
Abstract
Background:
Anterolateral ligament reconstruction (ALLR) or lateral extra-articular tenodesis (LET) is being used more frequently in conjunction with anterior cruciate ligament reconstruction (ACLR). However, the knee flexion angle at which fixation of ALLR or LET is performed during the procedure is quite variable based on existing technique descriptions.
Purpose/Hypothesis:
The purpose of this study was to identify whether flexion angle at the time of ALLR/LET fixation affected postoperative outcomes in a clinical population. It was hypothesized that ALLR/LET fixation at low versus high flexion angles would lead to no statistically significant differences in patient-reported outcome measures and graft failure rates.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PubMed, Embase, and Cochrane Library databases were searched according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to identify published clinical studies of ACLR with ALLR/LET in which the knee flexion angle at the time of ALLR/LET was reported. A priori, low flexion was defined as 0° to 30°, and high flexion was defined as 60° to 90°. Studies were excluded if the flexion angle was between 31° and 59° because these angles constituted neither low nor high flexion angles and including them in an analysis of high versus low flexion angle at fixation would have biased the study results toward the null. The overall risk of bias was assessed using the Newcastle-Ottawa Scale. The pooled results of the studies were analyzed using the International Knee Documentation Committee (IKDC), Lysholm, and Tegner scores, along with reported graft failure rates.
Results:
A total of 32 clinical studies (5230 patients) met inclusion criteria: 22 studies (1999 patients) in the low-flexion group and 10 studies (3231 patients) in the high-flexion group. The median Newcastle-Ottawa Scale score was 6. Comparisons of patients with a low flexion angle versus a high flexion angle demonstrated no differences in the IKDC (P = .84), Lysholm (P = .67), or Tegner (P = .44) scores or in graft failure (3.4% vs 4.1%, respectively; P = .69).
Conclusion:
The results of this review indicated that ACLR performed in conjunction with ALLR/LET provides good to excellent patient-reported outcomes and low graft failure rates when ALLR/LET fixation is performed in either low or high knee flexion.
Keywords
Given the high incidence of anterior cruciate ligament (ACL) injury, there has been increasing interest in novel methods for improving outcomes after ACL reconstruction (ACLR). To this end, the anterolateral ligament (ALL) and its potential association with ACL injury has become a recent focus of investigation. The ALL has a femoral footprint adjacent to the lateral epicondyle and courses in the anteroinferior direction, with a tibial footprint between the fibular head and the Gerdy tubercle. 41 Because of a growing but somewhat controversial body of evidence suggesting that ALL tears may occur in a substantial subset of patients who sustain ACL tears, ALL reconstruction (ALLR) and a similar technique, lateral extra-articular tenodesis (LET), have been proposed as adjunctive technical measures that may protect the ACL graft after ACLR. Such techniques, for which there remains substantial variation, may use free tendon autograft or allograft or a segment of the iliotibial band left attached to the Gerdy tubercle.
Several studies have shown superior outcomes with combined ACLR and ALLR.3,42,48 In a population of high-risk patients studied by Sonnery-Cottet et al, 48 ACLR and ALLR were associated with a significant reduction in ACL graft rupture rates, compared with isolated bone–patellar tendon–bone grafts or quadrupled hamstring tendon grafts. Relative to ACLR alone, combined ACL and ALLR has also been associated with improvements in knee laxity measurements. 25 Similarly, while the first LET procedure was described by Lemaire in 1967, 51 recent studies have shown that ACLR and LET, or a modified Lemaire procedure, 30 have the ability to reduce rotational laxity, with a statistically significant reduction in pivot shift after the procedure. 24 Despite the potential benefits, to date, there have been no differences identified in International Knee Documentation Committee (IKDC) scores between patients who underwent the combined procedure and those who underwent ACLR alone.7,12,38,45
A critical technical factor without existing evidence-based consensus is what knee flexion angle should be used at the time of tensioning and fixation of the ALLR or LET. Because anterolateral structures play a role in anterolateral rotatory instability, ALLR or LET graft fixation at full extension may be favorable to restore normal knee kinematics. However, it is unclear how knee flexion angle might alter stability and/or if it may lead to overconstraint and excessive load in the lateral compartment.34,37 Several groups have investigated adding ALLR or LET to ACLR in order to address concerns about ACL graft failure and residual knee laxity.15,34 Technical descriptions of lateral extra-articular augmentation techniques differ and range anywhere from 0° to 90° of knee flexion.5,52
To address the lack of consensus in the existing literature, we conducted this systematic review and meta-analysis to identify whether flexion angle at the time of ALLR/LET fixation affected postoperative outcomes in a clinical population. We hypothesized that flexion angle during fixation would not have a significant association with postoperative patient outcomes.
Methods
A literature search was conducted by an experienced librarian in PubMed and then adapted for use in the Embase and Cochrane Library databases. This systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A combination of controlled vocabulary and keywords for the search included “IT band,”“iliotibial band,”“anterolateral ligament,” or “lateral extra-articular tenodesis” and “anterior cruciate ligament” or “anterior cruciate ligament reconstruction.” The complete search strategy is shown in Appendix Table A1. Publications were extracted starting from January 1, 2001, and ending on January 1, 2022. Two authors (D.A.K. and J.A.) used Covidence—a systematic review and meta-analysis software package—to assist with assessing for deduplication of references, abstract screening, and full-text screening (Covidence systematic review software, Veritas Health Innovation). All articles were manually screened.
Eligibility Criteria
The inclusion criteria were as follows: (1) clinical study, (2) study participants underwent ACLR, and (3) study participants underwent ALLR or LET (Figure 1). Exclusion criteria consisted of studies with <5 study participants, systematic reviews and meta-analyses, trial protocols, surgical technique papers, failure to report knee flexion angle at the time of ALLR/LET fixation, or intermediate (31°-59°) knee flexion angles at the time of fixation. Intermediate flexion angles at fixation were excluded because they constituted neither low nor high flexion angles. Including them in an analysis of high versus low flexion angle at fixation would have biased the results of the study toward the null and increased the risk of type 2 error.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study selection flow diagram. ALLR, anterolateral ligament reconstruction; LET, lateral extra-articular tenodesis.
Risk of Bias
Risk of bias was assessed using the Newcastle-Ottawa Scale, which consists of 8 items categorized into 3 domains (selection, comparability, and outcome). Studies are rated from 0 to 9, with scores of 0 to 2 indicating poor quality, 3 to 5 indicating fair quality, and 6 to 9 indicating good/high quality.
Study Groups
Flexion angles at the time of ALLR/LET fixation were extracted individually for each article. Articles that reported >1 flexion value at the time of ALLR/LET fixation were reported as the mean of the reported range. The comparison groups of interest were ALLR/LET fixation at low flexion, defined as 0° to 30°, and ALLR/LET fixation at high flexion, defined as 60° to 90°.
Patient Characteristics and Outcomes
Demographic measures of interest included group size, follow-up time, sex, age, and body mass index (BMI). Five main outcomes of interest were identified: (1) postoperative IKDC score, (2) postoperative Lysholm score, (3) postoperative Tegner score, (4) graft failure, and (5) subsequent meniscal procedures. Analyses of subsets of the results of Getgood et al16,17 from the STABILITY Study were excluded from pooled analyses in order to avoid double-counting participants in summary analyses.
Statistical Analysis
Demographic variables of interest (follow-up time, age, sex, and BMI) were assessed using frequencies and percentages for categorical variables and medians and ranges for continuous variables. In order to assess for demographic similarities at baseline, baseline characteristics were also assessed stratified by low and high flexion angle. Pooled means for continuous outcomes (IKDC, Lysholm, and Tegner scores) were calculated using weighted means with a random-effects model, using a restricted maximum-likelihood estimator. Weighted means were also calculated for secondary outcomes, including the Knee injury and Osteoarthritis Outcome Score (KOOS) subscales (Pain, Symptoms, Activities of Daily Living [ADL], Recreation, and Quality of Life [QOL]). Chi-square tests and t tests of weighted values were used to compare results between the low-flexion and high-flexion groups. Pooled failure rates at each measured degree of flexion were also calculated. Subgroup analyses were also conducted in the same manner by assessing ALLR and LET procedures separately. The cutoff for statistical significance was P < .05. All analyses were performed with the use of R software Version 4.0 (R Foundation for Statistical Computing).
Results
A total of 32 clinical studies † (5230 knees) were included in this systematic review and meta-analysis (Appendix Table A2). There were 22 studies ‡ (1999 patients) in the low-flexion group and 10 studies5,13,16-19,26,29,32,44 (3231 patients) in the high-flexion group. Of the 32 studies, 24 (75.0%) studies reported the proportion of patients who were male (1490/2236; 66.6%). The median follow-up time was 35.4 months (range, 12.3-232.8 months), and the median age was 24.7 years (range, 13.0-33.1 years). Of the 11 (34.4%) studies reporting mean BMI values, the median BMI was 24.0 kg/m2 (range, 22.0-25.4 kg/m2). Patients in the low- and high-flexion groups were similar across a range of demographic variables (Table 1), although there were significantly more male patients in the low-flexion studies (P < .001).
Characteristics of the Low- and High-Flexion Studies a
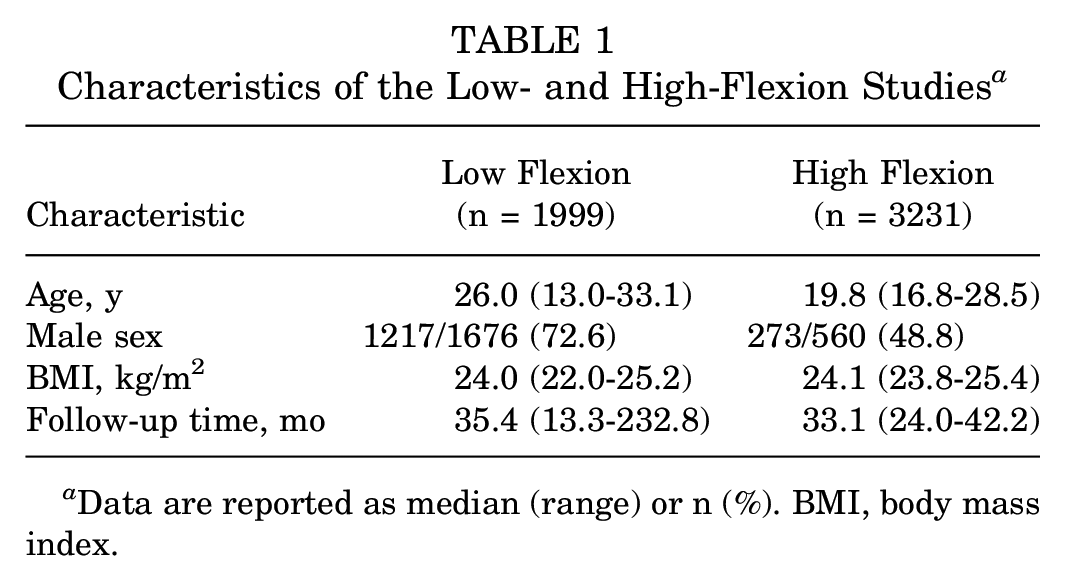
Data are reported as median (range) or n (%). BMI, body mass index.
The median Newcastle-Ottawa Scale score for the included studies was 6 (range, 3-9), indicating good quality. The most common reasons for lost points were inadequate control for covariables and insufficiently detailed loss to follow-up.
Main Outcomes
Pooled measures using random effects were calculated for both the low-flexion and high-flexion groups (Figure 2). For the postoperative IKDC score, the mean pooled estimate was 86.46 (95% CI, 81.86-91.05) for the low-flexion group and 87.18 (95% CI, 85.86-88.50) for the high-flexion group (P = .84). The mean postoperative Lysholm score was 90.37 (95% CI, 85.71-95.04) for low-flexion studies and 93.89 (95% CI, 86.83-100.94) for high-flexion studies (P = .67). There was no evidence that the postoperative Tegner score varied by flexion angle (P = .44), with mean scores being 6.65 (95% CI, 5.86-7.44) for low flexion and 7.70 (95% CI, 4.76-10.64) for high flexion.

Forest plots demonstrating the International Knee Documentation Committee (IKDC) scores for (A) low-flexion and (B) high-flexion studies, the Lysholm scores for (C) low-flexion and (D) high-flexion studies, and the Tegner scores for (E) low-flexion and (F) high-flexion studies. RE, random effects.
Among patients who underwent ALLR/LET fixation at low flexion, 27 of 791 (3.4%) experienced graft failure, as opposed to 13 of 315 (4.1%) who experienced graft failure in the high-flexion group (P = .69) (Table 2). Further exploring these differences, failure rates at 0°, 30°, 65°, and 90° were 2.7% (20/735), 12.5% (7/56), 3.8% (11/291), and 8.3% (2/24), respectively. Subsequent meniscal procedures were performed in 66 of 1077 (6.1%) patients in the low-flexion group. The frequency of subsequent meniscal procedures was not reported in any of the studies included in the high-flexion group and was therefore not included in the comparative analysis.
Graft Failures According to Definitions a

Dash indicates graft failure/rupture was not specified. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
This study included patients with acute and chronic injuries.
Additional Outcomes
Postoperative KOOS subscale scores were reported in 4 studies.17,32,46,47 Across both low-flexion and high-flexion studies, the weighted means of the Pain, Symptoms, and ADL subscores were 93.58 (95% CI, 89.73-97.42), 89.17 (95% CI, 84.08-94.25), and 96.92 (95% CI, 94.61-99.23), respectively. The mean for KOOS-Recreation was 85.58 (95% CI, 80.91-90.25), and that for KOOS-QOL was 80.87 (95% CI, 71.33-90.40).
Subanalysis of ALLR Versus LET
In this subanalysis, there were 15 studies § (2551 knees) in the ALLR group and 17 studies ‖ (2246 knees) in the LET group (total of 4797 knees). The study characteristics between the knees that underwent ALLR versus LET are shown in Table 3. There were no significant differences between the ALLR and LET groups.
Study Characteristics According to ALLR and LET Groups a
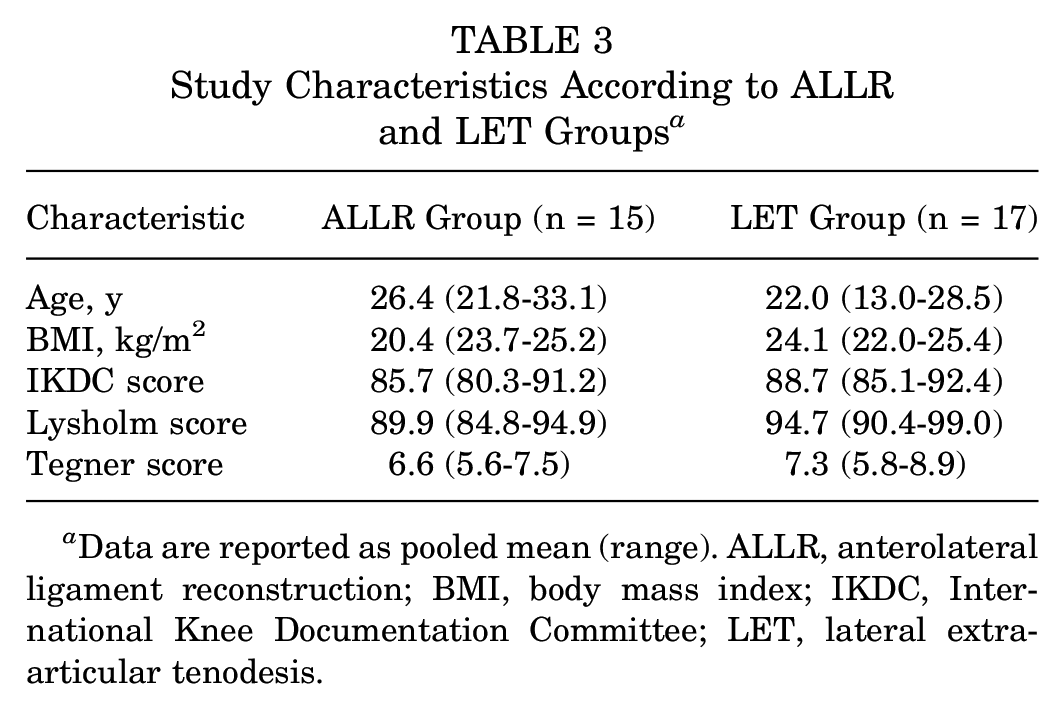
Data are reported as pooled mean (range). ALLR, anterolateral ligament reconstruction; BMI, body mass index; IKDC, International Knee Documentation Committee; LET, lateral extra-articular tenodesis.
Discussion
In this systematic review and meta-analysis, we investigated outcomes in patients who underwent ALLR/LET fixation at low (0°-30°) and high (60°-90°) flexion angles. The most important finding from this study was that differences between postoperative patient-reported outcome measures—the IKDC, Lysholm, and Tegner scores—were not statistically significant between patients who underwent ALLR/LET at low or high flexion fixation. The analysis also demonstrated that patients who underwent ALLR/LET fixation at a low flexion angle had a similar rate of graft failure to patients who underwent ALLR/LET fixation at a high flexion angle. These results suggest that ALLR/LET fixation may be effectively performed at both low and high flexion angles with good to excellent patient-reported outcome scores and low graft failure rates, without significant differences between cohorts.
Several studies have investigated the effects of flexion angle at the time of fixation in cadaveric specimens.15,36 Anatomically, the distal footprint is slightly different between the ALLR and LET techniques. ALLR is performed by identifying the tibial insertion of the ALL, located between the Gerdy tubercle and the anterior margin of the fibular head, approximately 1 cm distal to the joint line. 11 The native ALL has an ultimate tension of 32.78 MPa and an ultimate load to failure of 49.90 N, giving it the lowest load to failure in comparison with other ligaments of the knee, including ACL, posterior cruciate ligament, medial collateral ligament, and lateral collateral ligament (LCL). 54 For LET, the Gerdy tubercle is similarly identified, and an approximately 10 × 1 cm–wide band of the iliotibial band is harvested proximally and left attached to the Gerdy tubercle distally. Proximally, care is taken not to damage deeper structures such as the LCL. 2 After the free end of the graft is prepared, the iliotibial band strand is passed from distal to proximal, ensuring that the graft is passed under the LCL. Schon et al 43 found no kinematic differences at any tested ALLR fixation angle, including 0°, 15°, 30°, 45°, 60°, 75°, and 90°. However, all fixation angles led to overconstraint of the knee relative to normal joint kinematics, measured by anterior drawer, pivot-shift, and internal rotation tests. In contrast, Inderhaug et al 27 found that combined ACL and ALLR led to restoration of intact knee kinematics when graft fixation was performed in full extension. However, when the graft was fixed at 30° or 60°, there was a significant amount of internal rotation laxity. Interestingly, in the current study, clinical outcomes were similar for patients who underwent ALLR/LET fixation at either low or high flexion angles. The 12.5% failure rate identified at 30° of flexion is likely due to outlier data, which can skew results in smaller cohorts.
The flexion angle at the time of ACLR graft fixation has been shown to be an important factor for the loads sustained by ACLR grafts. 6 One study of double-bundle ACLR found that the posterolateral graft was overloaded when both bundles were fixed at 30°. 33 When the anteromedial bundle was fixed at 60° and the posterolateral bundle was fixed at 0°, the anteromedial graft was overloaded. Debandi et al 14 separately showed that anatomic ACLR at 30° of flexion restored rotational knee stability relative to grafts fixed at full extension.
Clinical studies investigating flexion angles at the time of ACL graft fixation have not shown differences in results between low flexion angles and high flexion angles at the time of fixation. Abdel Khalik et al, 1 in a systematic review, investigated the association of knee flexion angle—including low (<30°) and high (30°) angles—with outcomes in patients who underwent single-bundle quadriceps tendon autograft ACLR. The authors found comparable outcomes across all groups, suggesting there was not one ideal flexion angle for fixation. Therefore, even if the ACL graft fixation angles are different from the ALLR/LET fixation angles, ACL graft fixation angles should not have an effect on patient outcomes. To our knowledge, our study is the first systematic review and meta-analysis to specifically investigate the knee flexion angle at the time of ALLR/LET fixation in a large, pooled clinical population.
Limitations
There were several limitations to this study. First, the effect of flexion angle on subsequent outcomes would be best studied using a randomized controlled experimental design, which would randomize patients to ALLR/LET fixation at low versus high flexion. A randomized type of study design would minimize confounding by controlling for both observed and unobserved confounders. The present study was a systematic review of the existing literature (32 studies), with an evidence level of 4. Second, our review may have been underpowered to detect differences between outcomes of interest, including IKDC, Lysholm, and Tegner scores. It is important to note, however, that while statistical differences were not detected, small differences between patient-reported outcome measures are likely not clinically meaningful. Third, the definition of graft failure differed in our review based on the varied definitions in each included study. Importantly, Getgood et al 17 included an additional metric for failure—defined as “clinical failure”—that included mild asymmetric pivot-shift tests. The senior authors (P.D.F., B.E.H.) determined that clinical failure as described in that study was too liberal, including minor discrepancies in patient outcomes as “failures.” Thus, graft rupture was used to indicate graft failure when extracting data from the Getgood et al studies.16,17 Fourth, ALLR and LET were grouped together for the main analysis of this study. To avoid grouping the 2 different procedures, we also assessed both supplementary procedures individually in subanalyses. Fifth, this study was unable to control, to a significant degree, for confounding. Future randomized controlled trials could help definitively address if confounding plays a role. Sixth, there was a substantial amount of missing data regarding follow-up time among studies in this area. Additionally, rotation at the time of ALLR/LET was often not mentioned in the included studies. Therefore, we were unable to assess the association of rotation with patient-reported outcomes. Importantly, controversy exists regarding the precise function of the ALL and the extent to which it confers rotational stability to the knee. Finally, while ALLR/LET procedures are designed to enhance stability in the ACL-reconstructed knee, it is unclear if any particular flexion angle overconstrains the knee and if this would manifest as lateral compartment osteoarthritis with longer-term follow-up.
Conclusion
ACLR performed in conjunction with ALLR/LET was found to provide good to excellent patient-reported outcome scores and low graft failure rates when ALLR/LET fixation occurs in either low knee flexion or high knee flexion.
Footnotes
Appendix
Included ALLR/LET Fixation Studies (n = 32) a

| Lead Author (Year) | Flexion Angle at ALLR/LET Fixation, deg | No. of Patients | Mean or Median Follow-up Time, mo | Outcomes (mean or proportion) |
|---|---|---|---|---|
| Wilson (2019) 52 | 0 | 57 | 38.5 | Graft failure (3/57) |
| Nishida (2022) 35 | 10 | 9 | — | — |
| Getgood (2020) 17 | 65 | 306 | 24 | IKDC (87.3) |
| Helito (2019) 22 | 0 | 30 | 28.1 | IKDC (86.9), Lysholm (88.3) |
| Helito (2018) 21 | 0 | 33 | 25 | IKDC (92.7), Lysholm (95.4) |
| Sheean (2020) 44 | 60 | 10 | — | — |
| Alessio-Mazzola (2019) 5 | 90 | 24 | 42.2 | IKDC (88.4), Lysholm (97.4), Tegner (9.2), graft failure (2/24) |
| Yoon (2021) 53 | 30 | 19 | — | IKDC (57.8), Lysholm (58.7), Tegner (4), graft failure (2/18) |
| Grassi (2021) 19 | 70 | 2559 | — | — |
| Imbert (2017) 26 | 90 | — | — | — |
| Colombet (2011) 13 | 90 | 20 | — | — |
| Meynard (2020) 32 | 90 | 50 | — | IKDC (85.5), Lysholm (90.2), Tegner (6.2) |
| Sonnery-Cottet (2015) 49 | 0 | 92 | 32.4 | IKDC (86.7), Lysholm (92), Tegner (7.1) |
| Ibrahim (2017) 25 | 30 | 53 | — | Lysholm (98), Tegner (8) |
| Getgood (2020) 16 | 65 | 176 | — | Graft failure (3/23) |
| Branch (2015) 8 | 30 | 6 | — | — |
| Castoldi (2020) 9 | 30 | 60 | 232.8 | IKDC (82.4), Lysholm (90.3), graft failure (5/38), meniscal procedure (11/38) |
| Helito (2021) 23 | ||||
| Acute | 0 | 34 | 28.7 | IKDC (88.1), Lysholm (89.3), graft failure (1/34) |
| Chronic | 0 | 96 | 29.4 | IKDC (87.3), Lysholm (91.1), graft failure (2/96) |
| Thaunat (2017) 50 | 0 | 603 | 35.5 | Graft failure (14/548), meniscal procedure (30/548) |
| Sonnery-Cottet (2020) 47 | 0 | 112 | 12.3 | IKDC (86.8), Lysholm (92), Tegner (6), meniscal procedure (1/112) |
| Rowan (2019) 40 | 30 | 55 | 27 | Lysholm (98), Tegner (8.04) |
| Rosenstiel (2019) 39 | 0 | 72 | 46.8 | IKDC (90.5), Lysholm (94.4), Tegner (8.8), meniscal procedure (4/72) |
| Sonnery-Cottet (2017) 48 | 0 | 221 | 35.4 | IKDC (81.8), Lysholm (91.9), Tegner (7), meniscal procedure (11/221) |
| Ahn (2021) 4 | 30 | 47 | 47.9 | IKDC (93.3) |
| Gibbs (2022) 18 | 60 | 10 | — | — |
| Lee (2019) 31 | 30 | 42 | 38.2 | IKDC (84.3), Lysholm (90.2), Tegner (7) |
| Hamido (2021) 20 | 7.5 | 53 | 60 | Lysholm (96), Tegner (7.9) |
| Cavaignac (2020) 10 | 0 | 31 | — | IKDC (86.8), Lysholm (96.2), Tegner (5.9) |
| Zhang (2016) 55 | 30 | 20 | — | IKDC (96.2), Lysholm (96.3), Tegner (6.3) |
| Kocher (2006) 29 | 90 | 44 | — | — |
| Jørgensen (2001) 28 | 30 | 169 | — | Lysholm (99), Tegner (7) |
| Sonnery-Cottet (2021) 46 | 0 | 86 | 104.33 | IKDC (89.7), Lysholm (93.9), Tegner (6.1), meniscal procedure (9/86) |
Dashes indicate data not reported. ALLR, anterolateral ligament reconstruction; IKDC, International Knee Documentation Committee; LET, lateral extra-articular tenodesis.
Final revision submitted August 1, 2023; accepted August 17, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.D.F. has received consulting fees from WishBone Medical and stock options from Osso. B.E.H. has received financial or material support from AlloSource, Springer, and Vericel; education payments from Arthrex; nonconsulting fees from Arthrex; royalties from Springer; and stock options from Imagen Technologies. Y.M.Y. has received consulting fees from Smith & Nephew. D.E.K. has received financial or material support from Arthrex and consulting fees from Johnson & Johnson and Miach. M.S.K. has received financial or material support from Elsevier and Wolters Kluwer Health; consulting fees from Best Doctors, OrthoPediatrics, Ossur, and Smith & Nephew; and royalties from OrthoPediatrics, Ossur, Elsevier, and Wolters Kluwer Health. A.T.P. has received consulting fees from OrthoPediatrics. J.J.N. has received research support from Smith & Nephew and Zimmer Biomet Holdings, consulting fees from Responsive Arthroscopy and Smith & Nephew, nonconsulting fees from Smith & Nephew, and royalties from Responsive Arthroscopy. S.C.W. has received consulting fees from Smith & Nephew. P.L.W. has received research support from AlloSource and Ossur, financial or material support from Elsevier, and royalties from Elsevier. M.M. has received royalties from Elizur. J.E.V. has received consulting fees from Arthrex. D.D.S. has received financial or material support from Elsevier, research support from OrthoPediatrics, and royalties from Elsevier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Authors
David A. Kolin, MD (Hospital for Special Surgery, New York, New York, USA); John Apostolakos, MD (Hospital for Special Surgery, New York, New York, USA); Peter D. Fabricant, MD, MPH (Hospital for Special Surgery, New York, New York, USA); Bridget Jivanelli, MLIS, AHIP (Hospital for Special Surgery, New York, New York, USA); SATURN Study Group (Yi-Meng Yen, MD, PhD, FAAOS [Boston Children’s Hospital, Boston, Massachusetts, USA]; Dennis E. Kramer, MD, FAAOS [Boston Children’s Hospital, Boston, Massachusetts, USA]; Mininder S. Kocher, MD, MPH, FAAOS [Boston Children’s Hospital, Boston, Massachusetts, USA]; Andrew Tennant Pennock, MD, FAAOS [Rady Children’s Hospital, San Diego, California, USA]; Jeffrey J. Nepple, MD, FAAOS [Washington University Medical Center, St Louis, Missouri, USA]; Samuel Clifton Willimon, MD, FAAOS [Children’s Healthcare of Atlanta, Atlanta, Georgia, USA]; Crystal Ann Perkins, MD, FAAOS [Children’s Healthcare of Atlanta, Atlanta, Georgia, USA]; Henry Bone Ellis Jr, MD, FAAOS [Scottish Rite for Children, Dallas, Texas, USA]; Philip L. Wilson, MD, FAAOS [Scottish Rite for Children, Dallas, Texas, USA]; Michael McClincy, MD [University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA]; James Everett Voos, MD, FAAOS [University Hospital Cleveland Medical Center, Cleveland, Ohio, USA]; David D. Spence, MD, FAAOS [Campbell Clinic Orthopaedics, Memphis, Tennessee, USA]); and Benton E. Heyworth, MD (Boston Children’s Hospital, Boston, Massachusetts, USA).