
Abstract
Background:
Given the variability of the questions asked, the Patient-Reported Outcomes Measurement Information System (PROMIS) upper extremity (UE) computer adaptive test (CAT) Version 2.0 item bank aids in the evaluation of rotator cuff repair (RCR) rehabilitation by determining when recovery milestones are possible based on the quality of patient responses at certain time points.
Purpose:
To assess the time point at which patients with RCR were able to achieve specific functional milestones, determined as positive responses to the 5 most frequently asked items on the PROMIS UE CAT Version 2.0.
Study Design:
Case series; Level of evidence, 4.
Methods:
The postoperative PROMIS UE CAT Version 2.0 scores of patients who underwent RCR between February 16, 2017, and July 30, 2019, were reviewed with respect to individual PROMIS item, response, and timing of response. A functional milestone was considered achieved if the patient response was “without any difficulty” or “with a little difficulty” to any of the 5 most frequently asked PROMIS items. The percentage of patients in each monthlong postoperative interval who answered with either response was recorded. The logit generalized estimating equations method was used to analyze the association between milestone achievement for each PROMIS item and predictor variables (age, sex, body mass index, smoking status, race, ethnicity, and employment status).
Results:
A total of 1131 responses from 371 patients were included. The majority of patients attained milestone achievement on 4 of the 5 most frequently asked PROMIS items at time points ranging from 1 to 5 months postoperatively: “Are you able to carry a shopping bag or briefcase?” (by 1 month), “Are you able to put on and take off a coat or jacket?” (by 3 months), “Are you able to pour liquid from a bottle into a glass?” (by 3 months), and “Are you able to carry a heavy object (over 10 pounds/5 kg)?” (by 5 months). For the item “Are you able to put on a shirt or blouse?”, the majority of patients did not achieve the milestone by 1 year.
Conclusion:
These findings support the application of PROMIS UE CAT Version 2.0 milestone achievement in the shared decision-making process and postoperative monitoring, as patients can use this information to determine when they can return to certain activities and providers can apply these standards to identify patients needing additional clinical support.
Keywords
Rotator cuff pathology is the most common tendon injury in the adult population, accounting for up to 70% of all shoulder-related visits to physicians.15,21 Rotator cuff tears have been found to be present in >50% of people between 60 and 81 years of age, with incidence increasing with age and influenced by smoking, manual labor, and previous trauma.22,24,27 Rotator cuff repair (RCR) is a common treatment for rotator cuff tears, with 250,000 to 300,000 repairs being performed in the United States, the majority of which are arthroscopic.2,11 The use of arthroscopic RCR to treat rotator cuff tears is increasing dramatically and has demonstrated durable midterm and long-term results.2,12
As a major goal of RCR is the restoration of functionality of the affected shoulder, it is important for patients and providers to understand how to assess postoperative function after this procedure. A variety of patient-reported outcome measures have been used to measure various functional domains after RCR, including the American Shoulder and Elbow Surgeons standardized shoulder assessment form, the Single Assessment Numeric Evaluation, and the Constant-Murley score. The Patient-Reported Outcomes Measurement Information System (PROMIS) outcome measures were developed in 2004 by the National Institutes of Health to measure outcomes across various domains such as physical health, mental health, and social health. The PROMIS computer adaptive tests (CATs) use integrated response theory to select questions from a standard item bank based on previous patient answers through a predetermined algorithm.1,23 PROMIS CATs thereby provide generalizable outcome measures across multiple domains, which reduces the number of individual questions compared with legacy patient-reported outcome measures. 26 As the current health care climate emphasizes value-based care and a patient-centered approach, PROMIS CATs have become increasingly popular among orthopaedic surgeons treating shoulder pathology. 4 PROMIS scores have been shown to demonstrate responsiveness and correlate with legacy patient-reported outcome measures across all domains in patients who have undergone RCR.3,4,19
Assessing functional milestones after RCR is paramount to determining recovery trajectories in order to individualize care. In this way, providers are able to track the progress of individual patients and identify and address outliers at an early stage. Understanding their own recovery timeline and milestone achievement may provide a psychological benefit to patients as well. 17 Despite these benefits, the time at which patients achieve postoperative functional milestones after RCR remains unknown. Because of the variability of the questions asked, the PROMIS UE CAT Version 2.0 item bank aids can be utilized in the evaluation of RCR rehabilitation by determining when recovery milestones are possible based on the quality of responses at certain time points.
The purpose of this study was to use the PROMIS Upper Extremity (UE) CAT Version 2.0 form to determine the postoperative time points at which patients reach specific functional milestones after RCR, defined as positive responses to the 5 most frequently asked questions in the PROMIS UE CAT Version 2.0 questionnaire. We hypothesized that the majority of patients would achieve functional milestones by 3 months postoperatively.
Methods
The study protocol of this retrospective case series study received institutional review board approval. All patients who underwent primary RCR by 1 of 3 sports medicine fellowship-trained orthopaedic surgeons (E.C.M., V.M.) at our institution between February 16, 2017, and July 30, 2019, were included in this study. At our institution, the postoperative RCR rehabilitation course typically involves 2 weeks of immobilization in a sling and 12 weeks of physical therapy starting at 1 week postoperatively. Patient-reported outcome measures were administered by research assistants and then digitally stored by utilizing REDCap (Vanderbilt University), which is a secure web-based application service. 5 Preoperative PROMIS scores and patients who did not communicate in English or were physically unable to complete the form were excluded from the study. All patients enrolled provided informed consent.
PROMIS UE CAT Version 2.0 forms administered to patients comprised questions selected from a standard 45-item question bank through a predetermined algorithm considering previous patient answers.1,23 Given the adaptive design of the PROMIS UE CAT Version 2.0 form, patients completed unique forms with different lengths and question items. Postoperative PROMIS UE CAT Version 2.0 forms were reviewed with respect to individual item, response, and timing of response (with respect to the number of days after surgery using monthlong intervals). Responses were collected at each postoperative orthopaedic clinic appointment scheduled by the patient. For all PROMIS CAT Version 2.0 forms, a score of 50 represents a healthy patient, and a standard deviation is represented by a 10-point increase or decrease in score. For each PROMIS UE CAT Version 2.0 item, patients could choose from among the following 5 answer choices: “without any difficulty,”“with a little difficulty,”“with some difficulty,”“with much difficulty,” and “unable to do.” A response of “without any difficulty” or “with a little difficulty” was considered milestone achievement. The percentage of patients in each monthlong interval who answered with either of these responses was recorded.
Statistical Analysis
Descriptive statistics were described using means, standard deviations, counts, and percentages. The time effect of postoperative milestone achievement for each respective PROMIS item considered was assessed using descriptive statistics. The logit generalized estimating equations method was used to handle repeated-measures data and analyze the association between the probability of milestone achievement for each PROMIS item and patient characteristics; predictor variables assessed included age, sex, body mass index (BMI), smoking status, race, ethnicity, and employment status. An alpha level of <.05 was considered indicative of statistical significance. All analyses were completed in SAS Version 9.4 (SAS Institute Inc).
Results
A total of 1131 patient responses from 371 unique patients were included in the final analysis. Patient characteristics are displayed in Table 1. The number of PROMIS UE CAT Version 2.0 forms completed at each specific postoperative time point is displayed in Table 2.
Characteristics of the Study Cohort (N = 371 Patients) a

Data are reported as mean ± SD or n (%).
PROMIS Responses According to Postoperative Time Point (N = 1131 Responses) a

PROMIS, Patient-Reported Outcomes Measurement Information System.
The 5 most frequently asked questions in the PROMIS UE CAT Version 2.0 item bank were as follows: “Are you able to carry a heavy object (over 10 pounds/5 kg)?” (n = 1131), “Are you able to put on and take off a coat or jacket?” (n = 922), “Are you able to carry a shopping bag or briefcase?” (n = 450), “Are you able to pour liquid from a bottle into a glass?” (n = 666), and “Are you able to put on a shirt or blouse?” (n = 571). The postoperative times at which patients achieved various milestone thresholds are shown in Table 3. Figure 1 displays the percentage of patients who achieved milestones for each PROMIS item within 1 year postoperatively. All study patients achieved the milestones on the 5 most frequently asked questions on the PROMIS UE CAT Version 2.0 form by 1 to 5 months postoperatively, with the exception of the question “Are you able to put on a shirt or blouse?” (Table 3).
Postoperative PROMIS Milestone Achievement a
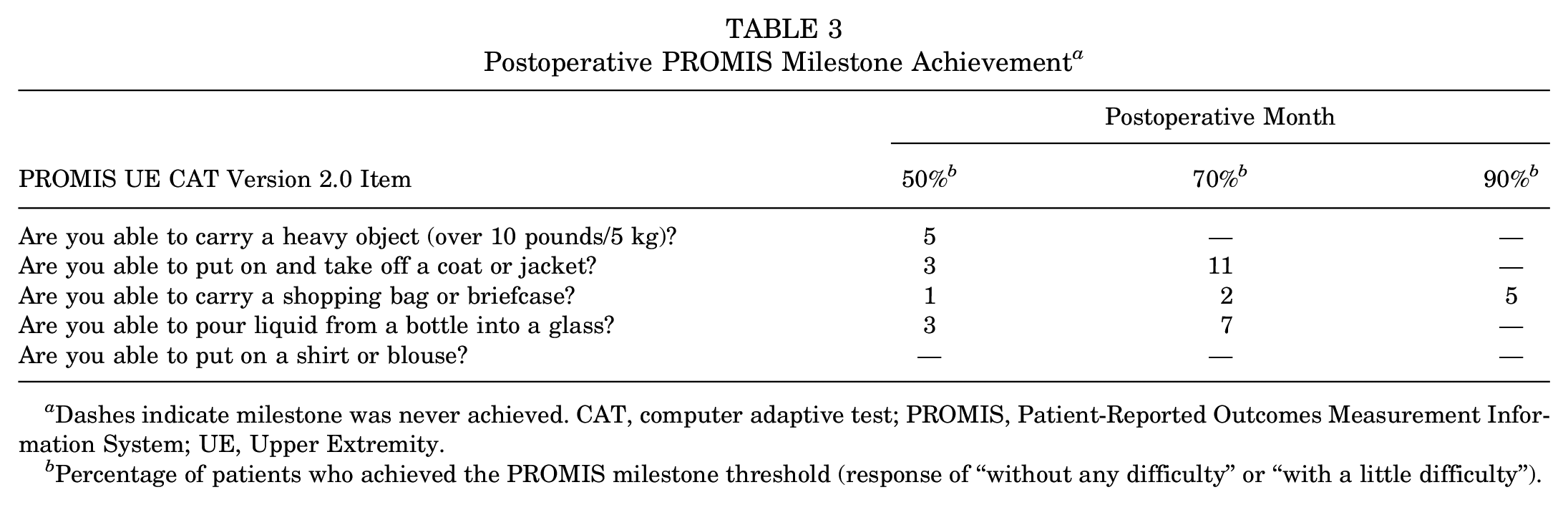
Dashes indicate milestone was never achieved. CAT, computer adaptive test; PROMIS, Patient-Reported Outcomes Measurement Information System; UE, Upper Extremity.
Percentage of patients who achieved the PROMIS milestone threshold (response of “without any difficulty” or “with a little difficulty”).

Scatterplots showing the percentage of patients who achieved the Patient-Reported Outcomes Measurement Information System milestone on the 5 most frequently asked questions according to months postoperatively.
Female sex (odds ratio [OR], 2.10 [95% CI, 1.52-2.90]; P < .001), Black/African American race (OR, 2.04 [95% CI, 1.38-3.01]; P < .001), and increased BMI (OR, 1.03 [95% CI, 1.01-1.06]; P = .019) were shown to be associated with greater milestone achievement corresponding to the item “Are you able to carry a heavy object (over 10 pounds/5 kg)?” (Supplemental Table S1, available separately). Increased age (OR, 0.98 [95% CI, 0.97-1.00]; P = .027) was associated with greater milestone achievement for the item “Are you able to pour liquid from a bottle into a glass?” (Supplemental Table S1). No associations with age, sex, race, ethnicity, smoking status, BMI, or employment status were found in the other PROMIS items considered.
Discussion
In this study, the majority of patients appeared to progress to functional improvement at 1 to 5 months after RCR. By 1 month postoperatively, the majority of patients were able to carry a shopping bag and briefcase. By 3 months postoperatively, at least 50% of patients were able to put on or take off a coat or jacket and to pour liquid from a bottle into a glass. Only by 5 months after RCR were patients able to carry heavy objects (over 10 pounds/5 kg). Of note, the majority of patients who responded were not able to put on a shirt or blouse at 1 year postoperatively.
PROMIS CAT forms have compared favorably to traditional patient-reported outcome measures because of the strong content validity, high efficiency, and high responsiveness to change.7,8,10 For UE patients in particular, PROMIS CAT forms have shown high efficacy when compared with UE legacy instruments such as the Disabilities of the Arm, Shoulder and Hand (DASH) and QuickDASH.18,25 PROMIS UE CAT is particularly supported as an efficient assessment tool in the UE patient population, especially for patients undergoing RCR.3,9,19 Furthermore, preoperative PROMIS UE CAT scores have been shown to have predictive ability of achieving minimal clinically important differences in patients with RCR. 6 Based on the high construct validity of PROMIS UE CAT Version 2.0, it is a widely applicable quantitative metric in assessing RCR recovery.
This study used the 5 most frequently asked questions in the PROMIS UE CAT Version 2.0 item bank in order to determine functional milestone achievement after RCR. Previous studies utilized a variety of different criteria to similarly assess postoperative RCR functional milestones. For instance, MacDermid et al 16 cited various physical therapy measures such as sling removal and initiation of strengthening and endurance exercises as indicators of recovery. Similarly, Kim et al 14 evaluated recovery by considering not only qualitative observations such as body motion range, performance of strength-related activities, and return to athletic activities, but also quantitative metrics such as the University of California–Los Angeles and the American Shoulder and Elbow Surgeon scores. Other quantitative measures of recovery include the Simple Shoulder Test, visual analog scale for pain, and 36-item Short Form Health Survey.13,20 While quantitative metrics have been used in assessing RCR milestone achievement, further investigation into the interpretation and utilization of such tools is necessary. Our study works toward this aim by supporting how PROMIS is a validated tool capable of identifying functional milestone achievement after RCR. Our findings provide a basis for orthopaedic providers to apply PROMIS item responses in order to compare patient progress to an objective standard while controlling for outliers, thereby enabling personalized care for each individual patient as a result. Furthermore, our work can lead to follow-up studies that utilize PROMIS item responses to better assess important follow-up metrics in patients with RCR, such as maximum outcome improvement and maximal medical improvement.
Understanding PROMIS milestone achievement in patients with RCR is also key to the shared decision-making process regarding whether surgery is appropriate for certain patients. In particular, milestone achievement information will be highly useful to patients with occupational or other essential requirements that necessitate a specific return to functional activity. For example, the preoperative consultation for a patient with a rotator cuff tear whose profession involves significant physical activity can include a discussion on how return to improved function will take around 4 months after surgery. Based on this information provided during the shared decision-making process, this patient is able to better evaluate treatment options while also considering the requirements for his or her livelihood. Furthermore, postoperative monitoring can incorporate PROMIS milestone achievement, with patients not achieving milestones at respective time points then being provided the appropriate additional clinical care.
Limitations
There are a number of limitations of this study to note. Preoperative PROMIS UE CAT Version 2.0 scores were not taken into consideration when evaluating milestone achievement. It is possible that milestone achievement was influenced by variability in the baseline preoperative functional status of patients in our cohort, but we believe that this is out of the scope of the current investigation and better suited to assess in a follow-up study. Also, this study used a retrospective design instead of a prospective design where PROMIS UE CAT Version 2.0 forms were administered at multiple standardized postoperative time intervals. Although this resulted in a different number of responses at each time interval, patients were still administered forms more than once (371 patients completed 1131 forms). Thus, our study still effectively evaluated the longitudinal progress of each patient throughout postoperative RCR recovery to assess milestone achievement. Regardless, it is important to acknowledge how our study did not account for patients who were discharged from the clinic at shorter postoperative time points because they were doing well functionally. Such patients did not complete PROMIS forms after their discharge from care, and this may be responsible for the lower milestone achievement rates over time for some of the PROMIS items analyzed.
A further limitation was that many items in the PROMIS UE CAT Version 2.0 question bank were not evaluated as part of the analysis, given the adaptive nature of the PROMIS UE CAT Version 2.0 interface and the resultant unequal distribution of items. Milestone achievement for these less frequently asked question items could have potentially been analyzed with a larger sample size. Additionally, included patients were English-speaking patients at a metropolitan academic center who were able to physically complete forms, resulting in potentially limited external validity due to selection from a single health care modality and the exclusion of certain physically debilitated patients. However, it was not feasible to include non–English-speaking patients and those physically unable to complete forms with respect to our study design, and the diverse nature of the included patient population in terms of ethnicity, race, age, and sex further reduced any associated selection biases. Factors that may have influenced postoperative PROMIS responses such as workers’ compensation, postoperative activity level, and compliance with physical therapy and rehabilitation were also not assessed in this study. Although we recognize the impact of these factors, we believe that they would be optimally assessed in future studies given how the primary aim of our study was to calibrate overall PROMIS milestones for the RCR cohort as a whole. Advice provided by surgeons to patients regarding physical activity may also be another variable that influences PROMIS responses that was not evaluated. However, any variability stemming from this factor is limited by how this study involved only 3 sports medicine fellowship-trained orthopaedic surgeons offering similar physical therapy and rehabilitation recommendations.
Lastly, it is important to acknowledge how PROMIS items do not necessarily specify the arm undergoing operation for questions such as “Are you able to carry a shopping bag or briefcase?” or “Are you able to pour liquid from a bottle into a glass?” Lack of clarification regarding these items may have potentially influenced patient responses. Furthermore, none of the 5 PROMIS items analyzed in this study directly related to overhead use of the arm, which is a major reason why patients choose RCR. Given both of these considerations, it is clear how the PROMIS item bank can incorporate more optimized wording and additional items in order to better evaluate functional outcomes in patients undergoing RCR.
Conclusion
The majority of patients undergoing RCR achieved functional milestones by 5 months postoperatively for the most commonly asked PROMIS UE CAT Version 2.0 items, except for being able to put on a shirt or blouse. As PROMIS utilization in orthopaedics increases, incorporation of PROMIS UE CAT Version 2.0 milestone achievement into clinical practice has potential as a new metric for assessing postoperative RCR recovery.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241231608 – Supplemental material for When Do Patients Achieve PROMIS Milestones After Rotator Cuff Repair?
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241231608 for When Do Patients Achieve PROMIS Milestones After Rotator Cuff Repair? by Nikhil R. Yedulla, Nabil Mehta, David N. Bernstein, Austin G. Cross, Kareem G. Elhage, Vasilios Moutzouros and Eric C. Makhni in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 17, 2023; accepted August 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.M. has received education payments from Medwest Associates. V.M. has received education payments from Arthrex, consulting fees from Pacira Pharmaceuticals, and hospitality payments from Smith & Nephew and Stryker. E.C.M. has received education payments from Endo Pharmaceuticals and Arthrex, consulting fees from Endo Pharmaceuticals and Smith & Nephew, nonconsulting fees from Smith & Nephew, and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Henry Ford Health System (reference No. 11361).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.