
Abstract
Background:
Malalignment has been suggested as a predisposing factor for the development of osteochondral lesions of the talus (OLTs).
Purpose:
To evaluate the clinical and radiographic outcomes of realignment surgery in patients with a large cystic OLT of the talar shoulder and concurrent malalignment of the foot and ankle.
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors reviewed consecutive patients with large cystic OLTs (diameter, >10 mm) of the talar shoulder and concurrent malalignment of the foot and ankle who underwent realignment surgery between September 2013 and April 2021. The type of realignment procedure was determined based on patient symptoms and findings on plain radiographs and weightbearing computed tomography. Clinical improvement was assessed using pre- and postoperative Foot Function Index (FFI) scores and the visual analog scale (VAS) for pain. The OLT location was categorized according to Raikin zone, and the OLT area and volume were measured and compared pre- and postoperatively. The comparative analysis was performed using the Wilcoxon signed-rank test.
Results:
In total, 27 ankles in 27 patients (mean age, 34.4 ± 11.9 years) were included in the analysis. There were 25 patients with a medial lesion (zone 4 [n = 19], zone 7 [n = 5], and zone 1 [n = 1]), and 2 patients with a lateral lesion (zone 6). Despite OLT location, patients’ symptoms varied; 15 (55.6%) patients reported both medial- and lateral-sided pain, 10 (37%) reported lateral-sided pain, and 2 (7%) reported medial-sided pain. Supramalleolar osteotomy was performed in 18 patients, while foot and hindfoot correction without supramalleolar osteotomy was performed in 9 patients. Postoperatively, both the median FFI (from 44.4 [interquartile range (IQR), 35.7-52.2] to 9.1 [IQR, 5.2-13.9]) and median VAS pain score (from 6 [IQR, 5-6] to 1 [IQR, 1-2]) improved significantly (P < .0001 for both), and the median lesion size (from 25.8 mm2 [IQR, 19.3-45.2 mm2] to 13.8 mm2 [IQR, 6.8-26.5 mm2]) and median volume (from 2226.8 mm3 [IQR, 1311-3104 mm3] to 1326.5 mm3 [IQR, 714-2100 mm3]) decreased significantly (P < .0001 for both). During the mean follow-up of 4.1 ± 2.1 years, no subsequent surgery for OLT was necessary.
Conclusion:
The results suggest that realignment procedures can improve the symptoms and radiographic profile of OLTs in patients with large cystic OLTs of the talar shoulder and malalignment of the foot and ankle.
Direct surgical treatment for osteochondral lesions of the talus (OLTs) is performed under the assumption that the lesion is the primary cause of the patient’s pain or may contribute to the development of degenerative ankle arthritis. Current surgical approaches for OLT are guided by the size and location of the lesion, 20 with a focus on regenerating or replacing damaged cartilage and subchondral bone to improve the biology of the joint.17,20
However, the origin of pain in patients with OLTs is not yet fully understood, and clinical evaluations of these patients are often complex and ambiguous. 18 The nature and localization of the pain reported by patients do not always correspond with the location of the lesion, and some OLTs are even asymptomatic and resolve spontaneously over time.15,22,25 Furthermore, concomitant procedures such as spur excision or synovectomy are frequently performed during OLT repair, making it challenging to attribute symptomatic improvement solely to the treatment of the OLT.
The treatment of large cystic osteochondral lesions, especially those located in the talar shoulder, poses a significant challenge.2,4,7,8 Mosaicplasty is known to be inadequate because of the lack of buttress, while allograft transplantation has been described as a possible solution.2,7 However, this option is costly, and it carries the potential risk of graft failure. 7 The senior author of this study (W.C.L.) has treated patients with large cystic osteochondral lesions in the talar shoulder whose symptoms were not clearly explained by the presence of osteochondral lesions. For this subset of patients, realignment procedures were performed to provide symptomatic relief instead of the patients undergoing direct treatment for the lesion. Although realignment procedures have been simultaneously performed at the time of cartilage repair surgery in previous studies,5,19,29 there is no evidence pertaining to the isolated effect of realignment in patients with OLTs.
The purpose of this study was to report the minimum 2-year clinical and radiographic outcomes of realignment surgery in patients with a large cystic osteochondral lesion of the talar shoulder with concurrent malalignment of the foot and ankle. We hypothesized that realignment procedures aimed at improving the biomechanical environment of the ankle joint might effectively relieve symptoms in patients with large cystic osteochondral lesions of the talar shoulder and also improve the radiographic appearance of the lesion.
Methods
Study Cohort
After receiving institutional review board approval for the study protocol, we reviewed the records of consecutive patients who had a large cystic osteochondral lesion of the talar shoulder (diameter, >10 mm) and underwent realignment surgery at our institution between September 2013 and April 2021. The diagnosis of OLT was made through imaging, which included weightbearing radiographs, computed tomography (CT) scans, and/or magnetic resonance imaging (MRI). Patients who were >18 years at the time of surgery and had minimum 2-year follow-up data were included in the study. Patients who had (1) definitive joint space narrowing (Kellgren-Lawrence grade 3 or 4) or tibiotalar tilt (talar tilt, >2°) on plain radiographs, which suggests degenerative ankle arthritis; (2) an osteochondral defect without a cystic lesion; or (3) concurrent cartilage repair surgery (eg, microfracture, bone graft, or bone marrow aspirate concentrate) at the time of realignment surgery were excluded from the study. Informed consent for the study was obtained from all patients.
After applying the inclusion and exclusion criteria, there were 27 ankles in 27 patients (18 male, 9 female) in the cohort (Figure 1).

Flowchart depicting the selection of the study patients.
Indications for Realignment Surgery and Surgical Procedures
All surgical procedures were performed by the senior author of this study (W.C.L.). The decision to perform realignment surgery was based on a comprehensive assessment of reported pain and symptoms as well as a physical examination and a radiographic evaluation of malalignment that included weightbearing CT scans. All study patients exhibited discernible malalignment on radiographic evaluation or were evaluated with an osteochondral lesion that was not considered the primary cause of their symptoms. As such, the senior author determined that an isolated replacement procedure for the osteochondral lesion would not effectively resolve patient symptoms, such as extra-articular pain at the sinus tarsi or pain on the opposite side relative to the location of the osteochondral lesion. Nevertheless, as the majority of patients sought surgical treatment specifically for the osteochondral lesion, a shared decision-making process was initiated with each patient. The benefits and risks of the planned realignment procedure, as well as allograft transplantation for the osteochondral lesion, which was described as a possible option for the talar shoulder lesion, were explained. Each patient was informed that secondary surgery specific to the cystic lesion may be necessary if the cyst increases after realignment surgery, and all patients agreed with the plan.
The goal of realignment surgery in this study was to realign the ankle and hindfoot to the tibial axis in order to alleviate pain. The lower limb mechanical axis was also referenced from whole lower limb alignment views to determine the type of osteotomy needed. When there was medial-sided pain and tibial plafond varus, a medial opening-wedge supramalleolar osteotomy (SMO) was performed to correct the tibial plafond varus and translate the ankle laterally. In cases of sinus tarsi pain and hindfoot valgus, 5 mL of lidocaine was administered into the sinus tarsi to assess the changes in pain level in the outpatient clinic. If pain relief was achieved, a medial displacement calcaneal osteotomy (MDCO) was performed to decompress the sinus tarsi. For patients with diffuse medial- and lateral-sided pain and associated malalignment, combined proximal (SMO) and distal (MDCO) realignment surgery was performed.
Other concurrent procedures were added during realignment surgery to achieve a plantigrade foot and stability of the ankle joint, including gastrocnemius recession (n = 7), osteotomy of the first metatarsal (n = 2), medial column stabilization using flexor hallucis longus tendon transfer (n = 2), 10 and the Broström procedure (n = 1). Arthroscopic debridement of anteromedial spurs, loose bodies, or inflamed synovium was performed when needed (n = 15); however, procedures for cartilage regeneration were not performed.
Study Groups
To assess pre- to postoperative changes in alignment, patients were categorized into 2 groups based on the main type of realignment surgery they underwent. The majority of patients who underwent SMO (17/18) received medial opening-wedge (valgus-angulating) SMO, while 1 patient underwent a dome osteotomy to varus angulate and laterally translate the ankle for a lateral-sided osteochondral lesion. 9 Because of the confounding effect of varus angulation of the tibial plafond, this patient was not included in the categorization. Ultimately, patients who underwent medial opening-wedge SMO with or without hindfoot correction were allocated to the supramalleolar realignment group (SRG; n = 17 ankles), while patients who underwent calcaneal osteotomies and/or flatfoot reconstruction were allocated to the hindfoot realignment group (HRG; n = 9 ankles).
Outcomes Evaluated
Radiographic Parameters
The radiographic parameters analyzed preoperatively and postoperatively included the medial distal tibial angle (MDTA) and talar center migration (TCM) from weightbearing ankle anteroposterior radiographs,3,13,30 as well as the hindfoot moment arm (HMA) from hindfoot alignment views. 23 For TCM and HMA, a positive value indicates that the talus is in a medial position and the inferior-most point of the calcaneus is in a lateral location relative to the tibia axis, respectively.
Assessment of OLT Size and Location
The size of the osteochondral lesion of the talar shoulder was measured using CT images, taken from 2 ankles using conventional CT and 25 using weightbearing CT scans. Both the volume of the OLT and the area of the cystic lesion were measured. For determining the OLT volume, the height, width, and length of the lesion in the coronal, sagittal, and axial CT images were measured, as previously reported by Fletcher et al. 7 For the area of the cystic lesion, the coronal, sagittal, and axial CT images displaying the largest lesion in each plane were automatically analyzed using ImageJ graphic-analytic software (US National Institutes of Health) (Figure 2). The area was then calculated by summing the areas in all 3 plane images and dividing by 3. In cases where an osteochondral lesion coexisted with a cystic lesion, the areas of both lesions were obtained and expressed as the area of the cystic lesion, as the cystic lesion often coalesced with the osteochondral lesion. The location of the lesion was described using the 9-zone anatomic grid scheme developed by Raikin et al. 21

The method used to determine the area of the cystic lesion from computed tomography (CT) images. (A) To ensure accuracy, the distance within each CT image was first calibrated using the ImageJ program. (B) Next, the thresholding method was applied to the CT images to segment the cystic area in black and the background in white, resulting in multiple regions of interest (ROIs) of cystic lesions (labeled a through g). (C and D) Finally, the area of each ROI of the cystic lesion was automatically calculated using the program, and this calculation was performed in images that showed the largest lesion in the coronal, sagittal, and axial plane images.
Clinical Assessment
Patient-reported outcomes were determined using the Foot Function Index (FFI) and the visual analog scale (VAS) for pain. The FFI has been previously validated in scientific publications related to foot and ankle surgeries. 27 All patients completed the FFI and VAS pain scores preoperatively and at a minimum of 2 years postoperatively. History of ankle trauma and previous surgery before realignment surgery, as well as any instances of reoperation or revision after surgery, were recorded during the retrospective chart review.
Statistical Analysis
Descriptive statistics are displayed as means ± standard deviations or medians and interquartile ranges (IQRs) for continuous variables and as frequencies (percentages) for categorical variables. The normality in the radiographic measurements was assessed with a Shapiro-Wilk test. The comparison of pre- and postoperative radiographic measurements and clinical outcomes was performed using the Wilcoxon signed-rank test. Statistical significance was determined as a P value of <.05. All statistical analyses were performed in Prism 8 for Mac (GraphPad Software).
Results
A total of 27 ankles in 27 patients were included in this analysis. The mean age of the included patients was 34.4 ± 11.9 years, and the mean body mass index was 25.1 ± 3.4 kg/m2. The mean follow-up period of the cohort was 4.1 ± 2.1 years. Of the 27 patients, 14 (51.9%) reported a history of ankle sprain. The mean duration between their sprain and realignment surgery was 3.3 ± 3.5 years. Prior surgeries had been performed in 7 (25.9%) patients, with 2 having undergone osteochondral autologous transplantation (OAT), 2 having the Broström procedure, 2 having microfracture with the Broström procedure, and 1 having microfracture. The mean time between these index surgeries and the realignment surgery was 4.1 ± 4.6 years.
Regarding the location of pain, 15 (55.6%) patients reported both medial- and lateral-sided pain, 10 (37%) reported lateral-sided pain, and 2 (7%) reported medial-sided pain. The location of the osteochondral lesions showed a different pattern from the reported symptoms, with 25 lesions located medially (Raikin zone 4 [n = 19], zone 7 [n = 5], and zone 1 [n = 1]) and 2 lesions located laterally (Raikin zone 6).
In the SRG group, the median MDTA increased significantly, from 87° (IQR, 85° to 88°) preoperatively to 91.5° (IQR, 90.8° to 94.3°) postoperatively (P < .0001) (Table 1). The preoperative TCM was 1.5 mm (IQR, 0.3 to 2.8 mm), and this changed to −2.5 mm (IQR, –4 to −1.3 mm) postoperatively (P < .0001), indicating lateral translation of the talus relative to the tibial axis. The HMA was not significantly different before and after surgery (P = .4346). In the HRG group, significant changes were seen in the HMA, which was 12 mm (IQR, 0.5 to 13 mm) preoperatively and 0 mm (IQR, –2.8 to 3.5 mm) postoperatively (P < .0078).
Comparison of Radiographic Parameters and OLT Size Before and After Realignment Surgery a
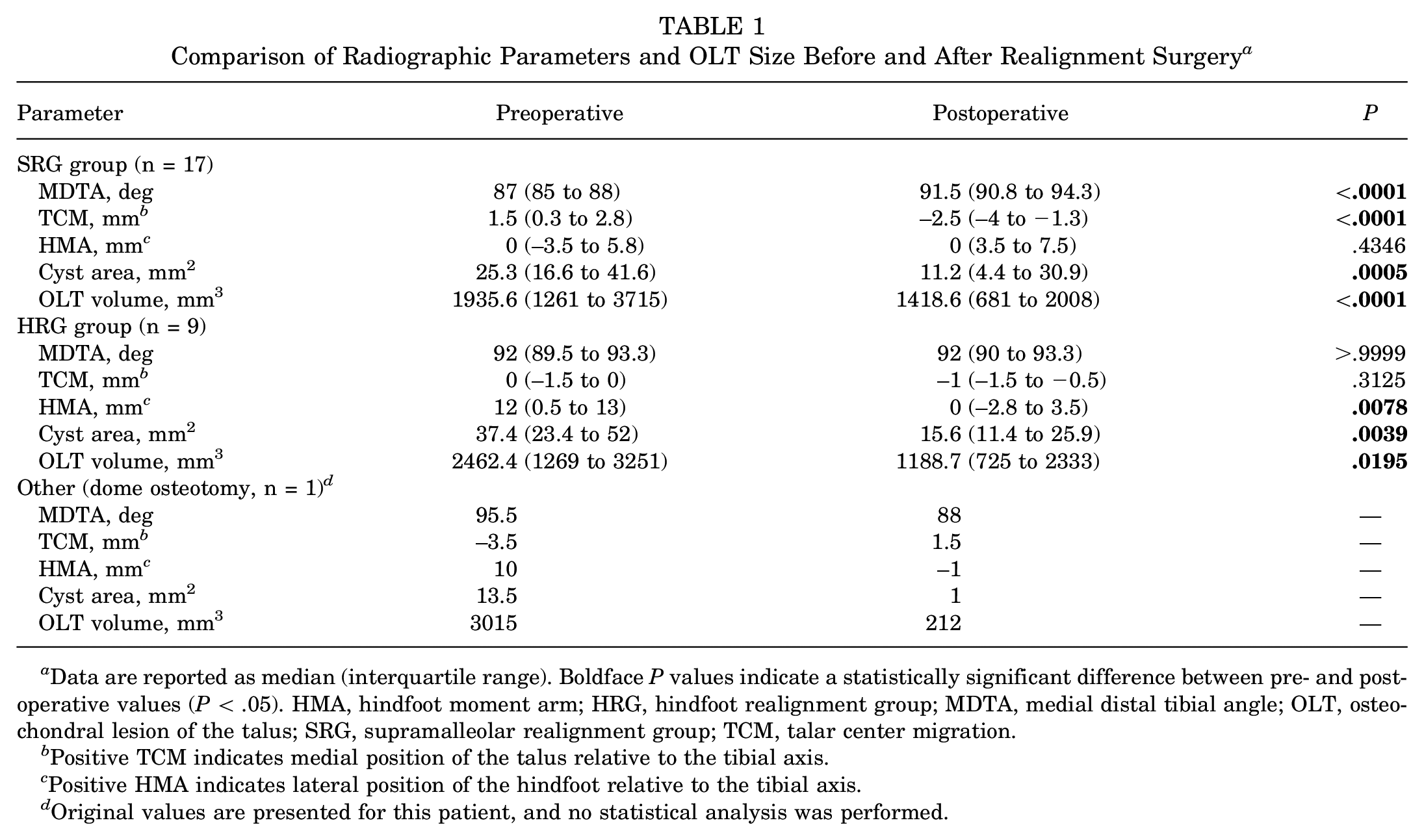
Data are reported as median (interquartile range). Boldface P values indicate a statistically significant difference between pre- and postoperative values (P < .05). HMA, hindfoot moment arm; HRG, hindfoot realignment group; MDTA, medial distal tibial angle; OLT, osteochondral lesion of the talus; SRG, supramalleolar realignment group; TCM, talar center migration.
Positive TCM indicates medial position of the talus relative to the tibial axis.
Positive HMA indicates lateral position of the hindfoot relative to the tibial axis.
Original values are presented for this patient, and no statistical analysis was performed.
There was significant improvement in the radiographic appearance of the osteochondral lesion in all patients (Figures 3 and 4). The median area of the cystic lesion was 25.8 mm2 (IQR, 19.3-45.2 mm2) preoperatively and 13.8 mm2 (IQR, 6.8-26.5 mm2) postoperatively (P < .0001). The median volume of the lesion for all patients was 2226.8 mm3 (IQR, 1311-3104 mm3) preoperatively and 1326.5 mm3 (IQR, 714-2100 mm3) postoperatively (P < .0001).
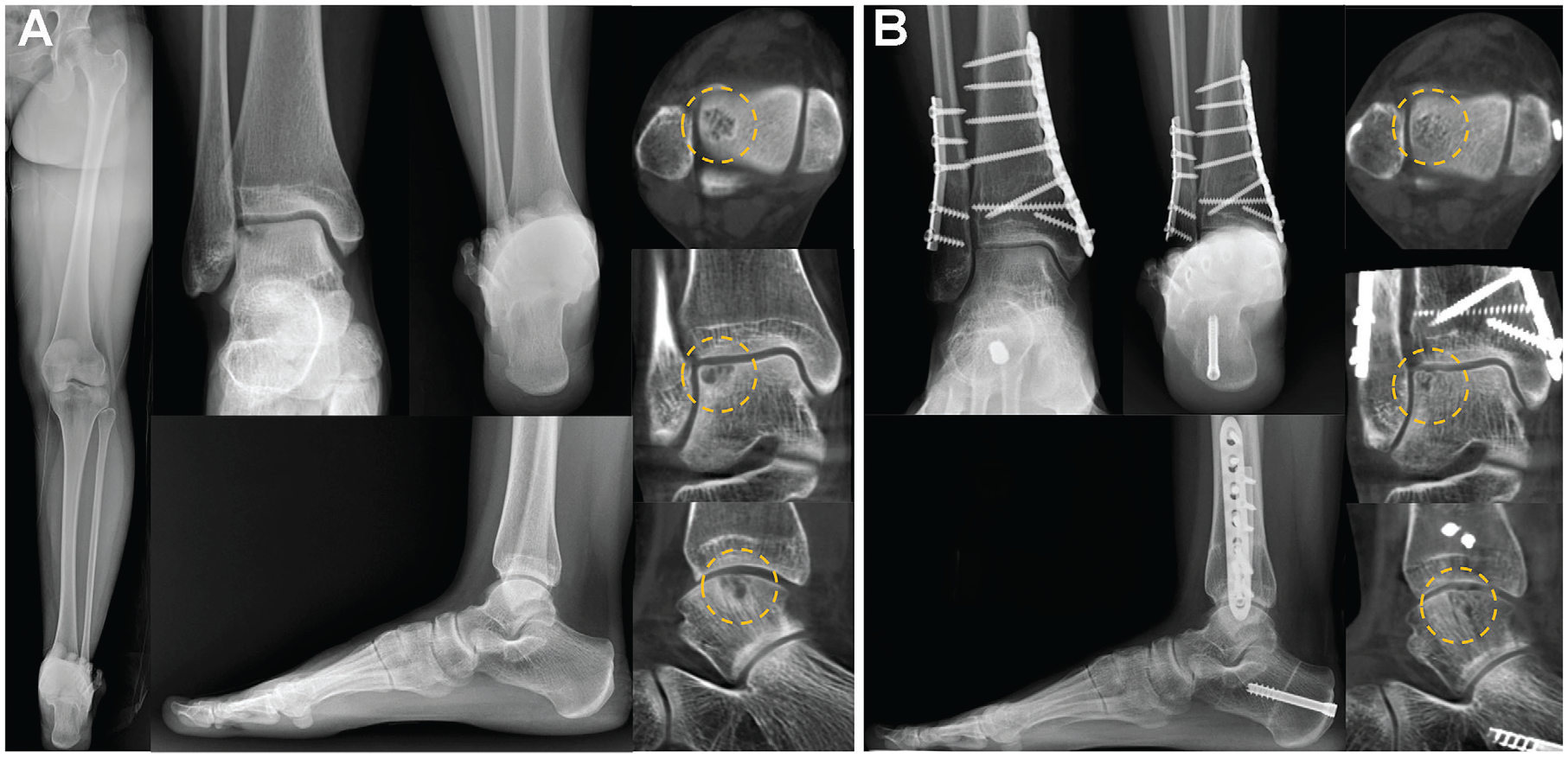
(A) Preoperative and (B) 2-year postoperative images obtained in a 31-year-old female patient who had a cystic osteochondral lesion at the lateral talar shoulder and varus deformity of the lower limb and distal tibia. A supramalleolar osteotomy and medial displacement calcaneal osteotomy were performed. Weightbearing computed tomography images show a decreased size of the lesion as well as spontaneous filling of the cystic lesion (dashed yellow circles).

(A) Preoperative and (B) 3-year postoperative images obtained in a 36-year-old male patient who had a cystic osteochondral lesion at the medial talar shoulder and varus deformity of the lower limb and distal tibia. A medial opening-wedge supramalleolar osteotomy was performed. Weightbearing computed tomography images show a decreased size of the lesion as well as spontaneous filling of the cystic lesion (dashed yellow circles).
Clinical scores improved significantly after surgery in all patients, with the median VAS improving from 6 (IQR, 5-6) to 1 (IQR, 1-2) and the median FFI improving from 44.4 (IQR, 35.7-52.2) to 9.1 (IQR, 5.2-13.9) (P < .0001 for both). Seventeen (63%) patients had hardware removal, but none of the patients underwent secondary surgery for the osteochondral lesion.
Discussion
Our findings demonstrated that realignment procedures, aimed at enhancing the biomechanical environment within the ankle joint, led to a significant improvement in VAS pain and FFI scores from pre- to postoperatively (P < .0001 for both). Additionally, we observed an improved radiographic profile of OLTs postoperatively, with a spontaneous decrease in median lesion area (from 25.8 to 13.8 mm2; P < .0001) and volume (from 2226.8 to 1326.5 mm3; P < .0001). None of the patients required a secondary procedure to address the OLTs during the mean 4.1-year follow-up period.
Although a direct causal relationship has not been established, existing literature suggests a plausible association between malalignment and the development of OLTs.6,16 Eccentric loading within the ankle joint can result in degenerative changes in the cartilage, and subsequent injury to the subchondral bone plate may allow joint fluid to infiltrate, creating a conducive environment for the development of a cystic lesion. 28 Our study results provide evidence of this possible association through radiographic improvement of the lesion after realignment procedures. While the exact mechanism of this radiographic improvement is not fully understood, it may be related to the decreased local pressure resulting from the redistribution of load within the ankle joint after realignment surgery. Additionally, the decreased size of the cystic lesion might have contributed to symptomatic relief, possibly from decreased stimulation of the nerve endings at the subchondral bone plate. 28
The use of realignment procedures in patients with OLTs is not a novel concept and has been previously documented in the literature. Li et al 19 reported successful outcomes in 11 cases in which biplanar SMO was performed concurrently with OATs for patients with a large OLT and varus distal tibial deformity. Similarly, Wiewiorski et al 29 described a case in which SMO with flatfoot reconstruction was performed in a patient for whom OAT failed and who had concurrent valgus distal tibial plafond and flatfoot deformity. Although these studies suggest the potential benefits of realignment surgery in patients with OLTs, the isolated effect of realignment surgery on the healing of osteochondral lesions has not been fully elucidated. However, a 2023 study by Kim et al 11 has provided new insight into this topic. These authors described 8 patients who had failed OATs and developed cystic lesions around the plug. Notably, those patients had malalignment at the distal tibia or hindfoot. Despite no direct treatment to the osteochondral lesion itself, the patients experienced both clinical and radiographic improvement of the osteochondral lesion, 11 which is consistent with the findings of the current study.
While the altered load distribution pattern within the tibiotalar joint resulting from varus or valgus distal tibial alignment has been well documented,16,24 we used the mediolateral position of the talus relative to the tibial axis (assessed with TCM) as an important additional parameter to determine the need for realignment procedures. 13 Medial talar translation may be associated with internal rotation of the talus in the axial plane,12,14,26 which we believe increases medial tibiotalar joint pressure and causes extra-articular symptoms such as sinus tarsi pain from talocalcaneal subluxation. 12 Therefore, even if the MDTA was within the normal range, if the talus was medially located relative to the tibial axis, SMO was performed to translate the talus slightly lateral to the tibial axis to decrease the medially directed shearing force within the joint.
Surgical treatment of a large cystic osteochondral lesion of the talar shoulder presents a significant challenge. Traditional treatments for a large OLT, such as OAT, may be ineffective for the shoulder lesion because of the lack of buttress and consequent difficulties in graft integration. As a potential alternative, fresh allograft transplantation has been used to replace the involved lesion.1,2,7 However, accessibility to size-matched fresh donors is not readily available for all orthopaedic centers. Additionally, allograft transplantation carries inherent risks of disease transmission 7 and potential nonunion or graft failure.
The results of the current study provide a possible option for patients with a large cystic osteochondral lesion of the talar shoulder, particularly if an isolated direct surgical treatment targeting the osteochondral lesion does not seem to improve patients’ symptoms in preoperative evaluation. In our study, the decision to pursue realignment procedures was based on the symptoms reported by the patients, in addition to radiographic assessment of malalignment. Despite the presence of a large cystic lesion on the talus, many patients included in this series had discrepancies in the location of their pain and the lesion. Furthermore, extra-articular pain at the sinus tarsi was the most common symptom, leading us to believe that altered kinematics resulting from malalignment may have been the primary source of the patients’ symptoms. Additionally, patients with medial lesions demonstrated slight medial gutter narrowing on the weightbearing CT, suggesting that correcting the biomechanical environment could benefit patients more than focusing solely on the cartilage lesion. This observation from the weightbearing CT is critical, as evaluation of OLT has largely relied on plain ankle radiographs up to now. As our study indicates, even patients without discernable joint space narrowing on plain radiographs may exhibit joint narrowing on weightbearing CT. Therefore, analyzing ankles with large osteochondral lesions of the talar shoulder could lead to a new understanding of OLTs and their treatment.
While realignment procedures resulted in a significant reduction in cyst volume and improvement in OLT profiles, the study does not conclusively indicate that these procedures replace the need for concurrent cartilage procedures. When OLTs are a significant source of pain, concurrent cartilage procedures may provide benefits to patients. 6 However, such procedures require an additional intra-articular osteotomy, which can have inherent complications and compromise blood supply to the talus. Hence, given the potential risk associated with concurrent cartilage procedures during realignment surgery, patients must be fully informed of the potential morbidity before making decisions regarding the feasibility of these interventions.
Limitations
This study has several limitations that must be acknowledged. First, the small number of cases and the lack of long-term follow-up make it challenging to draw definitive conclusions regarding the efficacy of realignment surgery for treating large osteochondral lesions of the talar shoulder. To obtain more robust results, future studies should adopt a prospective design with a sufficient sample size, considering comparative analyses with other treatment methods for similar lesions. Second, the retrospective nature of the study and the absence of a preoperatively well-established operative algorithm for realignment surgery may have introduced bias into the method of realignment. While the general principle of realignment involved translating the talus and the heel closer to the tibial axis, the specific method of realignment varied among patients. Additionally, the inclusion of patients who had previously undergone failed surgery and the heterogeneity of lesion locations are further limitations that could impact the study’s outcomes. Third, the method used to measure the size of osteochondral lesions was limited by the difficulty in accurately measuring the exact size of the lesion in 3 dimensions. In this study, the cystic area of the osteochondral lesions was assessed separately from the overall size of the lesion, considering that cystic osteochondral lesions often have a worse prognosis than noncystic ones. However, the variable shape and location of the cystic lesion may have introduced some margin of error in the measurement. Lastly, arthroscopic findings were not available, and MRI scans would have provided more detailed information about the condition of the ankle joint.
Conclusion
The findings of this study indicate promising short-term effects of realignment surgery for the clinical improvement and radiographic spontaneous healing of large cystic osteochondral lesions of the talar shoulder with concurrent malalignment. However, a longer-term observation of this cohort is necessary to determine whether the improved biomechanical environment of the ankle joint will further enhance the radiographic profile or if additional procedures will be necessary to manage the lesion.
Footnotes
Final revision submitted August 8, 2023; accepted September 7, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from a public institutional review board designated by the Ministry of Health and Welfare (reference No. P01-201911-21-001).