascending stairs, difficulty getting in and out of the car, difficulty twisting or pivoting, awareness of knee problem, and modification of lifestyle, with all patients reporting at least mild symptoms for each. Symptoms and functional limitations from all 42 KOOS items were seen in at least 75% of patients with MMPRT (Table 3).
Median and Prevalence of Item-Specific KOOS Responses Among Patients With MMPRT a

Missingness ranged from 7 to 10 patients for each item. ADL, Function in Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear; QOL, Knee-Related Quality of Life; Sport/Rec, Function in Sport and Recreation.
KOOS Items Related to Symptoms Among Patients With MMPRT
The most severe symptoms among patients with MMPRT, ranked from most to least severe, were as follows: knee pain in general (mean, 3.92 [95% CI, 3.67-4.18]), pain while twisting or pivoting (mean, 3.63 [95% CI, 3.35-3.91]), pain while climbing stairs (mean, 3.61 [95% CI, 3.39-3.83]), inability to straighten knee (mean, 3.52 [95% CI, 3.20-3.84]), and swelling in knee (mean, 3.50 [95% CI, 2.54-4.46]) (Table 4). Regarding the most prevalent symptoms, 100% of patients reported knee stiffness later in the day and pain while going up- or downstairs, while 98% of patients reported each of the following: pain while twisting or pivoting, pain while bending the knee, pain while standing upright, and pain while walking on a flat surface (Table 5). Overall, of the 11 most severe and prevalent symptoms, 8 came from the KOOS pain items.
Most Severe Symptoms Among Patients With MMPRT a

KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear.
Most Prevalent Symptoms Among Patients With MMPRT a

KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear.
KOOS Items Related to Functional Limitations Among Patients With MMPRT
The most severe functional limitations among patients with MMPRT, ranked from most to least severe, were as follows: awareness of knee problem (mean, 4.62 [95% CI, 4.47-4.78]), difficulty jumping (mean, 4.06 [95% CI, 3.73-4.39]), difficulty twisting or pivoting (mean, 4.04 [95% CI, 3.76-4.32]), difficulty kneeling (mean, 3.98 [95% CI, 3.65-4.31]), and modification of lifestyle (mean, 3.94 [95% CI, 3.69-4.20]) (Table 6). Regarding the most prevalent functional limitations, 100% of patients reported each of the following: difficulty ascending stairs, difficulty getting in or out of the car, difficulty twisting or pivoting, awareness of knee problem, and modification of lifestyle (Table 7). The most severe functional limitations were related to the KOOS-QOL and KOOS-Sport/Rec items, and the most prevalent functional limitations were related to the KOOS-ADL and KOOS-QOL items.
Most Severe Functional Limitations Among Patients With MMPRT a

KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear; QOL, Knee-Related Quality of Life; Sport/Rec, Function in Sport and Recreation.
Most Prevalent Functional Limitations Among Patients With MMPRT a
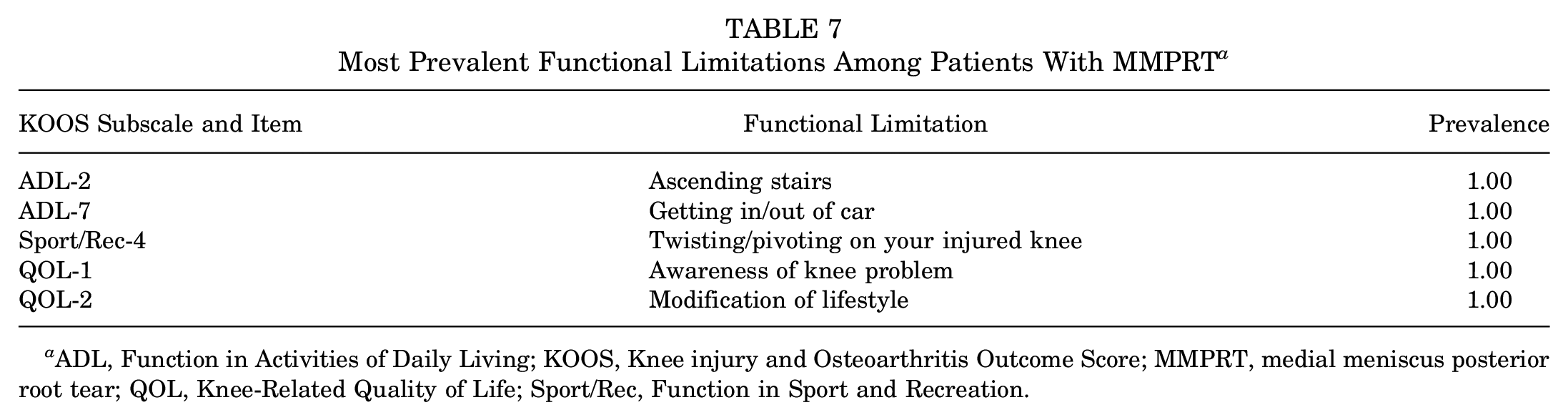
ADL, Function in Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MMPRT, medial meniscus posterior root tear; QOL, Knee-Related Quality of Life; Sport/Rec, Function in Sport and Recreation.
Discussion
In this study, we reported the most severe and prevalent symptoms and functional limitations among patients with MMPRT. The most severe symptoms were mainly related to pain, including knee pain in general (mean, 3.92 [95% CI, 3.67-4.18]), pain while twisting or pivoting (mean, 3.63 [95% CI, 3.35-3.91]), and pain while climbing stairs (mean, 3.61 [95% CI, 3.39-3.83]). The most prevalent symptoms were also mainly related to pain, with 100% of patients reporting pain while going up- or downstairs and 98% of patients reporting pain while twisting or pivoting, pain while bending the knee, pain while standing upright, and pain while walking on a flat surface. The most severe functional limitations were related to sports and recreation and quality of life, including awareness of knee problem (mean, 4.62 [95% CI, 4.47-4.78]), difficulty jumping (mean, 4.06 [95% CI, 3.73-4.39]), difficulty twisting or pivoting (mean, 4.04 [95% CI, 3.76-4.32]), difficulty kneeling (mean, 3.98 [95% CI, 3.65-4.31]), and modification of lifestyle (mean, 3.94 [95% CI, 3.69-4.20]). The most prevalent functional limitations were related to activities of daily living and quality of life, with 100% of patients reporting difficulty ascending stairs, difficulty getting in or out of the car, difficulty twisting or pivoting, awareness of knee problem, and modification of lifestyle. Symptoms and functional limitations from all 42 items of the KOOS questionnaire were seen in at least 75% of patients.
Early diagnosis of MMPRT is important given its well-known biomechanical consequences. The meniscus has a unique structure, imparting hoop strain resistance that allows it to act as a shock absorber in the tibiofemoral joint. Tears of the posterior root disrupt meniscal hoop strain resistance and render the meniscus functionless.1,27 As a result of these consequences, MMPRT has been associated with the development of marrow edema, osteonecrosis, and osteoarthritis.19,31,37,40-42 For most patients, operative repair is preferable to nonoperative care, can restore meniscal function, and has been shown to deliver better outcomes than nonoperative treatment or partial mensicectomy.4,6,25-27,29,39
The typical presentation of patients with meniscal tears, irrespective of tear type, includes distinct joint line tenderness, effusion, and a history of mechanical symptoms, such as locking and giving way. 36 Patients also commonly report functional limitations such as difficulty climbing stairs and pain while squatting. 17 The diagnostic value of these history and physical examination findings is debated in the literature. Niu et al 28 investigated the diagnostic value of 11 knee symptoms in patients with symptomatic meniscal tears. Of the 11 symptoms, localized pain, clicking, giving way, and catching were most associated with meniscal tear. However, other studies have found limited value in history and physical examination findings in diagnosing meniscal tear. 17 Additionally, it is uncertain if there are different symptoms associated with different types of meniscal tears. Some studies have suggested that patients with MMPRT have more severe pain than those with other meniscal tear types.15,22 However, Englund et al 11 found that the type and severity of meniscal tears do not correlate with the patient symptoms. As such, MRI or diagnostic MRI is typically needed to confirm the specific diagnosis and distinguish between tear types.
The KOOS is a valid and reliable tool for reporting outcomes of knee injuries.3,7,8,10,12,13,21,32-34 Among patients with MMPRT at the time of initial evaluation, we reported mean KOOS summary subscale scores between 25.0 and 25.6 for the Sport/Rec and QOL subscales and 46.3 to 51.7 for the Pain, Symptoms, and ADL subscales. In a retrospective chart review of 47 patients with MMPRT, Kodama et al 24 reported a similar range and trend of mean KOOS summary subscale scores (54.4 ± 23.5 [Pain], 64.1 ± 20.4 [Symptoms], 66.1 ± 18.4 [ADL], 25.1 ± 22.4 [Sport/Rec], and 31.2 ± 18.3 [QOL]). Baldwin et al 2 performed an observational study of 1000 healthy individuals stratified by age. For women in the 50- to 59-year age-group, mean KOOS summary subscale scores ranged from 83.1 to 97.6. While we did not include a direct comparison with healthy individuals in the current study, our patients with MMPRT appeared to have more severe mean KOOS summary subscale scores than those reported in the literature for the general healthy population. Further studies should be conducted to directly compare mean KOOS summary subscale scores in healthy individuals versus patients with MMPRT.
Baseline KOOS summary subscale scores have also been reported for patients with medial meniscal tears, irrespective of tear type. In a retrospective study of 100 patients with isolated medial meniscal tears, Ebrahimi et al 9 reported mean KOOS summary subscales ranging from 21.50 to 58.40 (56.39 ± 20.67 [Symptoms], 52.08 ± 19.41 [Pain], 58.40 ± 19.70 [ADL], 21.50 ± 21.72 [Sport/Rec], and 28.94 ± 19.68 [QOL]). However, these values vary in the literature. For example, Skou et al 35 reported similar summary subscale scores for patients with meniscal tears, while Hare et al 16 reported less severe summary subscale scores for patients with meniscal tears. We did not include a direct comparison of mean KOOS summary subscale scores for MMPRT versus other meniscal tear types. Further studies should be conducted to investigate potential differences between tear types.
Skou et al 35 used item-specific KOOS responses to describe the individual symptoms seen in 641 patients with meniscal tears, irrespective of tear type. Of the top 10 most prevalent items reported by Skou et al for patients with meniscal tear, 6 were also included in the top 10 most prevalent items for patients with MMPRT in the current study: awareness of knee problem (patients with meniscal tear vs patients with MMPRT: 99% vs 100%), difficulty twisting or pivoting (98% vs 100%), pain while twisting or pivoting (96% vs 98%), pain while going up- or downstairs (92% vs 100%), difficulty bending to the floor (97% vs 98%), and pain while bending the knee fully (89% vs 98%). The remaining 4 of the top 10 symptoms from Skou et al were not ranked as high in our patients with MMPRT but had similar absolute prevalence rates (88%-98% for patients with meniscal tear vs 87%-96% for patients with MMPRT). For example, we reported a similar prevalence to Skou et al regarding grinding/clicking noise, a symptom commonly associated with meniscal tears, even though it was not in our top 10 (88% for patients with a meniscal tear vs 87% for patients with MMPRT). When compared with the patients from Skou et al, the patients with MMPRT in our study more commonly reported other symptoms, such as knee stiffness later in the day (100%) and knee stiffness in the morning (96%).
Many of the most prevalent symptoms that we reported are less specific to meniscal tears and can be seen in many knee pathologies. Numerous studies in the literature have found that patients with meniscal tears commonly report symptoms associated with osteoarthritis.16,18,30,38 Further studies should be performed to determine whether these nonspecific symptoms are unique to MMPRT injury or a result of underlying knee pathologies.
Limitations
Our study is not without limitations. First, we did not include a direct comparison with healthy individuals or patients with other types of meniscal tears, making it challenging to draw specific conclusions about the extent to which patients with MMPRT are different from these populations. Our study was also limited by the lack of follow-up data from patients undergoing meniscal root repair. In future studies, it would be interesting to compare item-specific KOOS responses over time to see how item-specific responses change based on treatment method. In addition, we did not include information about the osteoarthritis severity of the patients. This makes it challenging to determine which symptoms are specific to meniscal tears and which symptoms are related to underlying osteoarthritis. Additionally, our study may be limited by the ceiling effect, with many items having a prevalence near 100%. Lastly, our study was limited by its small sample size. Multicenter follow-up studies should be performed to better assess the symptoms experienced by patients with MMPRT.
Conclusion
The findings of this study provide insight to physicians about the symptoms and functional limitations that they should expect in patients with MMPRT. Pain should be considered as one of the defining symptoms of MMPRT, as item-specific responses from the KOOS pain subscale made up a majority of the most severe and most prevalent symptoms. Notably however, meniscal symptoms commonly seen in other tear types, such as clicking and knee stiffness, were still quite prevalent in patients with MMPRT.
Footnotes
Final revision submitted August 1, 2023; accepted September 6, 2023.
The authors have declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the State University of New York at Buffalo (ref No. STUDY00006455).