
Abstract
Background:
Some patients with lateral ankle sprain (LAS) will experience chronic lateral ankle instability (CLAI). However, not all of those with residual increased lateral ankle laxity (ILAL) become symptomatic. There is a lack of evidence regarding the prevalence of undiagnosed ILAL in the general population.
Purpose:
To evaluate the prevalence of undiagnosed ILAL with the use of stress ultrasonography (US) and to investigate the percentage of ankle sprain copers (ASCs) with ILAL.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The anterior talofibular ligament (ATFL) lengths in college students without diagnosis of CLAI were measured consecutively in stress and nonstress positions. The ATFL ratio was calculated as an indicator of lateral ankle laxity according to a previously reported method. The manual anterior drawer test was also performed. The Cumberland Ankle Instability Tool (CAIT) and Ankle Instability Instrument (AII) were used to assess subjective impairments related to CLAI. The correlation between the ATFL ratio and CAIT score was evaluated.
Results:
A total of 207 ankles from 106 participants (mean age, 23.9 ± 2.2 years; male/female, 64/42) were included. Overall, 38 participants (35.8%; 50 ankles [24.2%]) were classified as having undiagnosed ILAL. Of the ankles with no history of LAS, 8% showed ILAL. Overall, 53 participants (50%) had a history of LAS and were all classified as ASCs. Of the 82 ankles from these ASCs, 40 (48.8%) were regarded as having undiagnosed ILAL. There was no correlation between the ATFL ratio and CAIT scores (r = -0.09, P = .414).
Conclusion:
The prevalence of undiagnosed ILAL by stress US screening was approximately one-third in young adults. In this study, 48.8% of the ankles from ASCs showed ILAL.
Keywords
Lateral ankle sprain (LAS) is a common musculoskeletal injury in nonathletic persons as well as in athletes.17,41 LAS needs to be managed in the early stage because it is often associated with several pathologies and high socioeconomic cost.17,27 Some patients who incur a primary LAS will experience chronic lateral ankle instability (CLAI) if left untreated or treated inappropriately.19,38 It has been reported that >50% of athletes with LAS do not report to a medical facility.25,29,39 In addition, evidence-based treatment may not be offered for patients with LAS even when they visit an orthopaedic hospital.38,47 Therefore, patient education and improvement of their understanding of the clinical significance of LAS and CLAI, as well as advancement in the diagnosis and treatment of LAS or CLAI by clinicians, are still needed.
As people with a history of LAS may not completely recover after their injury, it is estimated that there is a percentage of patients with LAS who have not been diagnosed with CLAI or who have residual increased lateral ankle laxity (ILAL). Historically, asymptomatic patients with a history of LAS have been classified as ankle sprain copers (ASCs).6,14,24,43 In general, ASCs rarely visit a medical facility, as these asymptomatic patients frequently do not notice the presence of ILAL. However, CLAI has been shown to be a cause of secondary ankle osteoarthritis.1,23,37 Thus, ASCs with ILAL may have an increased risk of developing ankle osteoarthritis compared with those without ILAL.
No previous studies can answer the following question: what is the future of ankles with undiagnosed ILAL when left untreated? In addition, as far as we know, no studies have investigated the extent to which ASCs have ILAL. Therefore, as a first step, it is worth investigating the percentage of ASCs who have undiagnosed ILAL. Stress ultrasonography (US) is a noninvasive modality and has been shown to be effective and reliable for evaluating LAS or CLAI.5,32,44,45,46 Therefore, stress US may be an effective tool for screening ILAL in the general population.
The primary purpose of this study was to evaluate the prevalence of undiagnosed ILAL in the general population with the use of stress US. The secondary purpose was to investigate the percentage of ASCs who have residual ILAL.
Methods
The protocol for this cross-sectional study was approved by an institutional review board. Medical college students were consecutively contacted and recruited at a single institute between April 1, 2021, and March 31, 2023. All participants provided their written informed consent before participating in this study. The study inclusion criteria were men and women ≥20 years old who had not been diagnosed with CLAI. We defined CLAI as ≥1 episode of LAS and ≥2 episodes of giving-way sensation of the ankle in the past 6 months. 20 In addition, participants who answered “yes” to ≥5 questions on the Ankle Instability Instrument (AII) and scored ≤24 on the Cumberland Ankle Instability Tool (CAIT) were considered to have CLAI.16,20,22,24 The AII and CAIT have been used widely in studies regarding CLAI, and their validity and reliability have been shown.16,22 The definition of LAS was applied based on the statement by the International Ankle Consortium as an acute traumatic injury to the ankle lateral ligament due to excessive inversion of the rear foot or a combined plantarflexion and adduction of the foot that results in at least 1 interrupted day of physical activity. 20 The study exclusion criteria were as follows: LAS within 12 months of the study, a history of surgery of the foot or ankle, presence of foot or ankle pain at the time of recruitment, inflammatory arthritis, and Ehlers-Danlos or Marfan syndrome.
Data Collection
Data regarding the age, sex, height, weight, body mass index (BMI), foot size, dominant ankle, and Tegner activity scale were obtained. 4 The dominant ankle was defined as the laterality used when kicking a ball. 31 Generalized joint laxity was assessed by the Beighton score. 2 In addition, participants completed a questionnaire regarding LAS. The questions included occurrences of LAS (0, 1, and ≥2 times), age at primary LAS (<10, 10-14, 15-19, and ≥20 years), whether they had visited a hospital at the time of primary LAS, and presence of giving-way sensation of the ankle within 6 months. Finally, the participants completed the CAIT and AII to evaluate self-reported impairments relating to CLAI. 20
Manual Anterior Drawer Test
The manual anterior drawer test (ADT) was performed by a senior orthopaedic surgeon (Y.M.) before the US examination. Manual ADT of the ankle was conducted with the participant in the supine position. The knee joint was flexed, and the ankle joint was sustained in 10° to 15° of plantarflexion. The participant was instructed to relax before the performance of ADT. While grasping the heel of the examined ankle with 1 hand and stabilizing the distal tibia with the other hand, the examiner drew the ankle anteriorly until no further movement was possible. The results were classified into 3 grades: 1, stable joint; 2, partially unstable; or 3, completely unstable. 8
Stress US Evaluation of the ATFL
The US evaluation of the ATFL was performed in the nonstress position (resting position) and the stress position (manual maximal internal rotation), as reported by Yokoe et al.44,45,46 All evaluations were performed by a certified orthopaedic surgeon (T.Y.) who was blinded to patient information.
US images were obtained with an Aloka Arietta 850 US apparatus (Hitachi) using a linear probe (L64 probe; 18-5 MHz). The spatial resolution of the US apparatus was as follows: axial resolution, ≤0.8 mm; and lateral resolution, ≤3.0 mm. The stress US procedure was reported previously.44,45,46 The accuracy and reproducibility of the stress US technique have been reported previously (intraclass correlation coefficients for the nonstress ATFL length, stress ATFL length, and ATFL ratio were 0.991, 0.993 and 0.987, respectively). 46 The US images were taken in 2 positions: resting (nonstress ATFL) and at manual maximal internal rotation (stress ATFL).
The nonstress ATFL images were taken first. The participant was in a sitting position with 1 leg hanging from the edge of the examination table (resting position). The transducer was placed over the ATFL and was parallel to the sole of the foot. The participant was then instructed to relax the ankle muscles with the ankle joint at 10° to 20° of plantarflexion. The ATFL length was measured as the linear distance from the origin to the insertion of the ATFL using digital calipers included with the US apparatus. The origin and insertion points of the ATFL were identified as bony landmarks to ensure standardization of the ATFL in a manner reported previously. 3 Thereafter, a stress ATFL image was obtained. The participant was first instructed to sit in the aforementioned resting position (in plantarflexion), and the examiner applied maximal internal rotation manually with varus talar tilt to the ankle by grasping the heel of the participant. The internal rotation with varus talar tilt in plantarflexion is useful for evaluating lateral ankle laxity.18,21
The ATFL length was measured as the linear distance from the origin to the insertion of the ATFL, in the same manner as for the nonstress ATFL images. The anterolateral aspect of the lateral malleolus was identified as the ATFL origin, and the peak of the talus was used as the insertion point. The peak of the talus also represents the anterior aspect of the lateral talar articular cartilage and the lateral neck of the talus. These bony landmarks can be identified as hyperechogenic points and were confirmed to ensure that the talar insertion was consistently selected at a reference point across images. 12 On both the nonstress and stress US images, the ATFL length was measured 3 times, and the mean of the 3 measurements was used to calculate the ATFL ratio (defined as length of stress ATFL/length of nonstress ATFL). The presence or absence of the avulsion fragment of the lateral malleolus was also evaluated.
Definitions of ASC and ILAL
Participants were classified as ASCs when they reported a history of at least 1 LAS with no subsequent sensations of giving way, answered “yes” to ≤4 questions on the AII, and scored >24 on the CAIT.24,43 According to studies by Yokoe et al,44,45 the normative values of the ATFL ratio in young men and women are 1.07 ± 0.04 and 1.09 ± 0.04, respectively.
In the present study, ILAL was defined as an ATFL ratio >1.15 for men and >1.17 for women, as these reference standards were twice the magnitude of each standard deviation. According to this definition, we categorized the study participants as “ILAL” or “no ILAL.”
Statistical Analysis
Data analyses were performed using the SAS software program (JMP Pro, Version 15.2.0; SAS Institute). The threshold of significance was set at P < .05. The data were reported as mean values with 95% confidence intervals. The Shapiro-Wilk method was used to test whether the data were distributed normally. The Student t test or Mann-Whitney U test was used to compare continuous data, and the chi-square test was used for categorical variables.
We compared the ILAL and no-ILAL groups with regard to overall characteristics, primary LAS occurrence, outcome scores, and examination findings. A similar subgroup analysis was also conducted on participants classified as ASCs with and without ILAL. In addition, the correlation between the CAIT score and the ATFL ratio was evaluated in ASCs using the Spearman rank correlation coefficient. The strength of the correlation of the rank coefficients was defined as follows: strong, 0.70 to 1.0; moderate, 0.40 to 0.69; and weak, 0.20 to 0.39. 26 No a priori power analysis was performed, as there were no data available to perform such analysis.
Results
Prevalence of Undiagnosed ILAL
Of the 212 ankles from 106 participants that were contacted in the study period, a total of 207 ankles from 106 participants were included, as shown in Figure 1. Overall, 24.2% (50/207) of the ankles (35.8% [38/106] of the participants) were classified as having undiagnosed ILAL. Ipsilateral ILAL was seen in 26 participants, and bilateral ILAL was seen in 12 participants.

Flowchart showing patient enrollment. CLAI, chronic lateral ankle instability; ILAL, increased lateral ankle laxity; LAS, lateral ankle sprain.
The participant characteristics according to study group are shown in Table 1. There were no significant differences other than weight (P = .007) and BMI (P = .002) between the groups. The data concerning primary LAS and giving-way episodes according to number of ankles are shown in Table 2. Previous occurrence of LAS was significantly greater in the ankles with ILAL (P < .0001). Of ankles without a history of LAS, 8% (10/125) showed ILAL. Table 3 summarizes the outcome scores, ADT, and stress US evaluations of the 2 groups. Significant group differences were detected across all variables (P < .0001 for all) except for nonstress ATFL length.
Characteristics of Study Participants With and Without ILAL (N = 106) a

Data are reported as mean ± SD (range) or No. of participants (%) unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ILAL, increased lateral ankle laxity.
Primary LAS and Giving Way of the Ankle (N = 207 Ankles) a
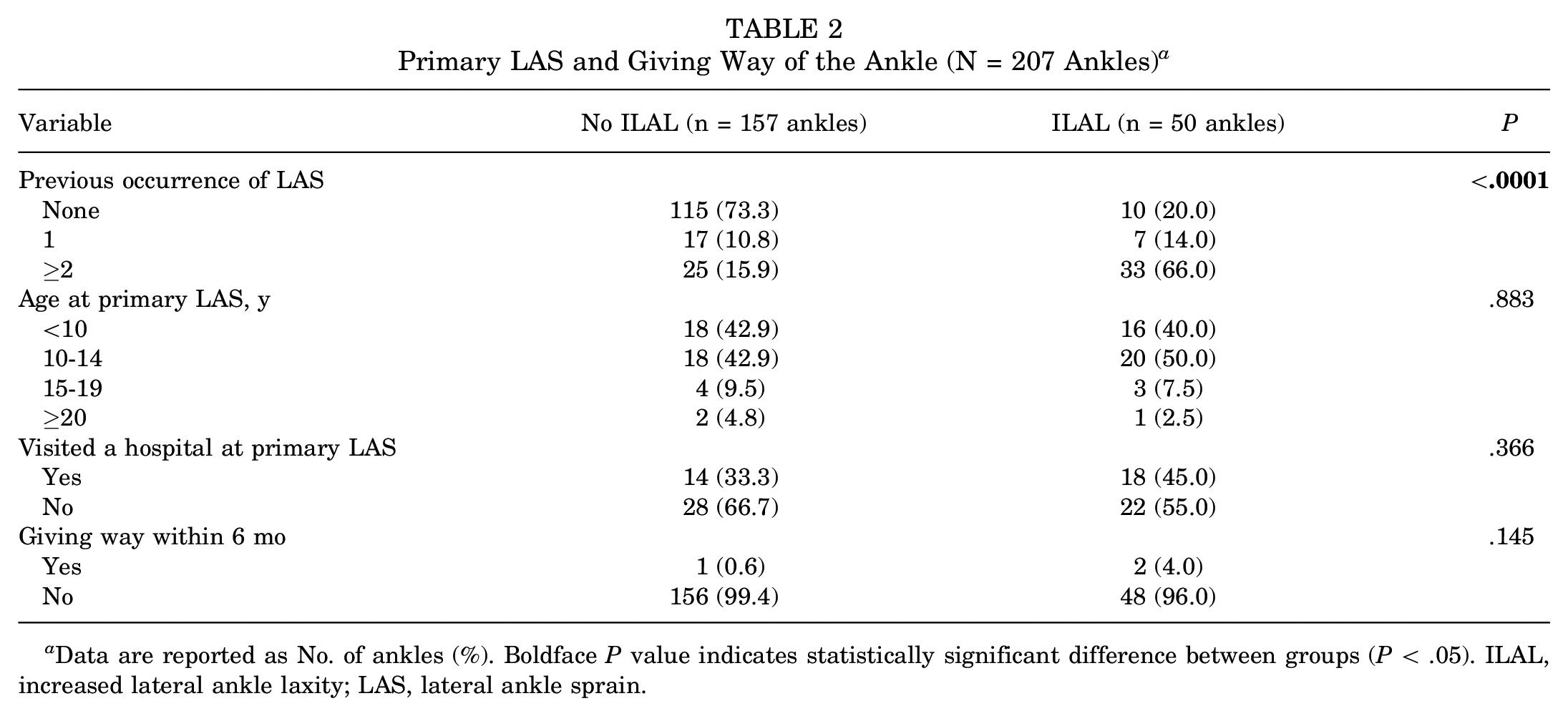
Data are reported as No. of ankles (%). Boldface P value indicates statistically significant difference between groups (P < .05). ILAL, increased lateral ankle laxity; LAS, lateral ankle sprain.
Outcome Scores, ADT, and Ultrasound Findings (N = 207 Ankles) a
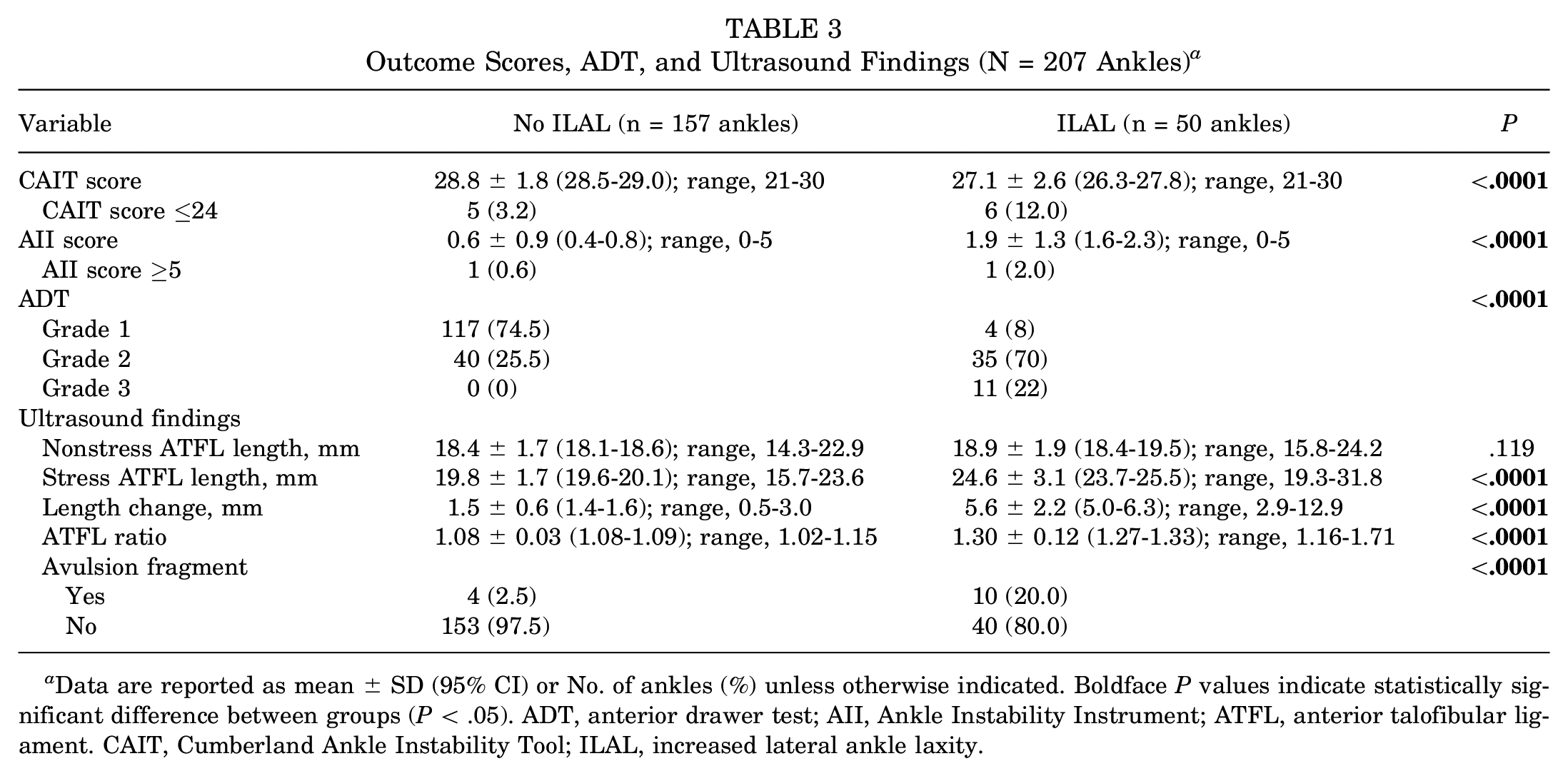
Data are reported as mean ± SD (95% CI) or No. of ankles (%) unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ADT, anterior drawer test; AII, Ankle Instability Instrument; ATFL, anterior talofibular ligament. CAIT, Cumberland Ankle Instability Tool; ILAL, increased lateral ankle laxity.
Comparison of ASCs With and Without ILAL
Of the 207 ankles, 82 (39.6%; from 53 participants [50%]) had a history of LAS. All of these participants were classified as ASCs. Of these ankles, 48.8% (40/82) were regarded as having undiagnosed ILAL. The characteristics of ASCs with and without ILAL are shown in Table 4. The results of CAIT, AII, ADT and stress US evaluations for this subgroup are shown in Table 5. No correlation was detected between the CAIT and the ATFL ratio in ASCs (r = -0.09, P = .414) (Figure 2).
Characteristics of ASCs With and Without ILAL (n = 82 Ankles) a

Data are reported as mean ± SD or No. of ankles (%) unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ASC, ankle sprain coper; ILAL, increased lateral ankle laxity; LAS, lateral ankle sprain.
Outcome Scores, ADT, and Ultrasound Findings in ASCs (n = 82 Ankles) a

Data are reported as mean ± SD (95% CI) or No. of ankles (%) unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ADT, anterior drawer test; AII, Ankle Instability Instrument; ATFL, anterior talofibular ligament; CAIT, Cumberland Ankle Instability Tool; ILAL, increased lateral ankle laxity; LAS, lateral ankle sprain.

Correlation of the ATFL ratio and CAIT score in ASCs. ASC, ankle sprain coper; ATFL, anterior talofibular ligament; CAIT, Cumberland Ankle Instability Tool.
Discussion
The most important finding of the present study was that the prevalence of undiagnosed ILAL by screening with stress US was approximately one-third among the young adult participants of this study. In addition, 48.8% of the ankles from ASCs showed ILAL. Of the ankles from participants without a history of LAS, 8% showed ILAL.
About 40% of patients with LAS develop CLAI. 15 According to a recent systematic review, 32% of patients with CLAI have chondral or osteochondral lesions. 42 Gradual cartilage degradation causes progression of the vicious cascade from a focal cartilage lesion toward osteoarthritis. 11 Based on the results of the present study, the incidence of undiagnosed ILAL was 35.8% (38/106). At present, why some people with ILAL are asymptomatic has yet to be clarified. However, anterior talar translation and internal rotation are increased by lateral ligament deficiency, leading to the development of osteochondral lesions. Wang et al 40 found that a longer duration from a LAS was associated with medial-side osteochondral lesions. In addition, several studies have suggested that altered landing knee kinematics influence knee injuries, such as anterior cruciate ligament injury.7,28,34 Given that many athletes have LAS, undiagnosed ILAL may predispose athletes to sports-related knee injuries. No studies have clarified what percentage of asymptomatic patients with ILAL will develop osteochondral lesions, ankle osteoarthritis, and knee or hip injuries. As shown in this study, screening of undiagnosed ILAL in asymptomatic patients with a history of LAS using stress US may be valuable for preventing these pathologies because stress US is noninvasive and effective for evaluating the presence of CLAI.5,32,45 When patients with residual ILAL have impaired neuromuscular function associated with CLAI, interventions to improve proprioception deficits or dynamic balance may be beneficial.7,36 Further studies will be needed to clarify whether stress US identification of undiagnosed ILAL will result in a decreased incidence of osteochondral lesions or secondary ankle osteoarthritis due to lateral ankle ligament deficiency.
Asymptomatic patients with a history of LAS have been classified as ASCs and compared with patients with CLAI and healthy controls in previous studies.6,14,24,43 Doherty et al 14 reported that patients with CLAI showed poorer dynamic balance as evaluated by the Star Excursion Balance Test when compared with ASCs and controls. Some authors have hypothesized that recovery from LAS depends on the sensorimotor control strategies adopted after injury.13,15,30 Croy et al 10 reported that greater length changes of the ATFL on US were detected in both ASCs and patients with CLAI than in controls. The authors of that study also found that there was no significant difference in the length change of the ATFL between ASCs and patients with CLAI, although there was a significant difference in the Foot and Ankle Ability Measure scores.
In the present study, we identified 2 groups of ASCs: those with and without ILAL. Approximately half of the ASCs had ILAL. Previous studies on ASCs considered them as a single group and did not separate them into those with versus without ILAL. Several authors have investigated differences in kinematics of the hip, knee, and ankle joints as well as single-leg landing between ASCs and patients with CLAI, and these results would be affected by the presence of ILAL in ASCs. Therefore, in future studies concerning ASCs, the presence of ILAL needs to be evaluated and considered. In addition, why ASCs with ILAL are asymptomatic remains unclear and needs to be clarified.
In the present study, 8% (10/125) of the ankles with no history of LAS showed ILAL. Of the 10 ankles, 4 were from participants with a higher Beighton score (≥5), suggesting the influence of generalized joint laxity on lateral ankle laxity. 45 However, 6 of the 10 ankles were from participants without generalized joint laxity. In this study, the definition of LAS was based on the statement by the International Ankle Consortium. 20 Therefore, participants who had a history of less severe LAS compared with the definition we used would be considered as having no history of LAS. As often is the case, the information regarding the number of LASs is not always correct due to recall bias. Therefore, there is another possibility that the study participants did not clearly remember early episodes of LAS.
Another interesting finding of the current study was that no significant correlation was found between the ATFL ratio and the CAIT. This was contrary to our hypothesis that participants with greater lateral ankle laxity would have a worse CAIT score. The CAIT and AII have been frequently used to evaluate patient-reported limitations caused by CLAI in previous studies performed by physical therapists or athletic trainers.13-15,24,43 However, these subjective scores have rarely been used in studies conducted by orthopaedic surgeons.9,33,35 There is a lack of studies evaluating the association between the extent of ILAL and the CAIT or AII. At present, there is no established measure for evaluating lateral ankle laxity. 33 Therefore, further studies will be needed to investigate the association between the extent of lateral ankle laxity and patient's subjective functional impairments using modalities other than US. This may help us to understand why some patients with ILAL are asymptomatic.
Limitations
There are several limitations to this study. First, this study evaluated the prevalence of ILAL by collecting stress US data of the ATFL in medical college students. Therefore, the prevalence of undiagnosed ILAL may be higher in those with higher Tegner activity scales or based on the type of sport. Second, this was a preliminary study and the sample size was not large. Third, subtalar instability was not assessed. Fourth, this study did not evaluate the influence of medial-side ankle laxity on lateral ankle laxity. The deltoid ligament complex, especially tibiocalcaneal ligament, may affect the internal rotation of the ankle joint. 48 Fifth, the present study evaluated only Japanese participants; the study results may differ in other racial populations. Despite these limitations, this study was the first to evaluate undiagnosed ILAL in young adult volunteers using stress US evaluation of the ATFL.
Conclusion
The prevalence of undiagnosed ILAL according to a stress US was 35.8% among the young adult participants of this study, and 48.8% of the ankles of ASCs showed ILAL. In addition, of the participants without a history of LAS, 8% of ankles (10/125) showed ILAL. Future studies are needed to evaluate whether or not ASCs with undiagnosed ILAL are associated with an increased risk of ankle osteoarthritis or osteochondral lesions. In addition, the presence of ILAL in ASCs should be confirmed in the studies dealing with ASCs because the presence or absence of ILAL may affect the study results.
Footnotes
Final revision submitted September 2, 2023; accepted September 7, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Miyazaki (ref. No. 0-0987).