
Abstract
Background:
Detailed knowledge of the anatomic course of the common peroneal nerve (CPN) is crucial for the surgical treatment of the posterolateral corner (PLC) of the knee.
Purpose:
To investigate the relationship of the CPN to the PLC of the knee at different flexion angles.
Study Design:
Descriptive laboratory study.
Methods:
Ten healthy volunteers were recruited to undergo magnetic resonance imaging (MRI) of the knee joint at knee flexion angles of 0°, 30°, 60°, 90°, and 120°. MRI scans at 3 levels (joint line, tibial cut, and fibular tip) were evaluated to determine (1) the distance from the CPN to the PLC and (2) the distances between the CPN and the anterior-posterior and medial-lateral tibial axes. A 3-dimensional model of the knee joint created from MRI scans of a single participant was used to simulate the creation of a fibular tunnel for PLC reconstruction and investigate the relationship between the CPN, fibular tunnel, and guide pin.
Results:
The CPN moved posteromedially with increased knee flexion angles. As the flexion angle increased, the distances from the CPN to the anterior-posterior axis and the PLC increased significantly, while the distance to the medial-lateral axis decreased significantly at all 3 measurement levels. The distances between the CPN and anterior-posterior and medial-lateral axes were significantly different among the different knee flexion angles at the different measurement levels. There were no significant differences in the mean distance from the CPN to the posterolateral border of the tibial plateau between 0° and 30° of flexion at the fibular tip level (P = .953). There were statistically significant differences in the distance from the CPN to the PLC of the tibial plateau at the different measurement levels. The 3-dimensional model demonstrated that the position of the CPN relative to the guide pin and the bone tunnel undergoes changes during knee flexion.
Conclusion:
Changes in the knee flexion angle produced corresponding changes in the course of the CPN on the posterolateral aspect of the knee joint. The CPN moved posteromedially with increased knee flexion angles.
Clinical Relevance:
Increasing the knee flexion angle during PLC reconstruction can effectively avoid direct injury of the CPN.
The common peroneal nerve (CPN) is the critical structure passing through the posterolateral corner (PLC) of the knee joint; thus, a precise understanding of its anatomic course and location is essential for posterolateral knee surgery. The CPN is fixed on the neck of the fibula by the fibular tunnel. The tunnel entrance is a musculoaponeurotic arch derived from the soleus and peroneus longus muscles; thus, the CPN is particularly vulnerable to injury in this region.15,24
Studies have shown that most CPN injuries are related to trauma or compression.7,10 However, iatrogenic CPN injuries cannot be ignored, including injuries during PLC reconstruction surgeries, compression, injection injuries, traction, and total knee arthroplasty. According to the literature,4,9,18,26,29 the incidence of CPN injury after total knee arthroplasty ranges from 0.3% to 9.5%. Injury to the CPN will seriously affect the function of the corresponding lower extremity. Given the increasing number of surgeries in the posterolateral aspect of the knee joint, such as meniscal repair and PLC injury reconstruction, as well as the cumulative incidence of total knee arthroplasty, the probability of CPN injury has increased accordingly. 23 Knee surgery that involves the PLC of the knee may put the CPN at high risk of direct injury during the procedure. Such surgeries occur close to the CPN; nonetheless, the position of the CPN during knee flexion is poorly understood.
Magnetic resonance imaging (MRI) can effectively visualize and identify the CPN and its adjacent anatomic structures. Therefore, MRI-based studies have been performed to measure the distance between the CPN and the PLC of the knee.5,8,9,25 Studies have focused on measuring the relationship between CPN location and surrounding tissue structures on knee scans in full extension. However, they have not considered the effect of changes in the knee flexion angle on the anatomic location and course of the CPN at the PLC of the knee joint.
This study aimed to investigate the relationship of the CPN to the PLC of the knee at different flexion angles and levels on knee MRI to provide practical information on avoiding CPN injury. The hypothesis was that the knee flexion angles would affect the anatomic location and course of the CPN at the PLC of the knee joint.
Methods
The study participants were 10 healthy volunteers, 6 men and 4 women, aged 31.5 ± 4.38 years, with a mean height of 166.7 cm (range, 158-174 cm) and a mean weight of 65.8 kg (range, 49-80 kg). The main inclusion criteria were as follows: asymptomatic knee joints, no present or previous history of a knee injury, and no previous knee surgery. The study protocol received institutional review board approval, and informed consent was obtained from the participants.
MRI scans of the right knee joints at different knee flexion angles (0°, 30°, 60°, 90°, 120°) were performed for each participant (Figure 1, A-E), and the scan data were exported in DICOM (Digital Imaging and Communications in Medicine) format. A flexible abdominal coil was used for each scan; the volunteers were placed in a lateral position, as the patients could not sufficiently bend their knees in the coil in other positions. The tested limb was then placed under the untested limb for stability. The scan area ranged from 8 cm above the joint line of the distal femur and 8 cm below the joint line of the proximal tibia. All MRIs were performed on a 3.0-T scanner (GE Discovery MR750) with a 3-dimensional (3D) proton-density sequence. Imaging parameters were as follows: repetition time/echo time, 1200/26.04 ms; slice thickness = 0.6 mm; pixel size, 0.3125 mm; and imaging matrix, 512 × 512.
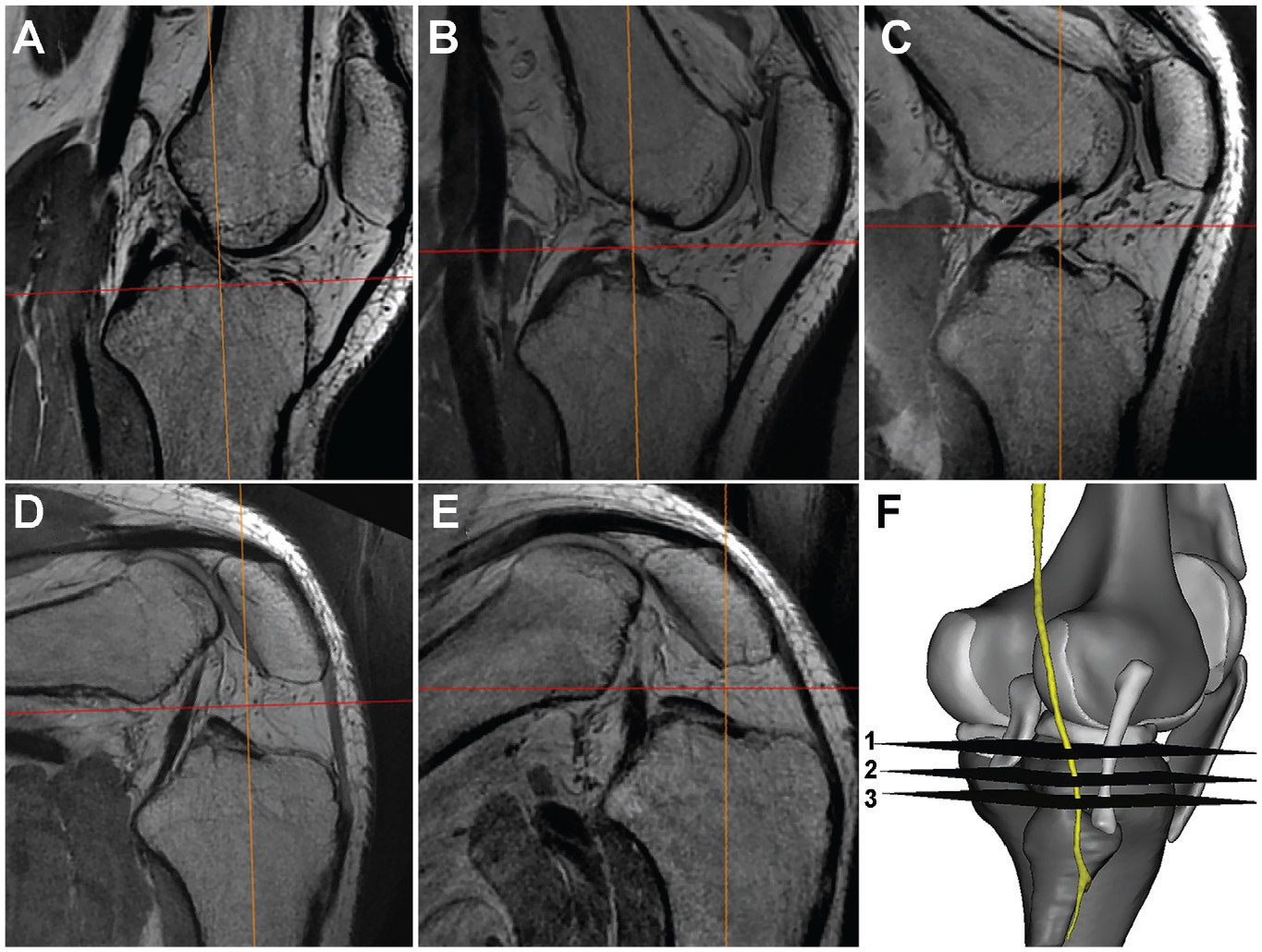
Sagittal MRI of the knee at (a) 0°, (b) 30°, (c) 60°, (d) 90°, and (e) 120° of flexion. (F) Schematic representation of the 3 measurement levels: 1 = joint line level; 2 = tibial cut level; and 3 = tibular tip level. MRI, magnetic resonance imaging.
The scanned data were imported into Mimics software Version 22 (Materialise), allowing them to be visualized in coronal, sagittal, and axial views. The multiplane function of the software was used to adjust the position of the X-, Y-, and Z-axes. Using the method introduced by Akagi et al, 2 we drew the medial border of the patellar ligament insertion and the midpoint of the tibial attachment of the posterior cruciate ligament on the axial view to establish the anterior-posterior (A-P) axis, and the medial-lateral (M-L) axis was established through a vertical line through the midpoint of the A-P axis. The X-Y axis of the software was then adjusted and overlapped with the A-P and M-L tibia axes. On the coronal view, the software's Z-axis was overlaid onto the anatomic axis of the proximal tibia. On sagittal view, the Z-axis was aligned parallel to the posterior cortical bone of the proximal tibia.
MRI Measurements
On axial plane images and using Mimics software, we measured the shortest distance from the CPN to the PLC of the knee at 3 levels—the joint line, tibial cut, and fibular tip (Figure 1F). The tibial cut level was taken 8 mm distal to the chondral surface of the lateral tibial plateau. At the tibial cut and fibular tip level, we took the closest distance between the CPN and the posterolateral border of the tibia. We also measured the shortest distance from the CPN to the A-P and M-L axes of the tibia at the same 3 levels (joint line, tibial cut, and fibular tip). To measure the distances, we drew 2 lines parallel to the A-P and M-L axes intersecting the center of the CPN (Figure 2).

Axial proton density MRI at the tibial bone cut level, demonstrating measurement of the CPN distance to the tibial A-P and M-L axes and the PLC of the knee. A, anterior; A-P, anterior-posterior; CPN, common peroneal nerve; l, lateral; M, medial; M-L, medial-lateral; MRI, magnetic resonance imaging; P, posterior; PLC, posterolateral corner.
Relationship Between the CPN, Fibular Tunnel, and Guide Pin
The knee MRI scans of a single male participant (age, 38 years; weight, 75k g; height, 173 cm) were used to develop 5 different flexion angles of 3D knee models. The 3D models included the CPN, bone tissue, articular cartilage, menisci, and ligaments (Figure 3). We simulated the fibular tunnel for PLC reconstruction to observe the relationship between the fibular tunnel, guide pin, and the CPN. An anatomic fibular tunnel serves as a connection between the centers of the lateral collateral ligament (LCL) and popliteofibular ligament (PFL) footprints. However, the positioning of the tunnel, which is located in proximity to the cortex, puts it at risk of breakage. To mitigate the risk of a shallow tunnel position and potential breakage, we adopted a technique recommended by Tompkins et al3,28 that involves creating a fibular tunnel that connects the anteroinferior side of the LCL footprint with the posteroinferior border of the PFL footprint. During the simulation of fibular tunnel creation, we inserted the guide pin from the anteroinferior side of the LCL footprint toward the posteroinferior border of the PFL footprint. We proceeded to advance the guide pin, simulating the potential risk of inadvertent excessive penetration that could damage the CPN (Figure 4).
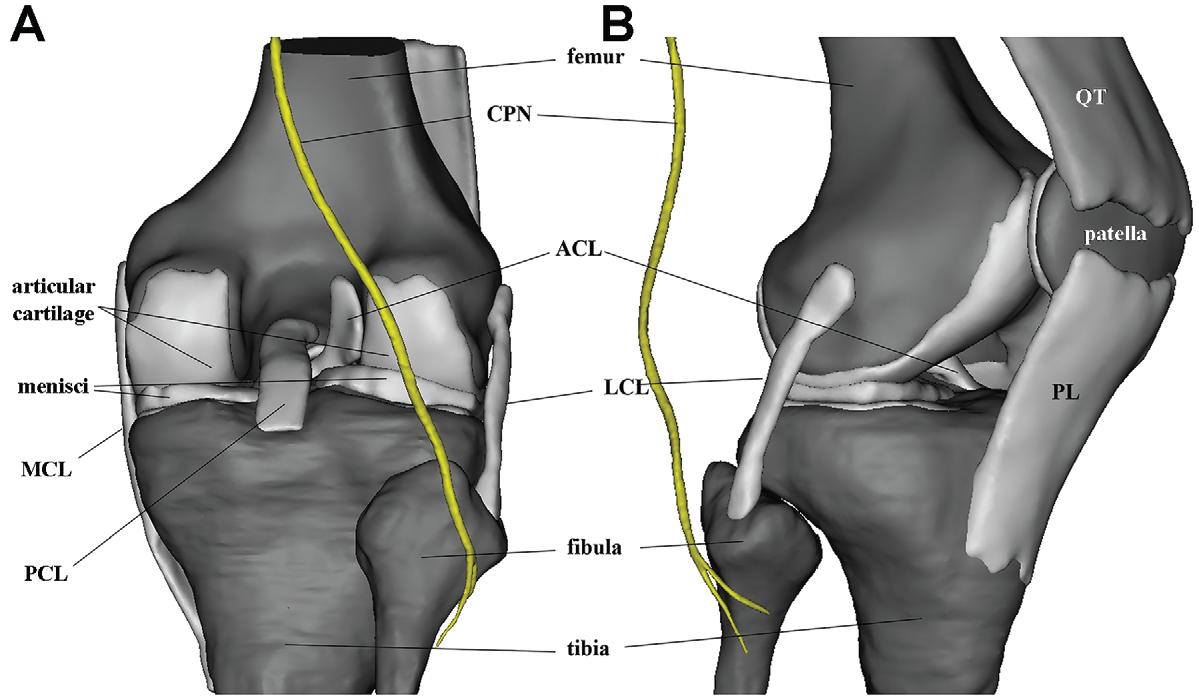
(A) Posterior and (B) anterolateral views of the 3D knee model. ACL, anterior cruciate ligament; CPN, common peroneal nerve; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PL, patellar ligament; QT, quadriceps tendon; 3D, 3-dimensional.

Simulation of the fibular tunnel and the guide pin. (A) lateral view, (B) top view. CPN, common peroneal nerve.
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) Version 22.0 for Windows (IBM). Descriptive statistics were calculated for all parameters. All data were described with means and standard deviations for continuous variables. Two independent observers performed each measurement, and the mean of these 2 values was calculated and used for analysis. The Spearman-Brown prediction method was used to determine the interobserver reliability between the 2 independent observers for all measured parameters, with the value ranging between 0.9347 and 0.9638. The paired Student t test was used to compare the measurements for the different knee flexion angles at different levels. P < .05 was considered statistically significant.
Results
The CPN could be observed in all participants at the 3 measurement levels at 0° to 60° of knee flexion. At a flexion of 90°, the CPN could not be observed at the joint line level in any of the subjects. Furthermore, the course of the CPN could not be observed on the knee MRI at the level of the tibial cut in 1 patient. At a knee flexion of 120°, the course of the CPN was not visible at any measurement level in any patient. Despite not being detected at 3 measurement levels, we identified the CPN positioned within the range of 5.21 to 15.17mm below the fibular tip.
We performed a post hoc power analysis using PASS software (Version 14.0; NCSS Statistical Software) to compare the measurements for the different knee flexion angles at different levels. The analysis results demonstrated that most of the power values were >0.95, indicating that despite the small sample size, this study had sufficient power to detect intergroup differences in the measurements.
MRI Measurements
Distance Between the CPN and the PLC
The shortest mean distances from the CPN to the posterolateral joint capsule at the 3 measurement levels gradually increased from 0° to 60° knee flexion. The shortest mean distances from the CPN to the posterolateral joint capsule at the level of the joint line were 17.08 ± 3.36 mm, 20.63 ± 3.58 mm, and 27.61 ± 7.94 mm at knee flexion angles of 0°, 30°, and 60°, respectively. When the knee was flexed at 90°, we could not detect the CPN course at the joint line level. With the knee flexion increasing, changes in nerve displacement at the joint line level were more evident than those at the tibial cut and fibular tip level (Figure 5).

Graph representing the distance from the CPN to the PLC of the knee at the different knee flexion angles and measurement levels. The CPN could not be seen at the joint line level with the knee flexed at 90°. Error bars represent standard deviations . A-P, anterior-posterior; CPN, common peroneal nerve; M-L, medial-lateral.
Distance Between the CPN and the A-P and M-L Axes
When the knee was flexed at 0°, the shortest distances from the CPN to the A-P axis were 37.60 ± 4.98 mm, 36 ± 4.32 mm, and 34.91 ± 4.70 mm at the level of the joint line, tibial cut, and fibular tip, respectively, and those to the M-L axis were 43.45 ± 4.06 mm, 46.24 ± 4.65 mm, and 48.14 ± 4.65 mm, respectively. When the knee was flexed to 90°, the course of the CPN course could not be detected at the joint line level. The shortest distances from the CPN to the A-P axis at the level of the tibial cut and fibular tip were 66.19 ± 8.27 mm and 62.73 ± 10.52 mm, respectively, and those to the M-L axis were 19.46 ± 9.67 mm and 24.44 ± 8.18 mm, respectively (Figure 6). The CPN was located below the fibular tip when the knee was flexed at 120°. At this level, the nerve was situated 51.96 to 68.63 mm from the A-P axis and 8.8 to 17.06 mm from the M-L axis. The measurements showed a notable variation in the CPN distance from the A-P and M-L axes.
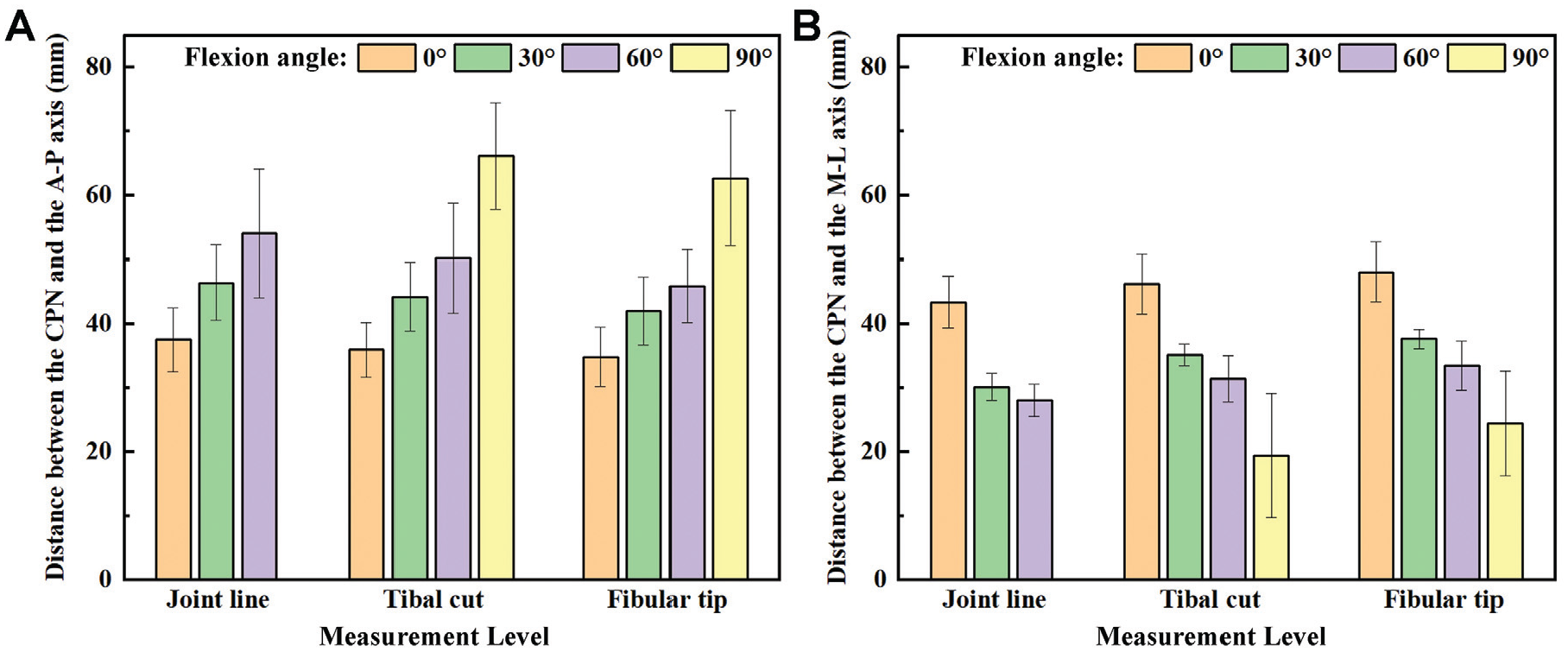
Bar graphs representing the distance from the CPN to the tibial (A) A-P and (B) M-L axes at the different knee flexion angles and measurement levels. The CPN could not be seen at joint level with the knee flexed to 90°. Error bars represent standard deviations . A-P, anterior-posterior; CPN, common peroneal nerve; M-L, medial-lateral; PLC, posterolateral corner.
The mean distances from the A-P and M-L axes to the CPN were significantly different among different knee flexion angles at the different measurement levels. However, the differences in the mean distances from the CPN to the posterolateral border of the tibial plateau were not significant between 0° or 30° of knee flexion (P = .953) at the fibular tip level. The other knee flexion angles demonstrated statistically significant differences in the mean distance from the CPN to the PLC of the tibial plateau at the different measurement levels (Table 1).
Comparison of the Distance From the CPN to the PLC, Tibial A-P Axis, and Tibial M-L Axis of the Knee at Different Flexion Angles (N = 10 Knees) a

Data are reported as mean ± SD. A-P, anterior-posterior; CPN, common peroneal nerve; M-L, medial-lateral; PLC, posterolateral corner.
The CPN could not be detected at the joint-line level when the knee was flexed to 90°.
Statistically significant when compared with 0°.
Statistically significant when compared with 30°.
Statistically significant when compared with 60°.
Relationship Between the CPN, Fibular Tunnel, and Guide Pin
The 3D model revealed that the entrance of the peroneal tunnel was effectively a fulcrum/pivot point for the trajectory of the position of the CPN (Figure 7). As the knee flexion angle increased, the upper part of the CPN moved posteromedially, with more pronounced displacements observed above the joint line. Higher flexion angles led to more noticeable CPN shifts toward the femur midline, signifying its close association with knee flexion.
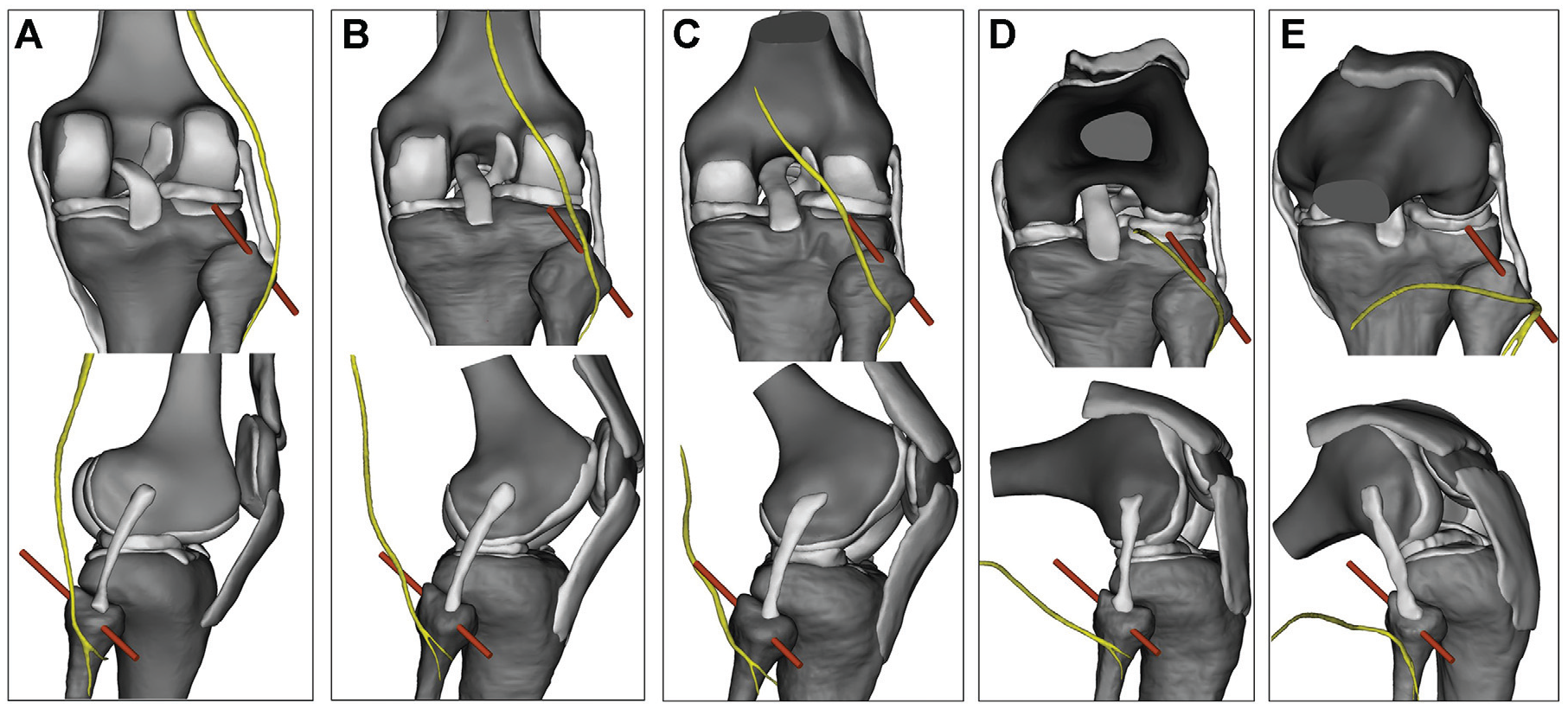
Three-dimensional model simulation of the fibular tunnel for PLC reconstruction, posterior (top row) and lateral (bottom row) views at knee flexion angles of (A) 0°, (B) 30°, (C) 60°, (D) 90°, and (E) 120°. As the flexion angle increased, the distance between the guide pin (red) exit point of the fibular bone tunnel and the CPN (yellow) became longer. CPN, common peroneal nerve; PLC, posterolateral corner.
Furthermore, the positioning of the CPN relative to the guide pin was found to change with knee flexion. In knee extension, the CPN was located on the posterolateral side of the knee joint, approximately 9.33 mm from the guide pin. At 30° of flexion, the CPN shifted medially and posteriorly, progressively approaching the guide pin. At 60° of flexion, the guide pin intersected with the CPN. When the knee reached 90° of flexion, the CPN ran parallel to and below the guide pin. At 120° of flexion, the CPN moved farther from the guide pin, positioning itself below the level of the fibular tip.
In addition, the shortest distance between the guide pin exit point of the fibular bone tunnel and the CPN changed with the knee flexion angle. Specifically, the shortest distance measured 9.33, 4.91, 7.32, 13.88, and 17.02 mm at knee flexion angles of 0°, 30°, 60°, 90°, and 120°, respectively.
Discussion
This is the first study to comprehensively analyze the location and movement of the CPN at different knee flexion angles using thin-slice MRI and by simulating the fibular tunnel drilling performed in reconstruction surgeries. The main finding of the study was that the anatomic course of the CPN in the PLC of the knee changed as the knee flexion angle changed. As the knee joint flexion angle increased, the fibular tunnel acted as a fulcrum, and the CPN moved posteromedially. The closer the CPN was to the distal femur, the more pronounced its posteromedial displacement. As the knee flexion angle increased, the distance from the CPN to the A-P axis and the PLC increased significantly, and the distance from the CPN to the M-L axis decreased significantly at each measurement level (see Table 1). The nerve displacement at the joint line level was more evident than at the tibial cut and fibular tip levels. Therefore, the study findings supported our hypothesis that knee flexion angles affect the anatomic location and course of the CPN at the PLC of the knee joint.
In this study, when the knee was in extension, the shortest distance from the CPN to the posterolateral capsule at the joint line level was 17.02 ± 3.36 mm. At the level of the tibial cut, the shortest distance from the CPN to the posterolateral border of the tibia was 14.57 ± 2.47 mm. At the level of the fibular tip, the shortest distance from the CPN to the posterolateral border of the tibia was 14.38 ± 1.70 mm. These values are very close to the measurements obtained in other studies.5,8,25 However, previous studies on the anatomic relationship between the CPN and the knee mainly implemented knee MRI or were cadaveric studies and evaluated the knee in full extension. Mihalko and Krackow 16 were the first to report on the anatomic location of the CPN relative to the tibia on cadaveric knees. In their study, the distance was found to be 6 to 12 mm at the level of the articular surface in knee extension; when flexed to 90°, the distance from the CPN to the PLC increased, but they did not include specific measurement data in their study. Our results confirm their findings; we also found that the distance from the PLC of the knee to the CPN increased as the knee flexion angle increased.
Clarke et al 5 measured the distance from the CPN to the tibia at the standard tibial cut level on 60 axial knee MRI scans. Their results showed that the mean distance from the CPN to the tibia was 14.9 mm (range, 9.1-21.8 mm). Bruzzone et al 4 measured the distance from the CPN to the PLC at the tibial cut plane after total knee arthroplasty of cadaveric knee specimens. The mean distance measured was 13.5 mm (range, 11.2-18.6 mm). Jia et al 9 measured the shortest distance from the CPN to the joint capsule of the knee PLC at the joint line level and the tibial cut level on MRI. At the joint line level, the closest distance between the CPN and the joint capsule of the PLC was 15.0 ± 2.6 mm (range, 8.5-22.3 mm), and that at the tibial cut level was 14 ± 2.7 mm (range, 8.0-23.2 mm). Jenkins et al 8 measured the distance between the CPN and the posterolateral capsule of the knee on knee MRIs; they found that the mean distance between the CPN and the posterolateral capsule at the level of the tibial cut was 11.9 mm (range, 4.7-22.13 mm). Sankineani et al 25 also used knee MRI to measure the distance between the CPN and the posterolateral joint capsule at the tibial cut level after total knee arthroplasty and obtained a mean distance of 15.55 mm (range, 7.8-26.2 mm).
In the present study, when measuring the shortest distance from the tibia to the CPN, the point where the shortest distance could be measured on the tibia border changed depending on the flexion angle. When the knee was in extension, the point was on the posterolateral side of the tibia, and as the flexion angle changed, the point gradually shifted from the posterolateral tibia to the posterior aspect of the lateral tibial plateau. When the knee was in 90° of flexion, the CPN was below the level of the joint line, and the course of the nerve could not be detected at the level of the joint line. The nerve distance measured at 90° was significantly larger than that at other knee flexion angles. With the knee flexed to 120°, the course of the CPN could not be detected at any of the 3 measurement levels. In our study, the shortest distance between the CPN and the proximal tibia at the 3 measurement levels gradually increased with increasing knee flexion angles.
The measurement results of the relationship between the CPN and the A-P and M-L axes showed that as the knee flexion angle increased, the distance between the CPN and the A-P axis increased substantially. In contrast, the distance between the M-L axis decreased, and the nerve was displaced posteromedially. The farther the CPN runs above the joint line, the more pronounced the tendency to shift posteromedially when flexing the knee. Teo et al 27 used cadaveric knees to assess whether the fibular head is a reliable reference point for identifying the position of the CPN at the PLC of the knee at different degrees of knee flexion (0°, 30°, 60°, 90°, 120°). They found that the CPN was consistently located on the fibular neck, approximately 20.7 ± 1 mm from the tip of the fibular head. Those authors thus concluded that the tip of the fibular head is a consistent landmark that can predict the position of the exit point of the CPN at the knee PLC. However, their study did not describe the anatomic course of the CPN on the PLC of the knee joint and the distance from the tibia to the CPN. Notably, the position of the CPN at the fibular neck is relatively fixed and does not change with the flexion angle of the knee joint. This suggests that the exit point of the CPN at the PLC can be more consistently identified regardless of the knee position. Because the location of the junction of the CPN and the fibular neck cannot be easily located on MRI scans, we did not measure the course of the CPN below the fibular tip in our study.
In the posterior aspect of the knee, the CPN starts at the apex of the popliteal fossa and follows the lateral border of the fossa closely along the medial margin of the biceps femoris and its tendon. It leaves the popliteal fossa by passing superficially to the lateral head of the gastrocnemius, then crosses over the posterior aspect of the head of the fibula, and divides into its terminal branches. During knee flexion, the femoral condyles roll and slide on the tibial plateau, and kinematic studies have revealed that the lateral femoral condyle slides backward more than the medial femoral condyle, leading to internal rotation of the tibia relative to the femur. 12 Using our 3D knee joint model, we were able to visualize this internal rotation. Specifically, we observed that as the knee flexion angle increased, the lateral femoral condyle shifted backward more noticeably than the medial femoral condyle, resulting in the tibia rotating internally relative to the femur.
By constructing a 3D model of the biceps femoris tendon at various knee flexion angles, we were able to observe that the position of the CPN remained relatively fixed as it descended along the biceps femoris and its tendon. Park et al 22 suggested that a tunnel is formed between the biceps femoris muscle and the lateral gastrocnemius muscle, which keeps the CPN relatively fixed at that location and lacks cushioning tissue, making the CPN more susceptible to injury. We also found from the 3D model that as the knee flexes, the biceps femoris muscle moves posteromedially along the longitudinal axis of the femoral shaft, utilizing the fibular head as a pivot point. The biceps femoris muscle's downward and inward movement and the tibia's internal rotation caused the CPN to shift posteromedially (Figure 8). We believe that this is the reason for the observed CPN shift posteromedially during increasing knee flexion angles.

The knee 3D models reveal that when the knee flexes, the biceps femoris muscle moves downward and inward along the femoral shaft's longitudinal axis, utilizing the fibular head as a pivot point. This downward and inward motion of the biceps femoris, in combination with the tibia's internal rotation, causes the CPN to shift downward and backward (CPN-yellow; biceps femoris and its tendon-red). CPN, common peroneal nerve; 3D, 3-dimensional.
If the lateral meniscus is torn in the posterior horn or at the popliteal hiatus, the surgeon will often repair it with a meniscal suture hook; nonetheless, this can injure the CPN if the suture hook is inserted too deeply. Some surgeons suture the posterior horn of the injured lateral meniscus to the popliteus tendon to obtain a more stable suture effect 21 ; however, according to Jenkins et al, 8 58% of CPNs are located just posterior to the popliteus tendon, 34.5% are located lateral to the popliteus tendon, and 7.5% are located medial to the popliteus tendon. Our study results show that by increasing the knee flexion angle, the CPN can be kept away from the PLC of the knee joint. Therefore, when the lateral meniscus is sutured in this area, injury to the CPN can be avoided.
Reconstructive surgery for PLC injuries requires the establishment of a bony tunnel at the head of the fibula, which can also easily injure the CPN. In addition, the current interest and application of minimally invasive techniques for PLC reconstruction could also lead to an increased incidence of CPN injury during surgery because of limited surgical exposure. During PLC reconstruction, special attention should be given to possible CPN injury when the fibular tunnel is drilled, as the method used to establish the bone tunnel differs according to the surgeon's experience. Some surgeons prefer open access, exposing the proximal fibula and CPN to establish the bone tunnel, while others prefer percutaneous needle penetration.1,6,11,13,14,19
In this study, we revealed that the CPN is on the posterolateral side of the knee in extension. In this condition, the CPN is very close to the PLC of the knee joint. When the knee is flexed between 30° and 60°, although the CPN moves farther from the fibular head, it shifts from the posterolateral aspect of the fibular head to the posterior aspect of the fibular head and the lateral tibial plateau. If the bone tunnel is drilled from the inferior anterolateral to the superior posteromedial direction of the fibular head, there is a certain risk of injury to the CPN because of the limited safety distance. When the knee is flexed to 90°, although the CPN is still located on the posteromedial side of the fibular head, it is located far from the surface of the fibular head, allowing the relatively safe establishment of a bone tunnel. When the knee is flexed to 120°, the entire nerve is located below the level of the fibular tip, and it is safest to create a bone tunnel at the head of the fibula.
In a cadaveric experiment, Otani et al 20 found that at high flexion angles, the CPN was farther away from the guide pin. Thus, when drilling a lateral femoral tunnel using the low medial auxiliary approach for anterior cruciate ligament reconstruction, the risk of injury was small. However, as the knee flexion angle decreased, the CPN moved closer to the guide pin, and the risk of nerve injury increased. Therefore, they recommended drilling the posterolateral femoral tunnel through an arthroscopic low medial assisted approach with the knee at 120° of flexion to reduce the risk of CPN injury 20 . Nakamura et al 17 found that when using the far-anteromedial approach to drill the femoral tunnel, a slight flexion angle of the knee joint may put the CPN at potential risk of injury, which decreased with increasing flexion angle of the knee joint. From the results of our measurements and 3D reconstruction model, increasing the knee flexion angle can keep the CPN away from the distal femur and proximal tibia, reducing the risk of direct CPN injury in the posterolateral part of the knee joint. This information may aid surgeons in potentially helping avoid iatrogenic damage to the CPN.
Limitations
As 1 limitation of this study, the sample size was small because it is difficult and time-consuming to collect knee MRI data at different knee flexion angles. The participants recruited for the study were all of medium height; however, the mean height of Chinese men and women is 169.7 and 158 cm, respectively; thus, the results of this study are representative of the course of the CPN in the general Chinese population. To ensure consistency in the research results, the knee joint data collected in this study were all from the right knee. Follow-up research is needed to determine whether there are any bilateral differences in the anatomic relationship between the CPN and the corresponding PLC of the knee joint. Furthermore, the influence of height, weight, and sex on the study findings was not studied.
In addition, our study was primarily theoretical and lacks simple surgical operations as a reference. Therefore, in follow-up studies, the combination of theoretical data and surgical findings will help further improve our understanding of the course of the CPN in the PLC.
Conclusion
The findings of this study indicated that as the knee flexion angle changes, the course of the CPN on the posterolateral aspect of the knee joint also changes. When performing surgical treatment on the posterolateral part of the knee, if conditions permit, increasing the knee flexion angle as much as possible may effectively avoid direct injury to the CPN.
Footnotes
Acknowledgements
The authors would like to thank American Journal Experts for their excellent language editing.
Final revision submitted August 20, 2023; accepted August 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from grants from the National Natural Science Foundation of China (81960399, 82172444), Inner Mongolia Natural Science Foundation (2020MS03064), the Science and Technology Program of Inner Mongolia (2022YFSH0053), and the Medical Health Science and Technology Program of Health Commission of Inner Mongolia (202201050). Y.Q. has received research funding from the National Natural Science Foundation of China. Y.X. has received research funding from the National Natural Science Foundation of China. H.B. has received research funds from the Inner Mongolia Natural Science Foundation, the Science and Technology Program of Inner Mongolia, and the Medicine and Health Science and Technology Program of Health Commission of Inner Mongolia. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Inner Mongolia People's Hospital (ref No. 2022042121).