
Abstract
Background:
With advancements in the technology, techniques, and biomechanical understanding of shoulder arthroplasty, higher rates of postoperative return to various sports have been seen in the past decade.
Purpose:
To observe the return-to-golf rate after various types of shoulder arthroplasty (anatomic total shoulder arthroplasty [TSA], hemiarthroplasty [HA], and reverse total shoulder arthroplasty [RSA]) and also to review the protocols for return to golf.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed in a search of PubMed, JSTOR, Google Scholar, ScienceDirect, and CORE using the keywords “return to sport,”“shoulder arthroplasty,”“golf,”“TSA,”“shoulder arthroplasty,”“hemiarthroplasty,”“reverse shoulder arthroplasty,”“RSA,”“sports,” and “athlete.” Of 145 preliminary results, 10 retrospective studies (n = 178 patients) published between 1998 and 2021 were included in the final analysis.
Results:
The mean patient age was 65 years. Of the 172 patients with reported return-to-sport rates, the mean return-to-golf rate was 75.8% for all types of shoulder arthroplasty. Of these 172 patients, 107 patients were categorized by type of procedure: Anatomic TSA had the highest return-to-golf rate at 77.6% (49/107), followed by HA at 64.3% (14/107) and RSA at 59.1% (44/107). Four studies commented on return to the full 18 holes of golf, with a return-to-sport timeline ranging from 5 to 6 months postoperatively. One study specified the return-to-golf timeline based on the type of shot and reported the mean number of weeks before putting, chipping, and returning to the course as 20, 22, and 27 weeks, respectively. Two studies that reported on golf playing frequency noted an increase from before to 1 year after TSA, from a mean of 1.6 and 0.7 times per week to 2.0 and 1.7 times per week, respectively. Only 1 study, published in 1998, provided a comprehensive return-to-golf protocol.
Conclusion:
The return-to-golf rate after shoulder arthroplasty was highest after anatomic TSA (78%) compared with HA (64%) and RSA (59%). The most commonly reported duration before returning to a full 18 holes was 5 to 6 months, but patients returned to putting and chipping earlier.
The incidence of shoulder arthroplasty in the United States has increased dramatically in the last decade and is predicted to continue to increase. 20 A combination of expanding indications for reverse shoulder arthroplasty, aging of the American population, and historically successful clinical outcomes with shoulder arthroplasty have resulted in a greater number of patients undergoing arthroplasty.10,15 Among the recreational activities to which patients hope to return after surgery, golf is common and can be demanding for the upper extremity.
Anecdotally, active patients are often the most inquisitive about goals and expectations after their surgery and appreciate detail in their counseling. Studies have found that 64% of patients chose to undergo arthroplasty in order to return to sport 11 and approximately 70% of patients participated in recreational sports within 4 years of shoulder arthroplasty. 18
The primary purpose of this study was to systematically review the literature for rates of return to golf after anatomic total shoulder arthroplasty (TSA), hemiarthroplasty (HA), and reverse shoulder arthroplasty (RSA). The secondary purposes included other topics relevant to golfers undergoing shoulder arthroplasty, as follows:
To provide evidence-based responses to common questions asked by golfers, including return-to-play protocols, discomfort with sport, changes in performance, and restrictions
To review the current literature for evidence that guides surgical decision-making on surgical technique and postoperative restrictions
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed in the conduct of this systematic review and meta-analysis. A search was completed in PubMed, MEDLINE, Scopus, EMBASE, and the Cochrane Library using the keywords “return to sport,”“shoulder arthroplasty,”“golf,”“TSA,”“shoulder arthroplasty,”“hemiarthroplasty,”“reverse shoulder arthroplasty,”“RSA,”“sports,” and “athlete” in different combinations. The quality of the included studies was evaluated according to the Methodological Index for Non-Randomized Studies checklist. Any study with English, German, or French as the primary language was included in the analysis. Review studies were omitted from the analysis. The preliminary search yielded 145 results. Of these, 135 were excluded due to lack of relevance or not having golf-specific statistics linked with athlete return to sport. Some of these studies are reviewed in the discussion section of this article; however, they were not included in the primary analysis. Ten studies, which included retrospective studies, cohort studies, and case series, were included in the final analysis (Figure 1). The texts of these papers were reviewed to answer questions pertinent to our secondary purposes.
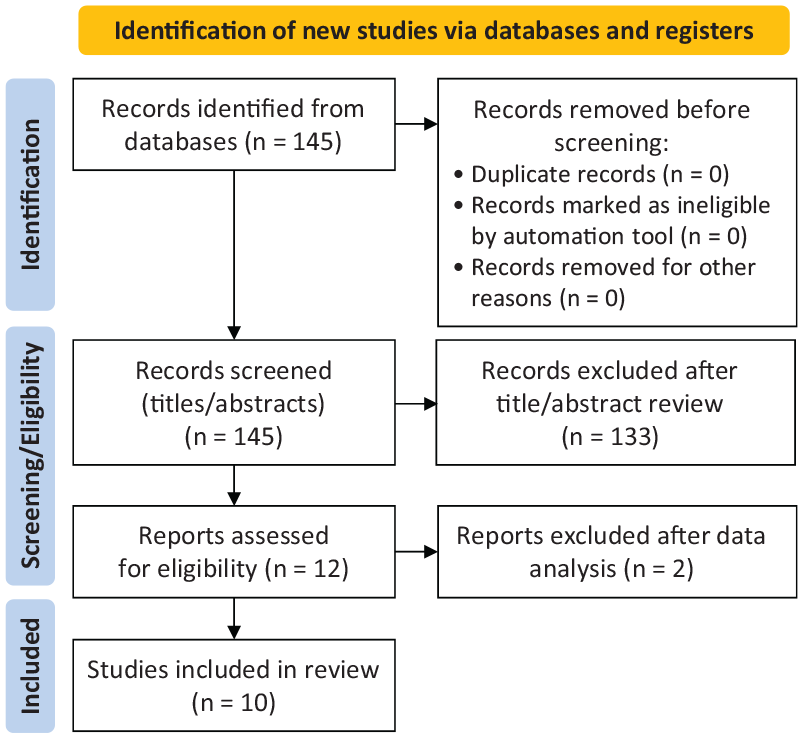
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart outlining the study exclusion and inclusion process. NA, not applicable.
Results
Return to Golf
Ten studies1,3-6,9,11,16,18,19 met the study inclusion criteria; all were either level 3 or 4 evidence (Table 1). The years of publication ranged from 1998 to 2021. The majority of studies included returning to any sport rather than just golf. Of a total of 773 patients with return-to-sport data, there were 172 golfers, and for 107 of these, the type of arthroplasty (HA, TSA, or RSA) was specified. The mean age for all golfers was 65 years (range, 49-75 years). All RSA data included were from 2015 and later.
Return-to-Sport Results from Meta-analysis a
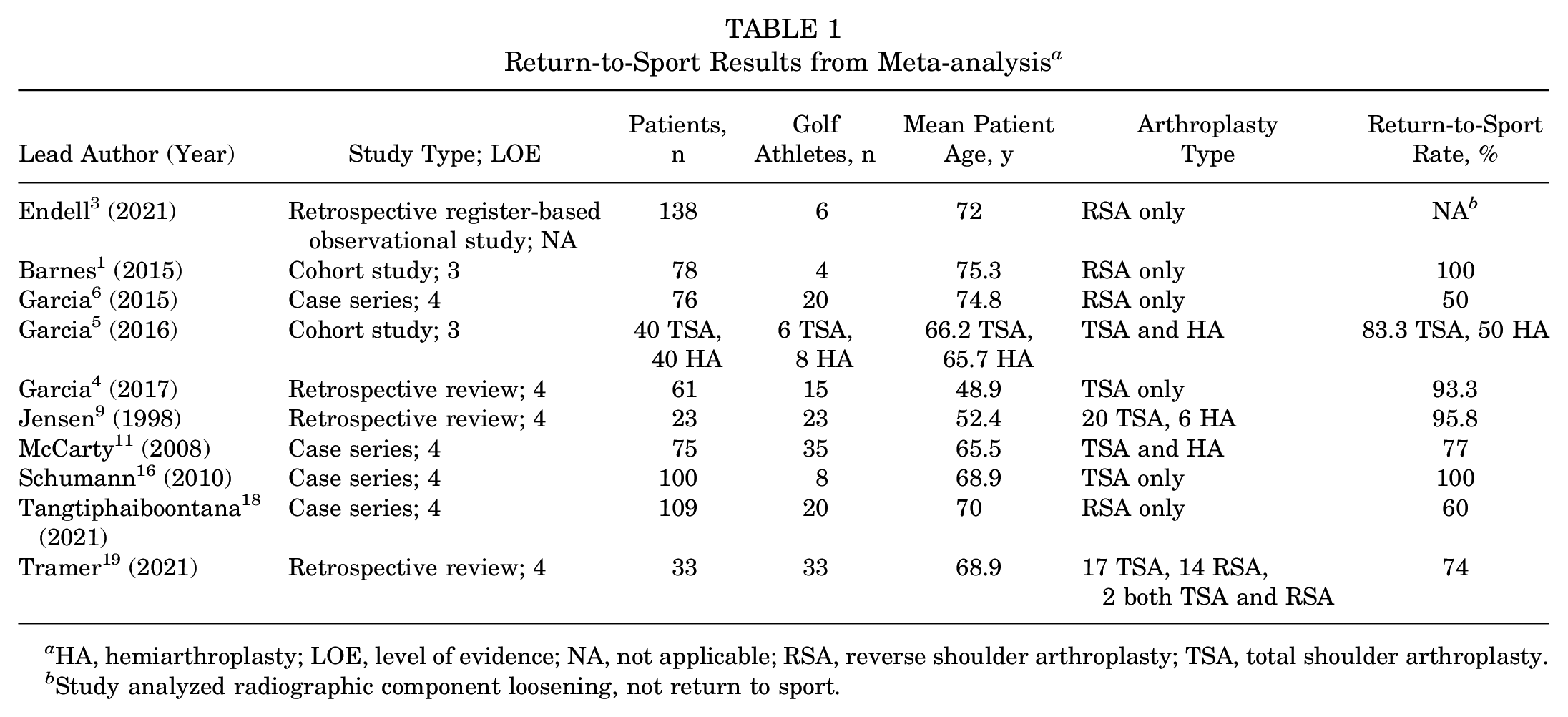
HA, hemiarthroplasty; LOE, level of evidence; NA, not applicable; RSA, reverse shoulder arthroplasty; TSA, total shoulder arthroplasty.
Study analyzed radiographic component loosening, not return to sport.
Of the 172 patients, the mean return-to-golf rate was 76% for all types of shoulder arthroplasty. The return-to-sport rate was highest for TSA (78%), followed by HA (64%) and RSA (59%) (Table 2). Garcia et al 5 specifically compared return to sport after 40 TSA and 40 HA procedures for primary osteoarthritis. Those authors found that 97% of TSA patients returned to sport compared with 66% of HA patients; 5 of 6 TSA patients were able to return to golf compared with 4 of 8 HA patients. In addition, 45% of HA patients felt hindered during sport compared with 13% of TSA patients. 5
Return to Sport by Arthroplasty Type

Four studies that reported timelines for return to the full 18 holes of golf found mean times of 4.5 months (TSA and HA), 9 5 months (TSA and HA), 11 5 months (RSA), 5 and 5 months (TSA). 16 Two studies9,11 reported frequency of golf before and after shoulder arthroplasty; Jensen and Rockwood 9 and McCarty et al 11 both reported an increase in the frequency of golf from before to 1 year after TSA, from a mean of 1.6 and 0.7 times per week to 2.0 and 1.7 times per week, respectively.
Postoperative Protocol for Returning to Golf
Only 1 study specified a return-to-golf protocol: Jensen and Rockwood 9 allowed TSA and HA patients to return to putting at 2 weeks, short chips at 4 to 6 weeks, medium irons at 6 to 8 weeks, long irons at 2 months, and then gradual progression toward full swings with a driver. Patients were also told to tee up all shots for 1 year after surgery.
Multiple studies on RSA reported postoperative protocols not specific to golf.3,4,18 All of these studies limited external rotation in the first month after surgery, and the timeline for return to sport or unrestricted motion varied from 3 weeks to 4 months. Tangtiphaiboontana et al 18 allowed full activity at 4 months but recommended avoiding activities involving forceful impact.
Risk Factors for Not Returning to Golf
In the studies reviewed, age >70 years was identified as a negative prognosticator for return to sport after RSA6,18 and TSA, 16 and return to sport in patients younger than 55 years undergoing TSA was reported as high as 93%. 4 The indication for RSA being osteoarthritis or rheumatoid arthritis has been reported to have higher return-to-sport rates than cuff tear arthropathy and fracture (100% vs 76%-81%). 6 Hand dominance did not affect the return-to-sport rate for HA or TSA in 2 studies5,11 and for RSA in 1 study, 6 but Tangtiphaiboontana et al 18 reported that the laterality of RSA affected return to sport, with a 38% return-to-sport rate after right-sided RSA compared with 71% after left-sided RSA, although the hand dominance of the patients was not specified. Bilateral RSA was reported to have similar return-to-sport rates as unilateral RSA (69% vs 76%, respectively). 18
Will Golf Be Painful After Surgery?
Three studies9,11,16 reported details about pain during or after rounds of golf after arthroplasty. Jensen and Rockwood 9 reported that 23 of 26 patients reported no pain while playing golf postoperatively; however, 3 patients continued to experience mild pain during golf rounds. McCarty et al 11 reported that 39% of patients took some type of pain medication in order to return to sport. In a group of 8 golfers, Schuman et al 16 found that half had no pain and the other half had slight pain after a round.
Will Arthroplasty Affect Performance?
Multiple studies reported on aspects of golf performance, including handicap and driving distance.9,11,19 Overall, the studies suggested that handicap can be expected to stay the same or improve. Driving distance seems to decrease by 10 to 20 yards (9-18 m) after RSA and increase by approximately 10 yards (9-18 m) after TSA, although there is some variability among studies in reports after TSA.
Two studies asked patients about their handicap before and after arthroplasty, and both studies found an improvement after arthroplasty.9,11 Jensen and Rockwood 9 reported a +4 mean change in handicap across all patients. McCarty et al 11 found that in a group of 48 patients who underwent TSA in order to return to sports, 71% reported an improvement in their ranking or handicap. It is important to note that handicap is calculated based on the past 20 rounds of golf, and 1-year follow-up is likely premature to see real changes in handicap. Studies that feature a 2-year follow-up of patients would provide a much more accurate reflection of the treatment effect.
Driving distance was reported to increase by a mean of 12 yards after TSA in 2 studies.9,14 One study reported driving distance after RSA and showed a mean postoperative decrease in driving distance of 20 yards (18 m). 19
Does Playing Golf Increase the Risk of Radiographic Lucencies, Complications, or Revisions?
All studies except one (Endell et al 3 ) had a minimum 2-year follow-up and included a retrospective chart review component for complications or revisions. Jensen and Rockwood 9 included a matched cohort of patients who did not perform athletic activity. The authors found no increase in complications or revision rates in 23 golfers who underwent HA or TSA compared with 76 nongolfers. Two studies3,9 included a radiographic review. Jensen and Rockwood 9 found no increased rate of progressive radiolucency around the humeral or glenoid component in a group of 20 golfers compared with 76 nongolfers. Endell et al 3 compared radiographic findings after RSA in 49 patients who participated in upper extremity sports versus 68 patients who did not; the rate of radiolucency around the humeral component was higher in the nonsports group (32% vs 12%). No differences were found in the rate of glenoid radiolucencies, scapular notching, bone resorption, or heterotopic bone formation; in addition, the investigators found no revisions for component loosening in the upper extremity sports group and no differences in all-cause revisions. Schuman et al 16 did not perform a radiographic analysis for the purpose of their study but commented that there were no symptomatic radiolucent lines that led to revision during the study period in a group of 55 HA and TSA procedures.
In the remainder of studies reporting revisions and complications, only Garcia et al 5 and Jensen and Rockwood 9 reported revisions during the follow-up period. At a mean 5 years of follow-up after HA and TSA in an athletic population, 2 of 40 TSA patients (5%) underwent revision for recurrent dislocations and painful stiffness; neither had glenoid loosening. Further, 4 of the 40 HA patients required revision: 3 were for glenoid arthritis and 1 for recurrent dislocations. 5 Last, Jensen and Rockwood 9 polled 50 surgeons on their subjective perception of whether increased complications occur in patients who participate in golf after arthroplasty; 91% believed that there was no increase in complications.
Discussion
This systematic review and meta-analysis identified return-to-golf rates to be 64%, 78% and 59% after HA, TSA, and RSA, respectively, and 76% overall. RSA had the lowest rate of return to golf, and for the diagnosis of primary osteoarthritis, TSA resulted in higher rates of return to golf than HA.
The most commonly reported duration before returning to the full 18 holes was 5 to 6 months, but patients have returned to putting and chipping earlier. Dukan et al 2 found that the mean number of weeks before putting, chipping, and returning to the course was 20, 22, and 27 weeks, respectively. Although most surgeons will not place restrictions on golf frequency or intensity after arthroplasty, the studies analyzed suggest that a sizable minority of surgeons have recommended limiting play to <2 rounds per week and avoiding shots with high impact. In the survey of 50 surgeons conducted by Jensen and Rockwood, 9 40% recommended a limit on the number of rounds per week, 27% recommended swing modifications (but did not specify what should be modified), and 46% gave special instructions (eg, tee up all shots for 1 year to avoid divots). Golant et al 8 surveyed 94 surgeons in 2012 on whether they allow patients to return to golf or other noncontact sports without limitation. Those authors found that for TSA, RSA, and HA, 28%, 35%, and 15% of surgeons, respectively, allowed return to golf with limitations; the limitations were not specified. The reason for the placement of these restrictions is unknown but may be a case-by-case decision made by the surgeon depending on patient risk factors that would predispose that patient to having an unsuccessful postoperative clinical or functional outcome.
Age >70 years and the indications for cuff tear arthropathy or fracture (compared with primary osteoarthritis or rheumatoid arthritis) have been negative predictors of returning to golf,4,6,16,18 although many patients have non–shoulder related reasons for not returning to golf. Bilateral RSA and dominant-extremity TSA or HA do not appear to influence return to golf,5,6,11 but dominant extremity RSA has been reported to reduce rates of return to sport. 18 Based on the 3 studies included in the analysis that assessed pain,9,11,16 although patients can expect an overall improvement in pain after arthroplasty, some patients may continue to experience mild pain while playing golf. Examining a group of 61 arthroplasty procedures of all types, Dukan et al 2 found that the mean visual analog scale pain score during golf decreased from 6.3 to 1.3. In a group of 26 TSA and HA procedures, 3 patients reported mild pain after a round, but the remaining were able to return pain free. Simovitch et al 17 and Godin et al 7 studied general return to sport and found slight difficulty or pain playing any sport after RSA in 38% and 13% of patients, respectively.
Golf handicaps can be expected to stay the same or slightly improve, based on studies by Jensen and Rockwood 9 and Papaliodis et al, 14 who reported a +4 and +1.4 change in handicap after TSA, respectively. Dukan et al 2 asked patients to report the change in their handicap from before surgery to 1 year after TSA and RSA; there was no change in handicap in both groups. Driving distance has been reported to increase by approximately 10 yards after TSA and decrease by 10 to 20 yards after RSA.2,9 However, these studies were underpowered and cannot be used to answer patient performance–related questions. A prospective return-to-golf study that evaluates patient pain as well as performance as an endpoint would be useful in updating patient rehabilitation protocols and setting realistic patient expectations.
An area of continued interest among researching physicians and patients alike is whether any technical- or implant-related decisions affect return to golf. Despite theoretical concerns about early mechanical failures, no study has reported increased rate of failure or concerning radiographic findings in athletes compared with nonathletic patients. Godin et al 7 reported a higher return-to-sport rate in patients with a repaired subscapularis; the criteria for repair were tissue quality amenable to repair and lack of high-grade fatty infiltration. Those investigators also reported no difference in return to sport based on glenosphere size after hypothesizing a negative correlation between sphere size and return to sport. No study has compared RSA implant design features such as lateralized or medialized center of rotation glenospheres; however, rates of return between lateralized 18 and medialized 7 glenospheres have been similar.
Although the thrower’s shoulder has been studied extensively and is commonly discussed in the shoulder community, less attention is given to the golf swing. Understanding the throwing phases allows clinicians to correlate symptoms at particular phases of the motion to pathology, avoid treatments that may reverse anatomic features that were adapted to throwing performance, and formulate sport-specific rehabilitation protocols that optimize return to previous level of play.12,13 For golf enthusiasts considering arthroplasty, a similar approach to understanding the golf swing and how different shoulder arthoplasty implants (TSA vs RSA vs HA) contribute to those swing mechanics, may aid in counseling and improve satisfaction. Dukan et al 2 examined the clinical impact of RSA or TSA on particular phases of the golf swing. The investigators found that for the left (front) arm, the follow-through was the most painful portion of the swing after RSA and TSA, giving credence to external rotation deficits after RSA being relevant to golf performance. On the right (back) arm, impact and follow-through were the most painful, corresponding to subscapularis and pectoralis major activity. In the current review, we did not examine whether the subscapularis was repaired, which would be interesting to know considering another study’s findings that subscapularis repair resulted in higher rates of return to golf. 7
Together, these studies may provide a basis for patients to anticipate changes to their swing and handicap after surgery and for rehabilitation efforts to include periscapular muscle strengthening. In addition, the range of motion during the swing in golfers older than 70 years swings—particularly external rotation and adduction—may not be possible to regain after RSA, and this could help explain the less favorable performance changes and return to golf after RSA compared with anatomic designs.4,17,18 Postoperative protocols and restrictions for return to golf after arthroplasty would be helpful for surgeons hoping to optimize time to return while not adding to early complication risks, such as subscapularis failure, instability, and acromial stress fractures. The stepwise protocol by Jensen and Rockwood 9 that progresses from putting and chipping to full swings with a driver offers an easy-to-follow return-to-golf protocol but requires updating with the latest evidence-based information. Although there is no evidence to suggest earlier mechanical failures or increasing complications in athletic patients after RSA and TSA, restrictions such as teeing the ball to avoid forceful impact and using a pushcart are easy targets to limit risks.
Limitations
This review has multiple limitations, the first being that the number of included studied was small and thus insufficient to draw any statistically significant conclusions from the data. Second, the studies reviewed were of relatively low evidence. Many of the studies did not separate their data and return-to-sport success rate based on the type of arthroplasty procedure performed. Although there were 172 patients with reported return-to-golf rates, only 107 of these patients were classified by the type of arthroplasty that they received, whereas the others were unspecified. On an individual level, many aspects contribute to a patient being able to return to sports apart from shoulder arthroplasty success. For example, in the study by Jensen and Rockwood, 9 only 1 patient did not return to golf, and that was due to debilitating osteoarthritis in his hip and knee and not due to shoulder arthroplasty failure. Other studies reported contributing factors that led to patients not returning to sports, including death, the presence of other limiting comorbidities aside from joint arthralgia, and a loss of interest in participating in sport activities.
This review suggests that there are multiple future directions for studying return to golf after shoulder arthroplasty. One would be analyzing differences in return to golf based on whether arthroplasty was performed on the front or back arm of the golf swing, given the differences in their muscle activation patterns. As modern templating software improves the surgeon’s ability to understand the impact of component position on postoperative range of motion, it would be interesting to simulate whether preoperative planning can be used to optimize range of motion needed for a golf swing. Motion laboratory analysis on seniors’ golf swings after shoulder arthroplasty—especially RSA—can add to our understanding of the motion requirements of a golf swing in this age group. Studying technical and implant decisions such as subscapularis repair and different glenosphere center of rotations would benefit preoperative planning. A standardized evidence-based guideline of responses to common questions asked by golfers, including return-to-play protocols, discomfort with sport, changes in performance, and restrictions, would help guide surgical decision-making regarding surgical technique and postoperative restrictions, especially given the increasing patient interest in postoperative performance in different aspects of golf that are measurable, such as driving distance and handicaps. Although efforts to optimize return to golf should continue, patients’ expectations should be tempered to more realistic outcomes, including pain relief and ability to perform daily functions. Return to golf is likely for all shoulder arthroplasty procedures but should be used cautiously as a driver for the decision to undergo arthroplasty.
Conclusion
The rate of return to golf after shoulder arthroplasty was found to be highest after TSA (78%) compared with RSA (59%) and HA (64%). Performance was less affected by TSA and HA than by RSA. The most commonly reported duration before returning to the full 18 holes was 5 to 6 months, but patients were able to return to putting and chipping earlier. It is difficult to draw any statistically significant conclusions from the current data on this topic, as the sample size was small and the studies were of low evidence. Higher evidence studies are required in order to provide evidence-based responses to common questions asked by golfers, including return-to-play protocols, discomfort with sport, changes in performance, and restrictions. Such evidence will help guide surgical decision-making regarding surgical technique and postoperative restrictions.
Footnotes
Final revision submitted July 31, 2023; accepted August 18, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.L. has received education payments from Goode Surgical, consulting fees from Arthrex, nonconsulting fees from Arthrex, and royalties from Arthrex. A.S. has received education payments from Arthrex, ImpactOrtho, and Medinc of Texas; consulting fees from Medacta; royalties from Arthrex and Medacta; and honoraria from Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.