
Abstract
Background:
Little is known on how meniscal morphology develops during skeletal growth and maturation and its subsequent relationship with the corresponding bony anatomy.
Hypotheses:
(1) Meniscal dimensions and morphology would change by age during skeletal growth and maturation in different ways in boys compared with girls. (2) Morphological features of the medial and lateral menisci would correlate to medial and lateral femoral condyle curvatures.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Anatomic features of the medial and lateral menisci were measured on magnetic resonance imaging scans from 269 unique knees (age, 3-18 years; 51% female) with no prior history of injury, congenital or growth-related skeletal disorders, or bony deformities. Morphological shape-based measurements were normalized to tibial plateau width or determined as ratios of meniscal dimensions. The association between age and anatomy was analyzed with linear regression. Two-way analysis of variance with the Holm-Šídák post hoc method was used to compare anatomy between sexes in different age groups. Linear regression was used to evaluate the relationship between femoral condyle curvature radius and meniscal morphology in each compartment after adjusting for age and sex.
Results:
Meniscal length, width, horn distance, mean cross-sectional area (CSA), and mean height increased with age in both sexes (R2 > 0.1; P < .001). Age-related changes in meniscal morphology were seen in normalized length, width, horn distance, and mean height; width-to-length ratio; horn distance-to-length ratio (lateral meniscus only); normalized mean CSA (except lateral meniscus in girls); and mean tip angle (R2 > 0.04; P < .02). Sex-based differences were also found, with some morphological differences (normalized length and height) throughout development (P < .03) and size differences (length, width, and mean CSA) in later development (P < .01). After adjusting for age and sex, there were significant correlations between medial condyle curvature radius and normalized width, width-to-length ratio, horn distance, horn distance-to-length ratio, mean CSA, and mean height of the medial meniscus (P≤ .041) and between lateral condyle curvature radius and normalized length, mean height, and mean tip angle of the lateral meniscus (P≤ .004).
Conclusion:
Age-related changes in meniscal dimensions and morphology, most notably a nonuniform growth pattern in meniscal geometry, occurred during skeletal growth and maturation, with different trends in boys than in girls.
The knee joint is the most common site of injury in children and adolescents and the largest and most complex joint in the human body.1,29,31 Menisci are among the most important knee structures, providing stability, load transmission, shock absorption, joint nutrition, and lubrication. 10 Their unique and complex morphology directly influences their function, 38 namely acting to redistribute the contact forces passing through the tibiofemoral joint. 41 Previous investigations have demonstrated that at least 50% of axial forces are distributed through the menisci during extension and 85% during flexion,21,23,37 highlighting the importance of menisci in knee loading. Menisci are prone to injury, especially in young active individuals, and lateral meniscal tears are more prevalent in this population. 28 The pattern and prevalence of injury have been shown to be age and sex related, with males at a higher risk of injury and incidence peaking at an age of 20 to 29 years for both sexes.9,18,26,28 Meniscal geometry has also been shown to influence the risk of anterior cruciate ligament injury and osteoarthritis.20,24 While the current literature on meniscal morphology is mainly focused on meniscal sizing in adult knees to guide implant design and selection,3,34,36 little is known on meniscal morphology development during skeletal growth and maturation; having this knowledge may help us to better understand meniscal function.
The menisci are formed in the knee joint between the 8th and 10th weeks of embryonic life. Several longitudinal studies have documented the development of the menisci in nonhuman vertebrate knees, largely focusing on these prenatal embryological origins. Clark and Ogden 6 were the first to document the development of the meniscus in human knees before skeletal maturity, with a collection of harvested menisci ranging from 14 weeks’ gestation prenatally to 14 years of age postnatally. They found that after birth, the most profound changes that occurred were a gradual devascularization of the meniscus, coupled with a significant increase in the intercellular matrix content of the menisci. Fibrocartilage was not found in specimens prenatally, consistent with the theory that fibrocartilage production occurs as a response to loading with the onset of weightbearing. They also showed that the ratio of meniscal surface area to the corresponding tibial plateau remained consistent throughout all stages of growth, both pre- and postnatally, suggesting a close relationship between menisci and bony development.
Traumatic meniscal injuries are increasing in children and young adults,39,40 and with the development of newer, more advanced invasive and noninvasive imaging techniques, other meniscal pathologies such as discoid menisci are being diagnosed more readily. As such, understanding the morphologic development of these intra-articular structures and the corresponding relationship to the surrounding bony anatomy is becoming an important supplement to improve treatment and diagnosis of musculoskeletal pathologies. The aim of this study was to map the age- and sex-dependent changes in meniscal dimensions and morphology during skeletal growth and maturation. We hypothesized that meniscal dimensions (i.e., length, width, horn distance, mean cross-sectional area [CSA], and mean height) and morphology (i.e., width-to-length ratio, horn distance-to-length ratio, tip angle and normalized length, width, mean CSA, horn distance, and mean height) would change by age during skeletal growth and maturation in different ways in boys compared with girls. Additionally, we hypothesized that morphological features of the medial and lateral menisci would correlate to medial and lateral femoral condyle curvatures.
Methods
Study Population
After receiving institutional review board approval for the study protocol, we reviewed the medical and imaging records of all patients ≤18 years of age who visited the orthopaedics or sports medicine clinics of our institute between 2011 and 2015 and had undergone knee magnetic resonance imaging (MRI) examination (N = 2,987). The primary reason for the MRI study was to assess soft tissue injury after an event. The clinical notes as well as radiology reports for each patient were reviewed. A waiver of informed consent for the use of reviewing this data retrospectively was approved by the institutional review board. Patients were excluded if they had prior knee injuries (including meniscal pathology), congenital or growth-related skeletal disorders, bony deformities, fractures of the tibial plateau or femoral condyles, or knee cartilage damage (635 patients were excluded). From the 2,352 eligible patients, we randomly selected up to 10 boys and 10 girls for each age using an unbiased random number generator, leading to 269 unique knees (age, 3-18 years; 51% female). Patients were selected in a manner to ensure equal distribution across each age. The same cohort has been used previously to study age- and sex-related changes in the anterior cruciate ligament and its anatomic risk factors.14,15
Imaging Analysis
Three-dimensional (3D) MRI stacks of the knee joint (SAG PD SPACE sequence with 1.5-mm slice thickness; Siemens) were used to measure the anatomic features of the medial and lateral menisci as shown in Figure 1, following established techniques described in the literature. Despite variations in image acquisition parameters over the years, all included MRI scans had sufficient resolution for accurate anatomic measurements. Thus, the reported anatomic measurements are not affected by those imaging variations. Raters were blinded to the patients’ sex and age and completed measurements using a commercial image viewer (Osirix Viewer; Pixemo SARL). Measurements were reported in millimeters and degrees. To assess the reliability of the measurements, the same examiner (A.M.K.) who did the initial measurements repeated these on a subset of randomly selected 20 samples, which was also measured by another independent examiner (S.H.). The intraclass correlation coefficients (ICCs) were calculated for interrater and intrarater reproducibility and reliability of the measurements (ICC > 0.7 for all measurements).

Measurement techniques used to quantify meniscal length (ML), meniscal width (MW), and meniscal horn distance (MHD); anterior and posterior meniscal cross-sectional area (ACSA and PCSA); anterior and posterior meniscal height (AMH and PMH) and anterior and posterior meniscal tip angle (α and β); femoral condyle curvature radius (FCR); and tibial plateau width (TPW). Separate measurements were performed for medial and lateral menisci.
Meniscal Length and Width
An oblique axial slice covering the full meniscus was used to measure meniscal length as the vertical (anterior-posterior) distance between the anterior peripheral wall and posterior peripheral wall of the meniscus approximately in the center of the compartment in the medial-lateral direction. Care was taken to ensure this measurement was taken at the peripheries of each wall (ML in Figure 1).19,34 The same oblique axial slice was also used to measure meniscal width as the horizontal distance from the outer edge of the meniscus (the most lateral point for the lateral meniscus or the most medial point for the medial meniscus) and the middle of the meniscal horns, as measured from the center of the line used to measure horn distance (MW in Figure 1).19,34
Meniscal Horn Distance
The same oblique axial slice used above was used to measure meniscal horn distance as the length of the straight line connecting the central aspects of anterior and posterior meniscal horn. These central points were identified by the examiner after outlining the contour of the meniscus in the same image (MHD in Figure 1).
Meniscal Mean CSA
A sagittal slice corresponding to the center of the medial or lateral compartment was used to measure the anterior and posterior CSA of the meniscus, by outlining its cross section. The sagittal slice location was visually confirmed to be in the approximate center of each compartment in the coronal view.12,13,15 The anterior and posterior measurements were then averaged to calculate the mean CSA (ACSA and PCSA in Figure 1). 17
Meniscal Mean Height
The same sagittal slice used above was used to measure meniscal height in the anterior and posterior regions. 17 The anterior and posterior measurements were then averaged to calculate mean height (AMH and PMH in Figure 1).
Meniscal Mean Tip Angle
The same sagittal slice was used to measure the angle of the meniscus in the anterior and posterior regions. The anterior and posterior measurements were then averaged to calculate mean tip angle (α and β in Figure 1). 17
Femoral Condyle Curvature Radius
The same sagittal slice was used to measure the femoral condyle curvature radius as the radius of the best-fit circle to the posterior aspect of the femoral condyle in the medial and lateral compartments (FCR in Figure 1). 7
Tibial Plateau Width
The coronal slice passing through the center of the knee was used to measure the tibial plateau width as the horizontal distance between the medial and lateral aspects of the plateau. The coronal slice location was visually confirmed to be in the approximate center of the knee in the sagittal view (TPW in Figure 1).12,13,15
Statistical Analysis
Age and all measured anatomic variables were defined as continuous. We also assessed meniscal morphology, independent of its sizing. To do this, we calculated the meniscal length-to-width ratio and the horn distance-to-length ratio. Additionally, we normalized the meniscal mean height, mean CSA, width, and length to the patients’ tibial plateau width. This normalization to tibial plateau width has been performed in previous studies because of the strong correlation between tibial plateau width and meniscal dimensions.2,5,34 Linear regression was used to assess the age-related changes in quantified anatomic and morphological features of the menisci. Separate analyses were done for boys and girls. To further evaluate sex differences at different ages, patients were classified into eight subgroups (four age groups for each sex), based on the following age ranges: preschool aged (3-6 years), prepubertal school aged (7-10 years), early adolescents (11-14 years), and late adolescents (15-18 years). 22 A 2-way analysis of variance (ANOVA) was used to evaluate the effects of age and sex on quantified features of the meniscus for the aforementioned eight subgroups. For these analyses, the anatomic parameters and age were defined as continuous variables, and sex was defined as a categorical and dichotomous variable. Quantified anatomic indices at each age group were compared between girls and boys by using the same ANOVA model (four pairwise comparisons). P values of all four pairwise comparisons were then adjusted based on the Holm-Šídák correction method to account for any potential increase in type 1 error because of multiple comparisons. Linear regression was also used to evaluate the associations between femoral condyle curvature radius and quantified anatomic and morphological features of the meniscus adjusting for age and sex. Separate analyses were done for the medial and lateral compartments. Analysis was done in Prism (Version 9; GraphPad Software) using α = 0.05.
Results
Age-dependent changes during skeletal growth and maturation in both medial and lateral compartments are presented in Tables 1 and 2, with meniscal dimensions and morphologic measurements presented, respectively. Meniscal dimensions refer to those measurements that indicate size of the anatomic features, while morphologic measurements refer to those that indicate shape of the anatomy (i.e., ratios, normalized measurements, and mean tip angle). Except lateral meniscal mean height (in girls), medial meniscal horn distance-to-length ratio (in both sexes), and lateral meniscal normalized mean CSA (in girls), all quantified indices changed by age (P < .02 for all associations).
Age-Dependent Changes in Meniscal Dimensions During Skeletal Growth and Maturation a

Boldface P values indicate statistical significance (P < .05). CSA, cross-sectional area.
Age-Dependent Changes in Meniscal Morphology During Skeletal Growth and Maturation a

Boldface P values indicate statistical significance (P < .05). CSA, cross-sectional area.
Normalized to the tibial plateau width.
Sex-based differences in medial and lateral menisci dimensions across different age groups are presented in Figure 2. Except for mean meniscal height, girls (15-18 years) had smaller menisci than age-matched boys (P < .01). Girls (7-10 years) also had a smaller mean medial meniscal CSA and lateral meniscal horn distance compared with age-matched boys (P < .03). No other sex-based differences were observed across quantified features.
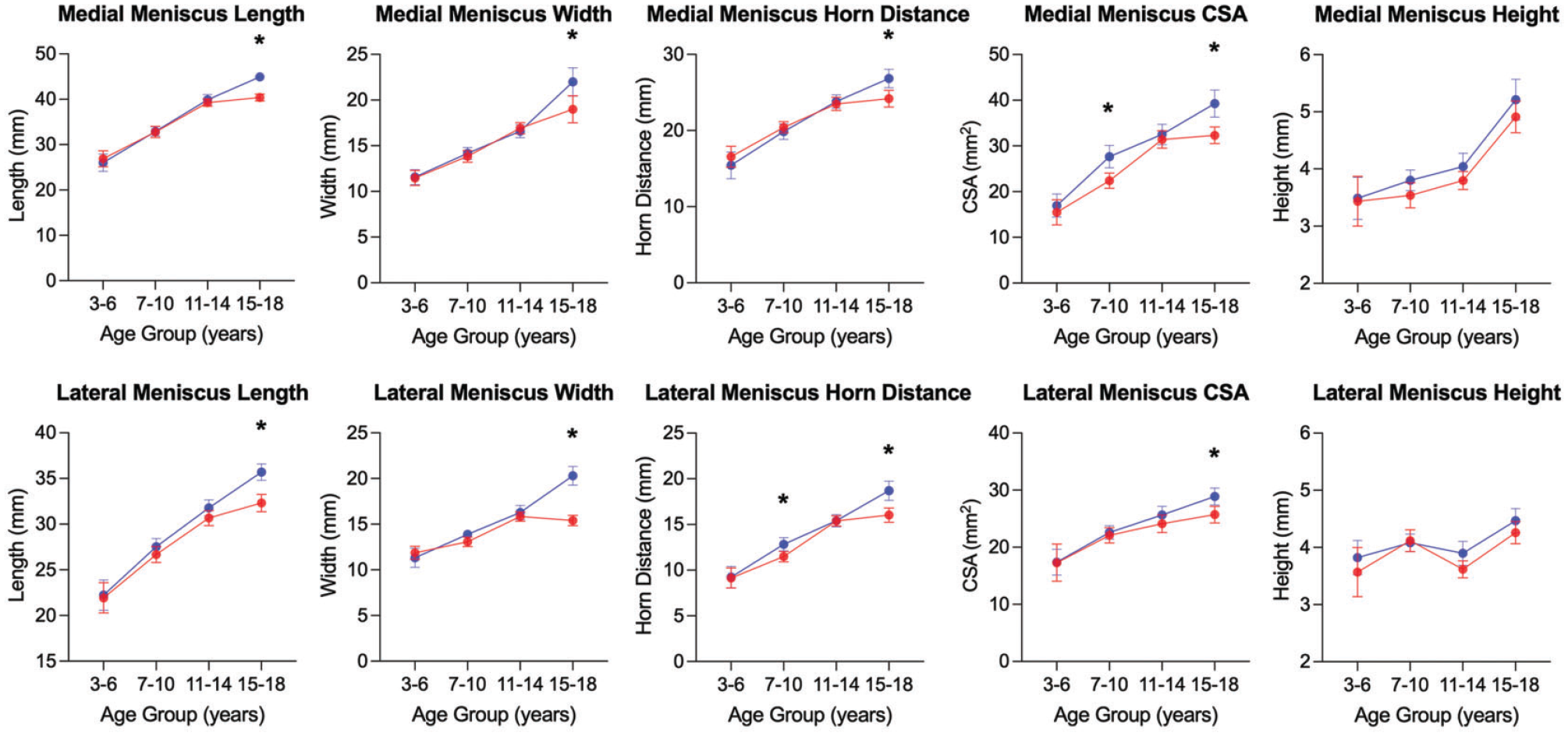
Sex-based differences in medial (top row) and lateral (bottom row) menisci dimensions during skeletal growth and maturation. Results are presented as means with error bars representing 95% CIs. *Statistically significant difference (P < .05) between boys (blue) and girls (red). CSA, cross-sectional area.
Sex-based differences in medial meniscal morphology across different age groups are presented in Figure 3. Girls had a larger normalized length (all age groups), a larger normalized horn distance (7-10 years), and a smaller mean normalized CSA (7-10 years) compared with age-matched boys (P < .04). No other sex-based differences were observed across quantified morphologic features.

Sex-based differences in medial meniscal morphology during skeletal growth and maturation. Results are presented as means with error bars representing 95% CIs. *Statistically significant difference (P < .05) between boys (blue) and girls (red). CSA, cross-sectional area.
Sex-based differences in lateral meniscal morphology across different age groups are presented in Figure 4. Girls had a smaller normalized width (15-18 years), smaller width-to-length ratio (15-18 years), and a larger normalized mean height (7-10 years and 15-18 years) compared with age-matched boys (P < .02). No other sex-based differences were observed across quantified morphologic features.

Sex-based differences in lateral meniscal morphology during skeletal growth and maturations. Results are presented as means with error bars representing 95% CIs. *Statistically significant difference (P < .05) between boys (blue) and girls (red). CSA, cross-sectional area.
Representative 3D models of meniscal cross-sectional morphology for a 6-year-old and a 17-year-old knee are shown in Figure 5, highlighting age-related changes in the cross-sectional profiles of medial and lateral menisci.
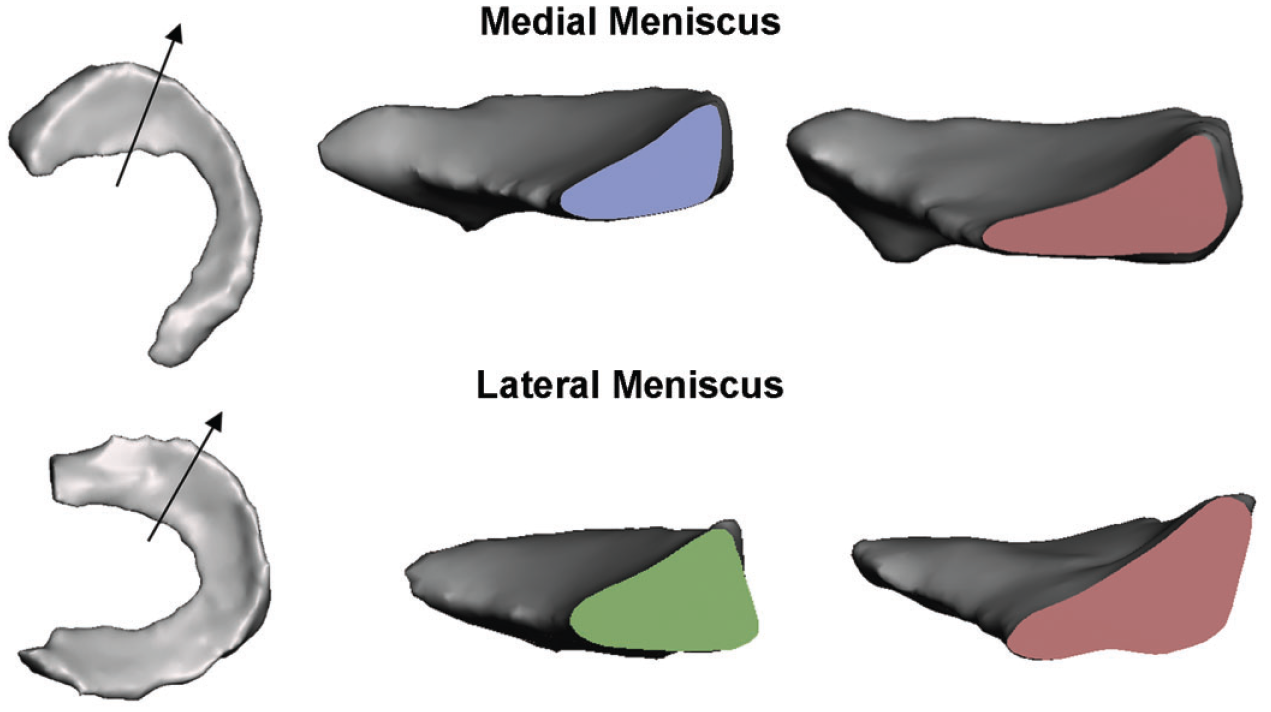
Changes in meniscal cross-sectional morphology of the medial and lateral menisci during skeletal growth and maturation. Left panel depicts cross section viewed, middle panel shows immature meniscal cross section, and right panel shows mature meniscal cross section.
Associations between both the medial femoral condyle curvature radius and medial meniscal morphology and the lateral femoral condyle curvature radius and lateral meniscal morphology adjusted for age and sex are presented in Tables 3 and 4, respectively. In the medial compartment, an increased femoral condyle curvature radius (flatter condyle) was associated with smaller normalized meniscal width (P < .001), lower meniscal width-to-length ratio (P < .001), lower meniscal horn distance-to-length ratio (P < .001), smaller mean normalized meniscal height (P = .007), and larger mean normalized meniscal CSA (P = .041). In the lateral compartment, increased femoral condyle curvature radius (flatter condyle) was associated with greater meniscal normalized length (P < .001), smaller mean normalized meniscal height (P < .001), and smaller mean meniscal tip angle (P = .004).
Associations Between Medial Femoral Condyle Curvature Radius and Medial Meniscal Morphology (n = 269) a

All predictors are presented as detailed model coefficient (β) (95% CI). All associations are adjusted for age and sex. Boldface P values indicate statistical significance (P < .05). CSA, cross-sectional area.
Normalized to the tibial plateau width.
Associations Between Lateral Femoral Condyle Curvature Radius and Lateral Meniscal Morphology (n = 269) a
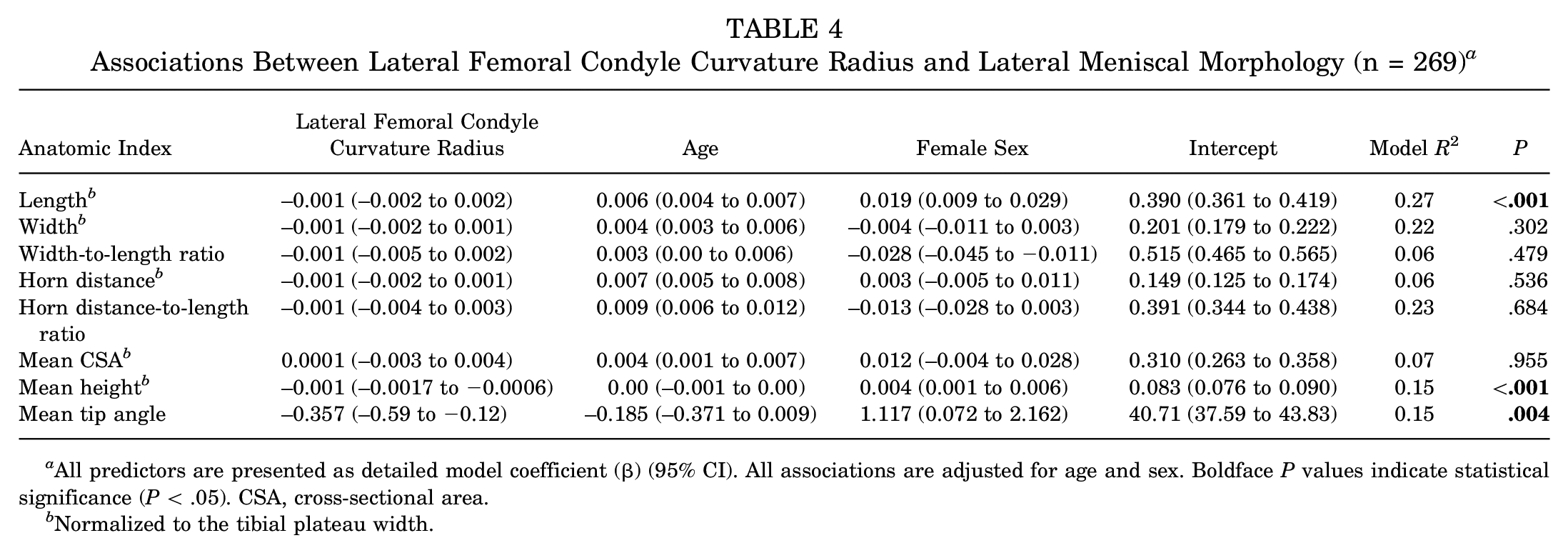
All predictors are presented as detailed model coefficient (β) (95% CI). All associations are adjusted for age and sex. Boldface P values indicate statistical significance (P < .05). CSA, cross-sectional area.
Normalized to the tibial plateau width.
Discussion
In this study, there were significant age-related changes in the majority of the measured meniscal dimensions as well as fundamental changes in the meniscal morphology during growth, with different trends observed in boys compared with girls, partially supporting our first hypothesis. Specifically, boys were found to have significantly larger menisci across all dimensions except meniscal height in the oldest age group, and differences were found in morphology throughout development in normalized length and normalized height. Meniscal morphologic trends had notable variations between the medial and lateral compartments during skeletal growth except for the mean meniscal tip angle, which decreased in both compartments. By this measure, the gross morphological change of the meniscus after the onset of weightbearing age in humans is not homogeneous in all directions and instead has a predisposition to a larger growth rate in the anterior-posterior and lateral directions compared with the superior-inferior direction, resulting in smaller mean tip angles at adolescence. Moreover, we saw notable correlations between meniscal morphology and femoral condyle curvature, primarily across the medial compartment, partially supporting our second hypothesis.
We found significant sex-based differences primarily in the later age groups for all meniscal dimension measurements other than meniscal mean height. We also found some morphologic shape differences, with girls having significantly larger normalized medial meniscal lengths across all age groups. This suggests that while size-based sex differences tend to appear later in development, shape-based morphologic sex differences tend to show trends throughout child and adolescent development. Our finding that boys have a larger medial and lateral meniscal size compared with age-matched girls (in measures of meniscal length, width, horn distance, and CSA) in middle to late adolescence is consistent with previous research, which shows that meniscal length and width are larger in men than in women.5,8,32,34 A similar cross-sectional study examining normal meniscal development throughout childhood also agreed, showing larger meniscal widths for boys after adjusting for age. 4
Our morphologic findings after normalizing to tibial plateau width differed from those of Bloecker et al, 5 who showed marginally but not significantly greater values in women than men after normalization. While Bloecker et al suggested that these normalized measures could be used as a parameter in studying mixed cohorts of men and women and their meniscal morphology, our findings disagree and suggest that there are significant shape differences throughout development between sexes. The larger normalized mean height found in girls in the lateral meniscus can potentially be explained by sex differences in condyle morphology. Mahfouz et al 25 found, by mapping condyle curvature at the most prominent contact points, that women across ethnicities have more curved femurs. Thus, a larger normalized mean height of the menisci in females can help to lessen the mismatch between the femur and meniscus. This may also help to explain why meniscal height was the only size dimension that was not significantly larger in boys in the oldest age group. Interestingly, using a statistical shape modeling approach, Vrancken et al 38 did not find sex-related shape differences in the lateral or medial menisci but noted how this opposes what would be expected given the sex-dependent differences in bony geometry. Increasingly, the literature supports sex-specific prevention and treatment protocols. Particularly with the meniscus, males have been found to be of higher risk of meniscal tears in adolescence as well as adulthood.18,26,33 The data provided here indicate that there are sex-based meniscal morphology and size differences, which can potentially help to further inform future study on these injury rate discrepancies.
The data also have potentially important implications for surgical technique in meniscal tear repair. Historically, the inside-out suture repair technique has been considered the gold standard of meniscal repair.11,27 However, with potential issues of damage to the neurovascular structures from the exiting suture needles, the paradigm has shifted to all-inside suture repair methods, which have continually grown in use and preference among surgeons.11,30 Still, despite the advantages of the all-inside method such as decreased surgical time and reduced neurovascular injury risk,11,30,35 one disadvantage to this method is the larger-diameter insertion needle required, which limits the number of sutures and fixation points. 30 The data presented here could offer important insight into the optimal choice of surgical technique specifically for younger patients, with dimensions such as meniscal height offering information on whether a larger-diameter needle is appropriate for meniscal repair. The reported data may also assist with proper selection of meniscal allografts to ensure proper size and congruency with bony structures. Future studies are required to assess how such measurements may impact surgical treatments of meniscal injuries.
Our results showed positive correlations for all dimensions with age in both medial and lateral menisci and in both sexes except for lateral and medial meniscal height in girls. This is mostly in agreement with a previous study finding of increases in all MRI-based meniscal dimensions throughout development except in the coronal meniscal width. 4 The most notable morphologic age-related changes found in this study show positive correlations with age in normalized meniscal width and normalized meniscal length but slightly negative to no correlation with age in normalized mean height and negative correlation with age in tip angle. These are indications of a heterogeneous morphological growth pattern, after controlling for normal tibial plateau growth. Specifically, meniscal shape has a larger growth rate in the anterior-posterior and lateral directions compared with the superior-inferior direction. Since an increase of meniscal width has been shown to decrease the contact stresses of the knee, 16 this type of growth would support a shift in functional morphology that helps in load distribution.
This heterogeneous growth pattern can also potentially be explained by the meniscal dependence on bony morphology. We have shown that a significant majority of the measured meniscal morphologic features correspond directly to the developing femoral condyle curvature, supporting our other initial hypothesis. Our finding is similar to that of Clark and Ogden, 6 who established a very steady and consistent relationship between the developing meniscal surface area and the corresponding tibial plateaus. The relationship observed between meniscal morphology and the corresponding bony anatomy, most notably the femoral condyle curvature radius in our study, potentially indicates a close developmental dependency between these two anatomic features. It is possible that the meniscus develops to accommodate changes in the tibiofemoral contact areas as the femur and tibia develop, as suggested by Clark and Ogden. 6 This dependence on bony morphology is an important finding that paves the way for further research into the connection between potential anatomic mismatch of the tibial plateaus and femoral condyles and the potential subsequent predisposition to developmental anomalies, such as discoid menisci, and/or meniscal injury.
Limitations
There are several limitations to this study to consider. Although we reviewed each case and only selected cases with “normal-looking knees” and no prior history of injury, we cannot exclude the possibility of them having abnormal joint anatomy. Because the patients in this cohort underwent MRI to assess potential injuries, the effects of the potential injury on the surrounding knee are unknown and the meniscus may in fact not be normal. Furthermore, the patients were grouped by their chronological age and not skeletal age. Moreover, we did not control for other factors (i.e., race, ethnicity, and physical activity) that may influence development and anatomy of the menisci. Additionally, the retrospective nature of this study may introduce limitations in using MRI to obtain accurate measurements, with the possibility that all patients may not have optimal MRI orientations to fully capture the meniscal geometry. It should also be noted that different scanning parameters used for the cohort may introduce variability in morphologic measurements. Finally, the cross-sectional nature of this study does not fully portray the longitudinal changes in a patient's anatomic features during growth and development. Future prospective longitudinal studies are necessary to confirm these findings.
Conclusion
We have shown in this study that beyond size growth, fundamental changes also occur in meniscal morphology with aging. The data suggest that the meniscus undergoes a larger growth rate in the axial plane compared with the superior-inferior direction, resulting in smaller mean tip angles and fundamental differences in meniscal geometry between young children and adults. This may suggest a shift in functional morphology to allow for greater load distribution as development occurs. This study also gives further insight into sex-based differences in meniscal growth, with suggestions that there are sex differences in meniscal morphology throughout development and in meniscal size later in development. Further investigations are warranted to discover intrinsic and extrinsic factors that may influence the development of meniscal morphology during growth as well as the influence of each of these morphological features on knee biomechanics, stability, injury risk, and developmental musculoskeletal pathologies.
Footnotes
Acknowledgements
The authors acknowledge the significant contributions of Ms. Gabriela Portilla, Dr. Kirsten Ecklund, and Dr. Martha Murray for assisting with this study.
Final revision submitted August 29, 2023; accepted September 18, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Children's Hospital Orthopaedic Surgery Foundation and Boston Children's Hospital Faculty Council. A.M.K. has received consulting fees from Miach Orthopaedics and maintained a conflict-of-interest management plan that was approved by Boston Children's Hospital and Harvard Medical School during the conduct of the study, with oversight by both conflict-of-interest committees and the institutional review board of Boston Children's Hospital. G.S.P. has received education payments from Kairos Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children's Hospital (reference No. IRB-P00015233).