
Abstract
Background:
Thinner anterior hip capsules are associated with hip laxity, but there is little known about the impact of capsular thickness on the development of instability after primary hip arthroscopic surgery.
Purpose:
To investigate the relationship between hip capsular thickness as measured on preoperative magnetic resonance imaging (MRI) and the development of hip instability after hip arthroscopic surgery for femoroacetabular impingement.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We reviewed revision hip arthroscopic procedures performed between January 1, 2019, and May 1, 2021, at a single institution. Inclusion criteria were preoperative MRI/magnetic resonance arthrography, completion of the study traction protocol, and asymmetric distraction between the hips of ≥3 mm on examination under anesthesia. A comparison group of patients treated for femoroacetabular impingement with primary hip arthroscopic surgery who did not develop capsular instability were matched 1:1 to the patients with instability. Superolateral hip capsular thickness was measured on MRI before index surgery. Analysis was conducted using independent-samples t tests and multivariable linear regression.
Results:
A total of 44 patients were included, with 22 patients each in the instability and no-instability groups. The mean capsular thickness was lower in the patients with hip instability than in those without (1.9 ± 0.6 vs 3.4 ± 1.1 mm, respectively; P < .001). Decreased capsular thickness was significantly associated with hips with instability versus no-instability (β = −1.468 [95% CI, –2.049 to −0.887]; P < .001).
Conclusion:
Thinner preoperative hip capsules in the region of the iliofemoral ligament were seen in patients who subsequently underwent revision arthroscopic surgery for hip instability compared to patients who underwent primary hip arthroscopic surgery without subsequent revision. Patients at a higher risk for the development of postoperative hip instability had a superolateral hip capsular thickness of <2 mm.
Keywords
Classically, the hip is considered a constrained joint, with its stability achieved by both osseous congruity between the femoral head and acetabulum as well as nonosseous structures, including the acetabular labrum, ligamentum teres, and hip capsule ligaments.20,29,32 Of these ligaments, the iliofemoral ligament has been widely accepted as the primary soft tissue restraint.22,32 Disruption of these ligaments reduces hip stability, with defects in the capsuloligamentous structure being associated with hip instability and increased hip distraction.6,12,21,36 Capsular repair has been previously shown to be important in terms of restoring native capsule biomechanics 25 and improving patient outcomes in the postoperative setting, furthering the importance of the hip capsule in overall hip stability.4,10,11,34
While the hip is regarded as an inherently stable joint, there has been recent investigation into the characterization of hip instability; these topics have come to the forefront as a result of increased recognition of their clinical importance. Recent studies have demonstrated worse outcomes in those patients experiencing hip instability15,23,24,34 and an overall rise in the utilization of hip arthroscopic procedures.5,7,17,19 While there is continued debate on an objective definition of hip instability, a generally accepted definition for the diagnosis of hip instability is painful, extraphysiological movement of the hip joint. 30 Demographic characteristics have also been associated with joint laxity, including hip dysplasia and female sex.9,36 It has also been shown in women that intraoperative joint laxity is associated with a thinner hip capsule as measured on magnetic resonance imaging (MRI).18,26
Despite this increased focus on hip instability, there has yet to be an in vivo evaluation of the relationship between hip capsular thickness in patients who undergo primary hip arthroscopic surgery and subsequently go on to develop instability requiring revision surgery. Although it has been previously demonstrated that thinner anterior capsules are associated with clinical hip instability13,16,26 and that patients with femoroacetabular impingement (FAI) have varying thicknesses of the hip capsule, 18 the clinical ramifications of capsular thickness and its impact on instability after primary hip arthroscopic surgery are still poorly understood.
The primary aim of this study was to investigate the relationship between hip capsular thickness as measured on preoperative MRI and the development of instability after hip arthroscopic surgery for FAI. We hypothesized that patients who underwent revision hip arthroscopic surgery for instability would have thinner hip capsules, as measured before primary hip arthroscopic surgery, compared to patients who did not require a subsequent revision procedure for the development of hip instability.
Methods
Participants
The study protocol received institutional review board approval. All revision hip arthroscopic procedures performed by the senior author (S.K.A.) between January 1, 2019, and May 1, 2021, were reviewed to establish a population of patients with hip instability (instability group). Study inclusion criteria were (1) asymmetric distraction between the operative and contralateral hips on examination under anesthesia before instrumentation during the revision procedure, defined as a difference of ≥3 mm21,31 between the surgical and contralateral hips at 45.4 kg of traction; (2) preoperative MRI or magnetic resonance arthrography (MRA) of the operative hip before the index hip arthroscopic procedure; and (3) completion of the traction protocol during revision hip arthroscopic surgery. Exclusion criteria were (1) lack of appropriate preoperative imaging and (2) incompletion of the traction protocol (described below). Of note, patients who underwent revision hip arthroscopic surgery with the senior author had several potential indications for revision such as hip pain or subjective hip joint instability, but patients with hip instability were diagnosed intraoperatively on examination under anesthesia using the above objective distraction criterion. Informed consent was not formally obtained for this study as the traction protocol is standard of care for all primary and revision hip arthroscopy patients in the senior author’s practice.
To generate a comparator group (no-instability group), patients who underwent primary hip arthroscopic surgery by the senior author for FAI were queried from a personal case database over the same period as the instability group. Inclusion criteria were (1) completion of the study traction protocol and (2) preoperative MRI or MRA of the operative hip before the index hip arthroscopic procedure. Exclusion criteria were (1) previous hip surgery and (2) subsequent revision hip arthroscopic surgery for any indication. Data in the electronic medical record were reviewed to determine if the patients were subsequently seen for revision hip arthroscopic surgery, and follow-up clinic notes were checked for symptoms of instability. The follow-up time was calculated as the duration in months from initial surgery to final follow-up. Patients in the no-instability group were included and matched to those in the instability group in a 1:1 fashion based on age, sex, and body mass index (BMI) after a manual review of patient records.
Axial Distraction Testing by Physical Examination
Patients in the instability group underwent axial distraction testing in the clinic by the senior author before revision surgery. Testing was performed with the patient supine on the examination table with the patient's pelvis stabilized by the examiner placing his knee on the patient's ischium. The patient's hip and knee were passively flexed to 45° and 90°, respectively, and an axial distraction force was applied to the hip joint. Hip instability was indicated by patient-reported hip pain, apprehension, or toggle. 24
Radiographic and Imaging Evaluation
Preoperative anteroposterior (AP) radiographs were utilized to calculate the total distraction distance visualized on fluoroscopy (described below) and to obtain the lateral center-edge angle to the acetabular sourcil using previously described methodology.33,35 Hip capsular thickness was measured on MRI or MRA before the index hip arthroscopic procedure in all study patients to minimize the influence of prior capsular instrumentation in the instability group, given their previous arthroscopic procedures. An example of these measurements is provided in Figure 1, with the measurements being made along the superolateral aspect of the hip capsule in the coronal plane on the T2-weighted image that contained the widest portion of the femoral head. Measurements of the hip capsule were performed in 3 discrete regions and averaged together for final analysis: immediately proximal to the zona orbicularis, at the level of the acetabular labrum, and at a midpoint between these 2 anatomic landmarks. This region of the hip capsule was chosen to approximate the iliofemoral ligament and was thought to likely represent the most clinically significant measurement of the hip capsule, given the previously established importance of this ligament. Radiographic and capsular measurements were made by 3 trained reviewers (S.M.O., D.L.F., T.R.S.), with the capsular measurements made using a previously published method with intraclass correlation coefficient values of >0.90. 18

Representative image of capsular measurements on a T2-weighted magnetic resonance arthrogram of a right hip in a patient from the no-instability group. Measurements were made in the coronal plane on the image that contained the widest portion of the femoral head at 3 sections of the hip capsule: just proximal to the zona orbicularis (blue line), at the level of the acetabular labrum (white line), and at a midpoint between these 2 lines (yellow line). These measurements were averaged to generate a value of capsular thickness for each patient.
Operative Protocol and Total Distraction Distance Measurements
Before hip arthroscopic surgery in both groups, patients underwent induction under general anesthesia and were positioned supine on a foam pad on a Pivot Guardian hip distraction table (Stryker), which is a post-free traction system with a built-in tensiometer. The tensiometer was calibrated using free weights at 11.3-kg force intervals up to 45.4 kg to confirm the accuracy of the tensiometer. The patients’ leg position was neutral, in line with their torso (0° of flexion/extension, 0° of abduction/adduction, and 0° of rotation). Fluoroscopic images were obtained utilizing an OEC 9900 Elite mobile C-arm (GE Healthcare) and were captured before instrumentation of the hip at 11.3-kg force intervals from 0 to 45.4 kg. An identical traction system and the same C-arm model were utilized for all patients in our study to minimize potential errors across patients.
The joint space was measured and distraction calculated according to previously published methodology, utilizing preoperative AP radiographs and intraoperative fluoroscopic images of the operative hip using the equation below.18,21,25 Patients in the instability group underwent the traction protocol bilaterally, which allowed for the assessment of asymmetric joint distraction to identify capsular instability. The joint space and femoral head diameter were measured on fluoroscopic images obtained immediately after an increase in traction at each traction interval. The joint space was measured from the shortest distance between the most lateral aspect of the acetabular sourcil and the superolateral femoral head at each traction interval, with pixels as the unit of measurement. The femoral head diameter was measured on preoperative AP radiographs using a best-fit circle of the femoral head, with the measurement in millimeters. Fluoroscopic image measurements were converted from units of pixels to millimeters using preoperative radiographs and the following equation to calculate the joint space at 0 and 45.4 kg of axial traction:
The total distraction distance of the hip was calculated as the difference between the joint space values at 45.4 kg of axial traction and 0 kg of axial traction. All distraction measurements were made by a trained reviewer (A.K.M.).
Statistical Analysis
All analyses were carried out using SPSS (Version 28; IBM). Before analyses, continuous variables were assessed for normality using the Shapiro-Wilk test. Independent-samples t tests were used to compare normally distributed continuous variables, with chi-square tests utilized for categorical variables. Multivariable linear regression was performed using capsular thickness and total distraction distance as dependent variables in separate models. Based on our sample size, the critical Pearson correlation coefficient values for our linear regression were r = 0.251 for a P value of .05 and r = 0.350 for a P value of .01. 28 Our regression analyses were estimated to be sufficiently powered to detect a statistically significant difference using the rule of 10 participants per variable in the final model. 2 A P value of <.05 was used as the threshold to indicate statistical significance.
Results
After a review of 100 operative cases over the study time frame, 22 hips in 22 patients were included in the instability group, with 29 hips excluded for a lack of complete fluoroscopic images, 46 hips excluded for no evidence of hip instability on examination under anesthesia, and 3 hips excluded for unavailable MRI or MRA. A total of 44 hips were obtained after matching and the inclusion of 22 patients from the no-instability group, with a mean follow-up of 13.9 ± 4.5 months (Figure 2).
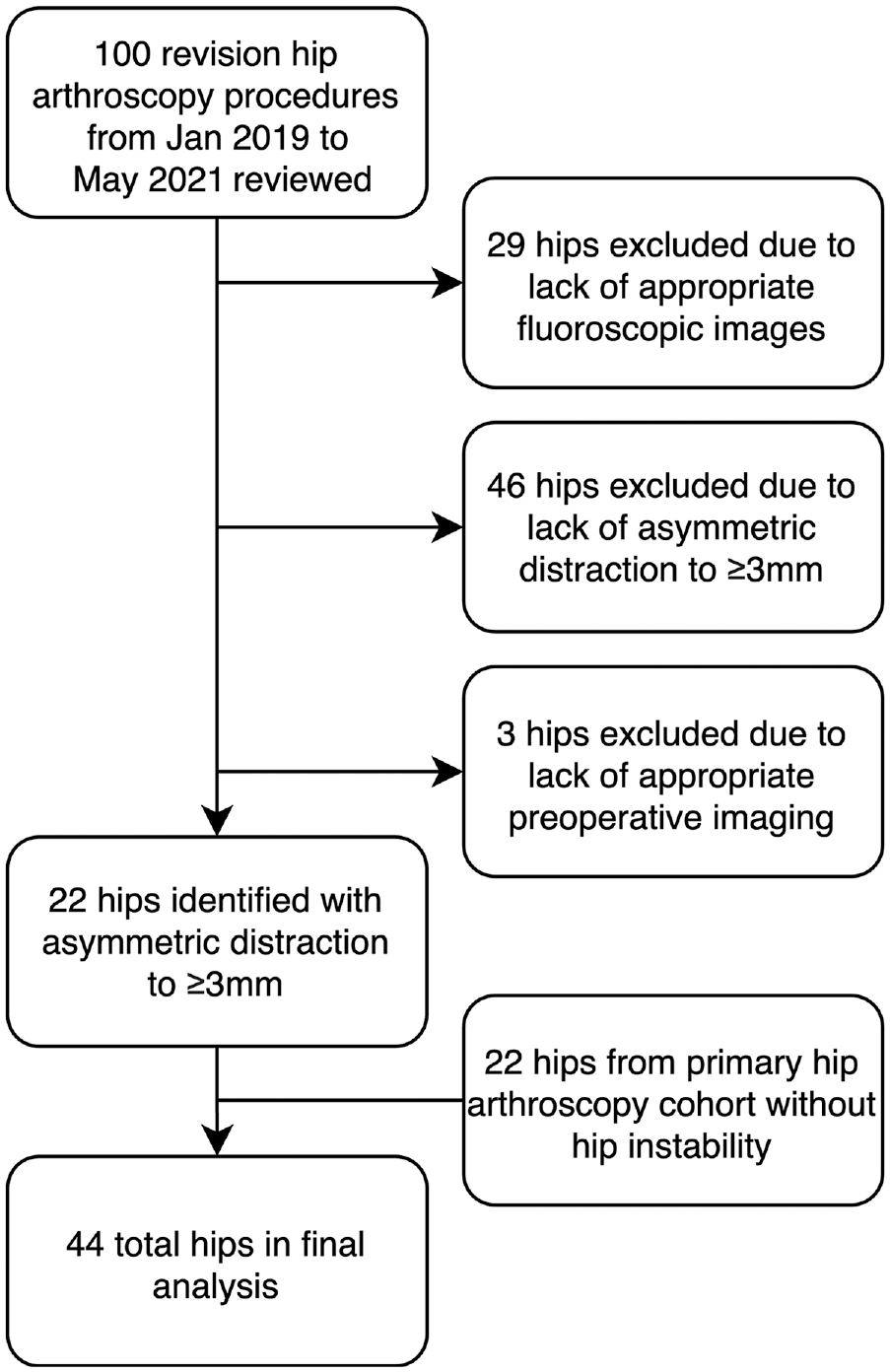
Flow diagram showing the selection of study groups. There were 100 revision arthroscopic cases initially reviewed for inclusion, with 22 meeting the inclusion criteria. Overall, 22 hips that underwent primary hip arthroscopic surgery were matched based on age, sex, and body mass index for the final inclusion and analysis of 44 total hips.
Patient demographic and radiographic data are presented in Table 1. The mean age of all patients was 29.6 ± 9.6 years, and the mean BMI was 25.6 ± 5.5 kg/m2. Of the 44 patients included, 42 (95.5%) were female. There were 26 (59.1%) right and 18 (40.9%) left hips between the 2 groups. Patients were 100% sex matched between the 2 groups, with a mean difference in age of 3.5 years and a mean difference in BMI of 0.8 kg/m2 between groups.
Characteristics of Patients a

Data are reported as mean ± SD or n (%). Boldface P value indicates a statistically significant difference between groups (P < .05). BMI, body mass index.
Beighton scores available in 28 (63.6%) patients.
Results of the preoperative physical examination for instability are shown in Table 2. Of the 22 patients in the instability group, 20 (90.9%) patients self-reported feelings of hip instability. On axial distraction testing, 14 (63.6%) had pain, 16 (72.7%) had apprehension, and 16 (72.7%) had an objective toggle. Only 2 (9.1%) patients in the no-instability group reported pain on axial distraction testing, with no patients experiencing instability symptoms, apprehension, or an objective toggle (P < .001 for all).
Axial Distraction Testing Findings a

Data are reported as n (%).
Independent-samples t tests demonstrated significant differences in both capsular thickness and total distraction distance between the study groups. Capsular thickness was found to be lower in the instability group compared with the no-instability group (1.9 ± 0.6 vs 3.4 ± 1.1 mm, respectively; P < .001) (Figure 3). Total distraction distance at 45.4 kg of axial traction was found to be higher in the instability group compared with the no-instability group (10.9 ± 2.6 vs 8.6 ± 2.5 mm, respectively; P = .004).
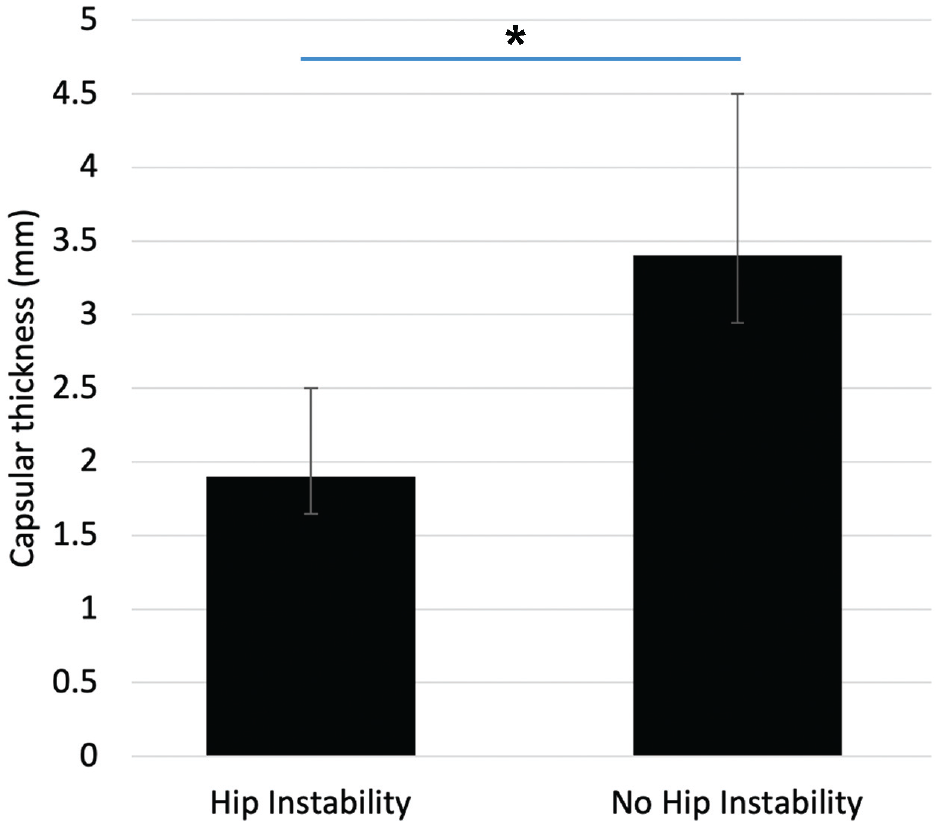
Bar graph showing the mean difference in capsular thickness between the instability and no-instability groups. Error bars represent the 95% confidence interval for the standard error of the mean. The no-instability group was found to have a significantly higher mean capsular thickness compared to the instability group (*P < .001; independent-samples t test).
Several associations of hip capsular thickness with hip instability were identified through multivariable linear regression analysis (Table 3). A thinner hip capsule measured before index surgery was significantly associated with hips that subsequently underwent revision surgery for capsular instability (β = −1.468 [95% CI, −2.049 to −0.887]; r = 0.663; P < .001), while there was no significant association of age, BMI, or lateral center-edge angle to the sourcil with the development of postoperative hip instability requiring revision surgery.
Results of Multivariable Linear Regression Analysis With Capsular Thickness as Dependent Variable a

Pearson correlation coefficient (r) = 0.663; coefficient of determination (R 2 ) = 0.440. Boldface P value indicates a statistically significant difference (P < .05). BMI, body mass index.
Discussion
The findings of this study demonstrated an association between thinner hip capsules in the region of the iliofemoral ligament and patients who underwent revision hip arthroscopic surgery with asymmetric distraction on examination under anesthesia. This supports our hypothesis that thinner preoperative hip capsules measured before index hip arthroscopic surgery would be seen in patients who subsequently underwent revision hip arthroscopic surgery for capsular instability compared to patients who underwent primary hip arthroscopic surgery without subsequent revision procedures.
It has been previously demonstrated that thinner hip capsules are associated with hip joint laxity and clinical instability.8,13,16,18,26 Magerkurth et al 16 examined a cohort of 27 patients who underwent hip arthroscopic surgery, reporting that those diagnosed with hip laxity at the time of surgery, determined by assessing the distraction difference between the symptomatic and asymptomatic hips, were associated with thinner anterior hip capsules on MRA. In a similar study, Packer et al 26 examined a cohort of 62 patients undergoing hip arthroscopic surgery and their association with anterior hip capsular thickness and hip laxity, which was diagnosed intraoperatively by utilizing a minimal amount of traction to distract the hip (often the patient's body weight) or the absence of hip reduction when under traction and after the release of negative intra-articular pressure, finding that female patients were associated with both intraoperative laxity and a decreased anterior capsular thickness on MRA. An in vivo study by Devitt et al 8 examined the association between capsular thickness measured intraoperatively during hip arthroscopic surgery of the iliofemoral ligament and the preoperative Beighton score, finding that patients with higher Beighton scores, and thus increased joint laxity, were associated with thinner hip capsules.13,16,18,26 The present study builds on these previous studies by providing an objective characterization of both hip capsular thickness and hip instability on examination under anesthesia. Additionally, the study results demonstrated an association between thinner hip capsules, specifically in the region of the iliofemoral ligament, and the development of hip instability requiring revision hip arthroscopic surgery. It is also worth noting that in the present study, there were no group differences in Beighton scores, with overall low mean values, suggesting that the changes in hip laxity at the time of revision may have been more likely to be iatrogenic in nature. Our study findings suggest that preoperative capsular thickness measurements may be used to evaluate the risk of subsequent hip instability in clinical practice.
Distraction of the hip has been previously investigated in the revision hip arthroscopic setting. A study by Mortensen et al 21 examined the difference in the distraction profile between hips undergoing revision hip arthroscopic surgery and contralateral asymptomatic hips, finding that a majority of patients undergoing revision hip arthroscopic surgery had increased distraction on examination under anesthesia in the operative hip compared to their asymptomatic hip. Similar to their study, we found increased distraction in the revision setting in the instability group compared with their contralateral hip. The present study builds on the study of Mortensen et al 21 by extending the analysis to include a matched group of patients who did not develop hip instability and exploring the association of hip instability with hip capsular thickness, finding that decreased capsular thickness at primary hip arthroscopic surgery was associated with the subsequent development of hip instability on examination under anesthesia.
Overall, our study results suggest that it is important to consider hip capsular thickness in patients undergoing primary hip arthroscopic surgery and its potential contribution to the development of hip instability. The results demonstrate that patients with thinner hip capsules may be at an increased risk of iatrogenic instability after hip arthroscopic surgery. This is an especially important consideration when performing these procedures, given the inherent violation of the capsule during hip access and instrumentation. While further prospective work is needed in this area, caution should be utilized when performing hip arthroscopic surgery in patients with thinner hip capsules. Surgeons should strongly consider capsulotomy techniques that minimize capsular disruption and perform hip capsular repair in this patient population, especially given that prior research has demonstrated the restoration of capsular stability after hip capsular repair both in cadaveric and in vivo analyses.1,3,14,25,27
Limitations
There are several limitations to the current study that warrant consideration. First, the patient sex distribution was skewed female (95.5%). Second, 3 patients identified to have hip instability were subsequently excluded from final analysis because of unavailable MRI or MRA. Third, not all preoperative imaging was performed at our institution, resulting in a lack of a standardized imaging protocol. Fourth, patients included in the no-instability group were not contacted directly and asked questions regarding symptoms suggestive of hip instability; rather, they were solely reviewed through the electronic medical record, leaving the potential that some of these patients may have developed hip instability after hip arthroscopic surgery and did not present to our institution. Fifth, we were unable to fully assess initial indications for hip arthroscopic surgery or capsular management during index surgery in the no-instability group, including capsulotomy type and method of capsular repair, as the majority of these index procedures were not performed by the senior author but at outside institutions.
Conclusion
Thinner preoperative hip capsules in the region of the iliofemoral ligament were seen in patients who subsequently underwent revision arthroscopic surgery for hip instability compared to patients who underwent primary hip arthroscopic surgery without subsequent revision. Patients at a higher risk for the development of postoperative hip instability had a superolateral hip capsular thickness of <2 mm.
Footnotes
Final revision submitted August 18, 2023; accepted August 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.A. has received consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Utah (No. IRB_00055341).