
Abstract
Background:
The medial knee structures have a primary role in stabilizing valgus and rotational stress, which makes them important in assessing the ligament-injured knee globally and choosing the most adequate treatment.
Purpose:
To conduct a layer-by-layer dissection of the knee’s anteromedial side and provide a qualitative and quantitative description of the anatomy and histology of a ligament in the anteromedial region of the knee, which we have termed the anterior oblique ligament (AOL). Also, to describe the AOL relationship with what we have termed the medial cross—a ligament complex that stabilizes the medial pivot.
Study Design:
Descriptive laboratory study.
Methods:
A total of 35 fresh-frozen knees from transfemoral amputations that were exclusively performed for vascular reasons were dissected. Structures were identified after meticulous dissection, respecting the same protocol, measured with a digital caliper rule, and histologically studied for data.
Results:
The AOL was found in all dissected knees, with a mean length of 31.47 ± 5.06 mm. This structure presented a ligament histology with densely organized collagen fibrils. The medial cross was represented by the superficial medial collateral ligament, AOL (anterior region), and posterior oblique ligament.
Conclusion:
This study demonstrated the presence of a ligament in the anteromedial region of the knee, termed the AOL. This structure was in the anterior part of a ligament complex—the medial cross.
Clinical Relevance:
Studying and revisiting the medial compartment can provide important information for understanding joint instability and promoting better results in ligament reconstructions.
The medial knee structures have a primary role in the stabilization of valgus stress and rotational stress, making them important in the global assessment of the ligament-injured knee and choosing the most adequate treatment. The medial collateral ligament (MCL) is the most commonly injured knee ligament. 8 However, the importance given to the anatomic study of these structures has been small compared with the lateral portion, which may be explained by the fact that the MCL has a significant postinjury healing potential.10,16 However, interest in the medial knee region has recently increased. In the presence of unaddressed MCL laxity, the failure rate of anterior cruciate ligament (ACL) grafts can increase by 13 times after primary ACL reconstruction (ACLR) and 17 times after revision ACLR. 1 Why not consider the medial side when increasing extra-articular procedures concomitant to ACLRs?
The first anatomic description of the knee medial side was published in 1979 by Warren and Marshall. 17 This study divided the medial dissection into 3 layers. Layer 1 consists of the crural fascia, from the patella to the popliteal fossa and including the sartorius fascia. The gracilis tendon and semitendinosus tendon can be found between layers 1 and 2. Layer 2 consists of the superficial MCL (sMCL), and layer 3 is the articular capsule and the deep MCL (dMCL). In 2006, Robinson et al 14 published an anatomic study with a new 3-layer division of the knee medial portion, from anterior to posterior.
In an article published in 2007, LaPrade et al 9 argued that the simple division by layers, however adequate, may not be the best method for anatomic dissection since knowing the origins and insertions of the structures is essential to planning surgical reconstruction. This study focused on the quantitative assessment of the medial portion of the knee, which is different from previous studies that focused on a simple qualitative description. Nonetheless, the anteromedial quadrant was shown as an almost empty space, with no ligament structures but the anterior sMCL fibers. Two studies have described ligament structures on the anteromedial quadrant, dMCL, 1 and patellar retinaculum. 12
In our previous 2021 and 2022 studies, we have described what we term the anterior oblique ligament (AOL) in the anteromedial region of the knee.5,6 In the present study, we aimed to conduct a thorough and careful dissection of the knee anteromedial side and provide a qualitative and quantitative description of the anatomy and histology of the AOL. We also described the AOL relationship with what we have termed the medial cross—a ligament complex that stabilizes the medial pivot.
Methods
The research ethics committee of our institution approved the protocol for this study. Included were 35 fresh-frozen knees that were donated to our anatomy department between April 2020 and November 2022 after transfemoral amputations that were performed exclusively for vascular reasons and with no signs or indication of trauma. The following exclusion criteria were applied: signs of trauma, previous surgery, macroscopic signs of osteoarthritis, and poor state of preservation.
The dissection, cutting, and taking of all measurements were performed by the same orthopaedic surgeon (P.B.J.) who specializes in knee surgery and acts as a senior consultant, and the other authors participated in the dissections in different cases with him. The histological analyses were performed in the institution's pathology department and made by the same independent pathologist. The specimens were photographed by a 12-megapixel digital camera and measured with a 0.01-mm precision digital caliper rule (Mitutoyo). All measurements were reported as means and standard deviations.
Dissection Technique
The knee specimens were thawed for 24 hours at room temperature before anatomic dissection. The dissections were performed 2 to 21 days (mean, 11.65 ± 5.39 days) after the amputation. Systematically, all knee specimens were submitted for a thorough and careful dissection to identify the knee medial structures.
A hockey stick-shaped incision was made to gain the medial access, with the knee flexed at 45°, starting at the femoral shaft, bending at the medial epicondyle, and finishing at the tibial shaft (Figure 1A). Next, the entire subcutaneous tissue was carefully dissected from the knee anterior region to the popliteal fossa, exposing the fatty tissue that surrounds the posterior structures, a thin and adhered medial fascia, and the medial oblique vastus muscle (Figure 1B). The medial epicondyle was identified and marked (blue pin in Figure 1C). From there, the medial fascia opening was made in a longitudinal direction, followed by careful anterior and posterior dissection, avoiding damage to the deeper structures. As described in our previous study, 6 this fascia is a delicate tissue covering the deeper structures attached to the bone tissue and often with the deeper structures strongly adhered to it. It can be identified from the level of the distal femur to the topography of the sMCL distal attachment.
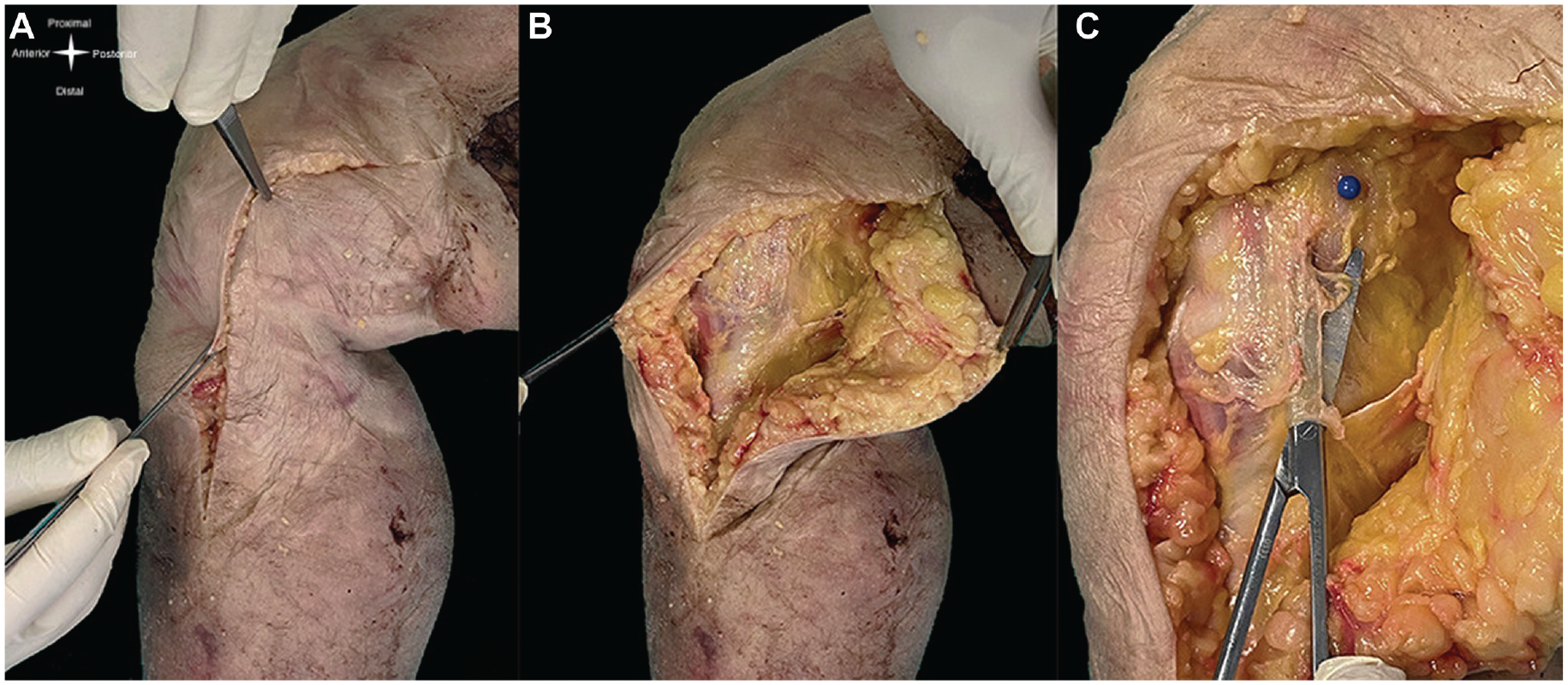
(A) Medial hockey stick incision. (B) Subcutaneous tissue dissection from the knee anterior region to the popliteal fossa. (C) Careful opening of medial osseous fascia. The blue pin marks the medial epicondyle.
Better identification of the medial structures was possible after opening and dissecting the entire fascia. At that point, the transition of palpable thickness tissue on the anterior and posterior joint line was marked (green pins in Figure 2A), representing the anterior edge of the AOL and the posterior edge of the posterior oblique ligament (POL). The palpation of the difference in thickness between tissues facilitated the identification of structures. It was not difficult to differentiate the thicker tissues (ie, the ligaments) from the joint capsule. The distal MCL attachment was identified distally to the insertions of the semitendinosus and gracilis tendons (blue pins in Figure 2A). These 4 structures marked what we termed the medial cross. The dissection continued in a posterior direction. By carefully removing the adipose tissue that was strongly adhered to the deep structures, it was possible to identify the semimembranosus tendon inserted in the tibia. Next, we carefully dissected the POL portion that was placed on it (orange pin in Figure 2B).
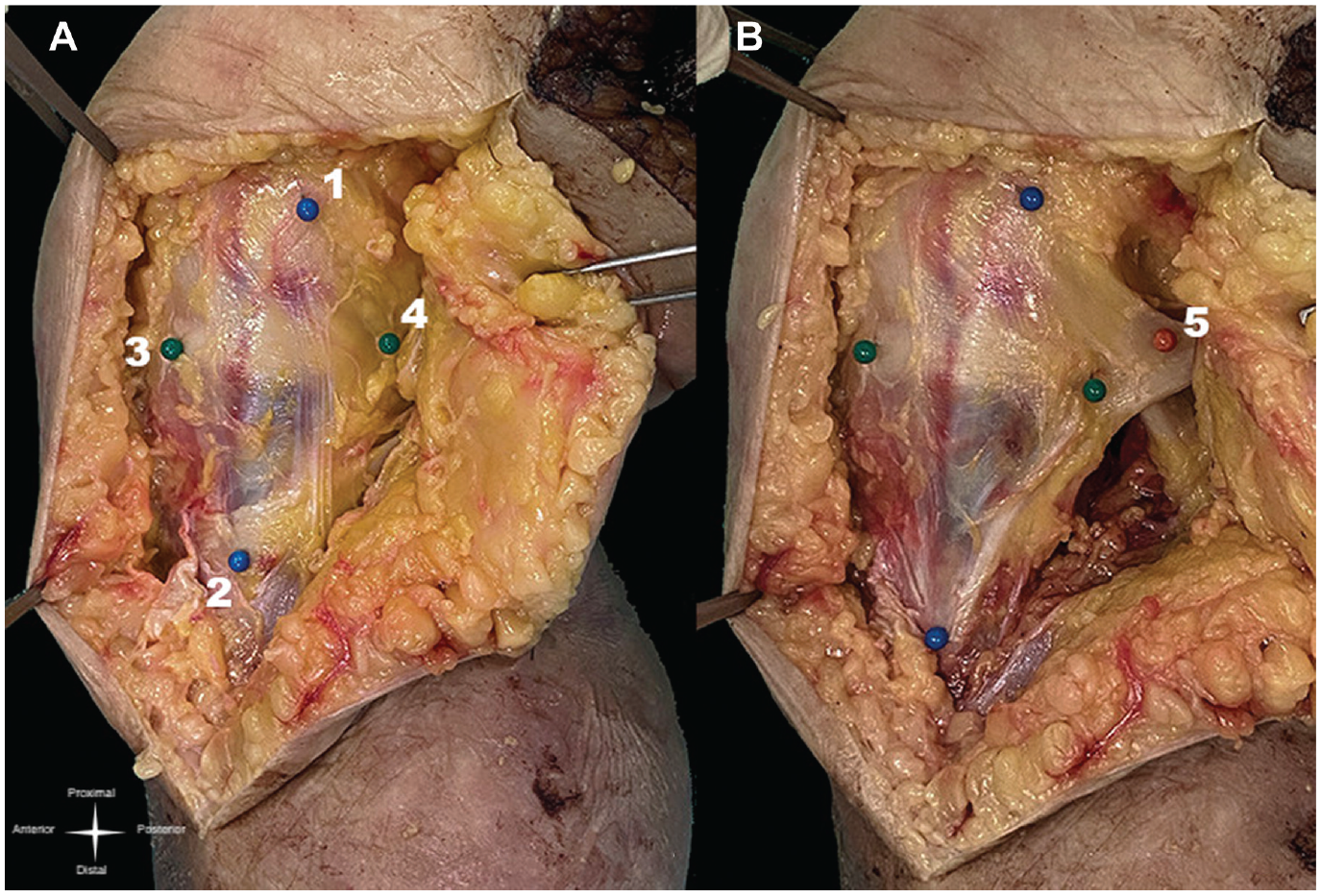
(A) The medial cross, with the 4 pins marking its limits: 1, medial epicondyle; 2, distal sMCL at its tibial insertion; 3, visible and palpable anterior border of the AOL at its tibial insertion; and 4, visible and palpable posterior border of the POL at its tibial insertion. (B) The medial cross with the POL dissected (orange pin); 5, semimembranosus insertion of the POL. AOL, anterior oblique ligament; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
Next, we detached the sMCL from the tibia from distal to proximal direction. Its distal tibial insertion was firm and wide. At this moment, a new scalpel blade was used, facilitating the structure's release. When the entire distal tibial insertion loosened, the ligament was proximally separated from the bone by a soft areolar connective tissue as a bursa. 6 Proximal to this bursa, and just anterior to the tibial insertion of the semimembranosus tendon, there was a bony prominence—a bony tubercle 6 (Figure 3).

Medial view of the knee after deep dissection. 1, sMCL dissected and reflected proximally; 2, bone tubercle (just anterior to the tibial insertion of the semimembranosus); 3, bursa; 4, distal tibial insertion of the sMCL; and 5, tibial insertion of the semimembranosus. The green and orange pins mark the same structures as in Figure 2. sMCL, superficial medial collateral ligament.
Dissection of the sMCL continued proximally. The less firm and smaller proximal tibial insertion of the MCL was located just above this tubercle. Proceeding proximally, it was possible to gently separate the superficial ligament from the dMCL. Combining visual identification with palpation, the anterior and posterior borders of the dMCL were marked (blue pins in Figure 4).

Medial view of the knee after deep dissection and marking the dMCL. 1, sMCL dissected and reflected proximally; 2, dMCL; 3, visible and palpable anterior border of the AOL at its tibial insertion; 4, visible and palpable posterior border of the POL at its tibial insertion; and 5, visible and palpable anterior and posterior borders of the dMCL. AOL, anterior oblique ligament; dMCL, deep medial collateral ligament; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
From then on, it was evident that the AOL existed as an anterior and superficial structure to the dMCL. Originating from the medial epicondyle, the AOL ran distally in an oblique direction to the tibia upper border where it was inserted. The anterior green pin was removed, and the tibial insertion of the AOL was marked (2 orange pins in Figure 5). The AOL could easily be separated from the joint capsule (Figure 6). Regarding the present study, the measures were limited to the AOL (length, femoral origin width, tibial insertion width, and the distance between the tibial insertion center of the AOL and the anterior edge of the sMCL) and were made in this point of the dissection.

Medial view of the knee after deep dissection, marking the dMCL and dissecting the AOL. 1, AOL; 2, visible and palpable anterior and posterior borders of the AOL at its tibial insertion; 3, dMCL; and 4, visible and palpable anterior and posterior borders of the dMCL. AOL, anterior oblique ligament; dMCL, deep medial collateral ligament.

Photograph of the knee from the side showing a space between the AOL and joint capsule. 1, AOL; and 2, intact articular capsule. The orange and blue pins mark the same structures as in Figure 5. AOL, anterior oblique ligament.
After identifying all the structures and measuring sizes and distances, 23 of the knees studied were cut into blocks, preserving their bone origin and insertion (Figure 7). They were then sent to the histology department, which evaluated their microscopic structure. The structure identified as the AOL was fixed in 10% formalin overnight, serially dehydrated in a graded ethanol series, embedded in paraffin, and sectioned longitudinally at 4-μm thickness. Histological sections were stained with hematoxylin and eosin for histological analysis by the same pathologist.

Block-cut piece for histological analysis. 1, sMCL dissected and reflected proximally; 2, AOL; 3, dMCL; and 4, soft tissue (articular capsule). AOL, anterior oblique ligament; dMCL, deep medial collateral ligament; sMCL, superficial medial collateral ligament.
Results
Qualitative and Quantitative Approach
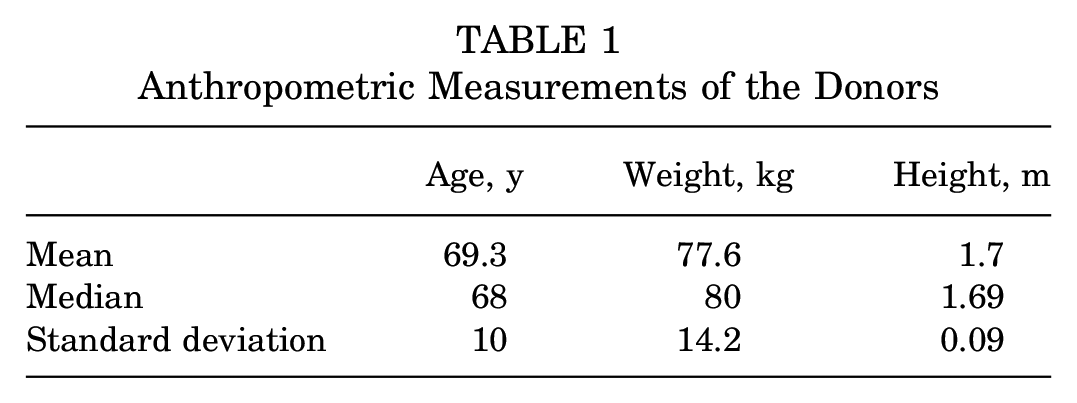
There were 13 female and 22 male specimens, with a mean age of 69.28 ± 10.07 years. The anthropometric measures of the donors are described in Table 1.
Anthropometric Measurements of the Donors
The AOL was found to be a superficial structure in all specimens on the anteromedial side of the knee. It was an extracapsular structure and could be distinguished easily from the sMCL, dMCL, articular capsule, and medial patellofemoral ligament (Figure 8).

The medial patellofemoral ligament. The orange and blue pins mark the same structures as in Figure 5.
The medial dissection is not a simple procedure; an abundance of fat tissue and adherence makes it difficult. Initially, a wide access route is important, with a complete subcutaneous tissue dissection, from the anterior region to the popliteal fossa, which is what we consider the most superficial layer of the medial dissection. After this, it is possible to identify the medial fascia that covers the deeper structures attached to the bone and fatty tissue that surrounds the posterior structures. The fascia opening and fat tissue cleaning must be performed carefully to observe the ligaments and tendinous structures better. The medial cross (represented by the sMCL, AOL anterior edge, and POL posterior edge) can be identified (see Figure 2A). The gracilis tendon and semitendinosus tendon can be found at this time, crossing the sMCL distal third superficially. Under the fascia are the ligamentous structures, over the bones, represented by the sMCL, POL, and AOL. When the sMCL is completely released, from distal to proximal, it is possible to identify the dMCL and articular capsule.
The femoral attachment of the AOL is at the medial epicondyle anterior portion. In 28 of the 35 specimens dissected, the ligament origin could be individualized from the origin of the sMCL in a most superficial and anterior topography. The proximal attachment of the AOL and the sMCL could not be individualized in 7 cases.
The AOL tibial attachment—thicker than the femoral origin in anteroposterior orientation—is located immediately distal to the tibial plateau. The ligament is fan-shaped, and its tibial insertion is separated from the sMCL anterior edge. When we look at the medial cross as a set of ligament stabilizers in the knee medial region, its anterior arm is represented by the AOL. The mean length (proximal to distal) of the AOL was 31.47 ± 5.06 mm. The mean thickness (medial to lateral) of its femoral origin was 6.51 ± 1.03 mm, and the tibial insertion mean thickness was 12.99 ± 1.67 mm, showing the fan shape of the structure.
The AOL lies anteriorly to the sMCL, and loose connective tissue is always seen between the 2. The distance between the tibial insertion center of the AOL and the anterior edge of the sMCL was 10.29 ± 1.51 mm.
Histological Analysis
The histology of the AOL revealed a slender ligament structure with densely organized collagen fibrils. The AOL was thicker and consisted of denser and more connective tissue than the anteromedial articular capsule. The fibers were parallel-oriented and positioned slightly in undulatory-like collagen fibrils, typical of ligament structures (Figure 9). Dense connective tissue with arranged fibers and little cellular material was found in all specimens.

Histological aspect of the AOL. This longitudinal axis cut shows dense connective tissue surrounded by looser tissue superficial to the AOL. AOL, anterior oblique ligament.
Discussion
This study established the anatomic landmarks of a ligament in the anteromedial region of the knee that we have termed the AOL.5,6 The AOL was observed in 100% of the dissections, and its histological analysis was compatible with ligament tissue. This line of research can be of great importance, considering that the results of ACLR must be improved. To the extent that, since the anterolateral ligament was revisited3,4 in 2013, extra-articular reinforcement has become a matter of great interest and the path to better outcomes after ACLR seems to be clearer.11,13,15 By studying and understanding the medial compartment better, we may achieve better results in central pivot reconstructions, as occurred in the study of the lateral compartment.
According to the theory of the tibial quadrants, elaborated and published by our author group, 5 which discusses the rotational and angular control promoted by the peripheral ligaments of the knee, the valgus and knee external rotation are controlled by the anteromedial quadrant. It may be that in patients with ACL lesions and mild medial instability, in patients without high-grade pivot shift, and in those with trauma in valgus and external rotation, a medial extra-articular reinforcement could be better indicated. Patients with ACL injury in our study group received ACLR and reinforcement in the AOL topography using the surgical technique already described in the literature. 7
Interest in the anatomy of the knee medial region is increasing. In 2022, Peez et al 12 published a qualitative and quantitative assessment of the anatomy of the medial patellar retinaculum. They reported that the medial patellar retinaculum extends from the medial patellofemoral ligament to the sMCL anterior edge, inserting distally at the tibia, almost 30 mm below the articular surface. We believe that there are 2 distinct ligamentous structures: the medial patellofemoral ligament and the AOL (Figure 8). In our study, the AOL was found in all knees, and it had a similar length, width, and thickness measurements in all specimens. The attachment of the ligament to the medial epicondyle region was similar in all dissected knees. The AOL from the 35 dissected knees, while presenting minor variations, had a femoral attachment that was anterior to the sMCL origin. From here, the AOL runs distally and obliquely toward the tibia. When crossing the joint, it was always possible to separate it from the joint capsule. The AOL tibial insertion is thicker than its femoral origin. On the tibia, the ligament inserts just below the joint line, anterior to the sMCL anterior border, and is separated from this ligament by clearly looser tissue (Figure 7).
The reinforcement of the knee anteromedial quadrant has recently attracted greater interest. In an in vitro series, Miyaji et al 10 demonstrated that sMCL reconstruction, associated with what they called dMCL reconstruction, in a similar topography of the AOL, was beneficial in controlling anteromedial rotatory instability, which is a cause of ACLR failures. In another in vitro series, Behrendt et al 2 demonstrated better control of anteromedial rotatory instability when sMCL reconstruction was performed associated with ligament reinforcement in the anteromedial compartment, exactly in the topography where the AOL is found, which biomechanically demonstrates the assertiveness of the tibial quadrant theory, 5 and which may be important in some specific cases of ACL insufficiency associated with subtle medial and rotational instability.
We believe that achieving complete medial stability reestablishment is one of the essential factors for improving outcomes in ligament injuries. The knee medial region is inherently more stable than the lateral region, thanks to the bony anatomy and ligament portion. The cross shape of the medial peripheral ligaments (the medial cross) contributes to this stability, and the AOL is anatomically located in an important quadrant for valgus and external rotation control. The histological analysis confirmed that the AOL ligamentous nature—a thick connective tissue organized with parallel and undulatory-like orientated collagen fibrils—and the dissections showed how easy it was to separate it from the joint capsule—a looser tissue that was obviously distinct.
Limitations
There are some limitations to the present study. The main weakness of our study was the absence of a biomechanical analysis of this ligament. Our findings can serve as a guide for biomechanical studies in the future. We did not perform a sample calculation, and we described all the dissections that had been made at that point. Another weakness was the advanced age of cadaveric specimens. What these findings add as relevant data in addition to the anatomic revision is unknown. Thus, further studies on the subject are needed; nonetheless, this is an interesting start.
Conclusion
The 35 dissections reported in this study demonstrate a ligamentous structure called the AOL in the knee medial region. It originates from the anterior border of the medial epicondyle and inserts more widely under the articular surface, thus having a fan shape. It is in an extracapsular situation, not directly related to the medial meniscus, representing the anterior arm of the medial cross. Studying and revisiting the medial compartment can provide important information for understanding joint instability and promoting better results in ligament reconstructions.
Footnotes
Final revision submitted September 14, 2023; accepted October 1, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Santa Casa de Misericórdia de São Paulo (ref No. 4.251.622).