
Abstract
Background:
Generalized joint laxity (GJL) is a risk factor for inferior outcomes after the modified Broström procedure for chronic lateral ankle instability, while anatomic reconstruction with tendons is more inclined to be recommended. However, whether anatomic reconstruction could achieve better results than the modified Broström procedure in patients with GJL is unknown.
Purpose:
To compare clinical outcomes and return to sports between anatomic reconstruction and the modified Broström procedure in patients with GJL.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with GJL (Beighton score ≥4) who underwent either the modified Broström procedure or anatomic reconstruction with gracilis autografts between 2017 and 2020 were reviewed. Included were 19 patients who underwent anatomic reconstruction (reconstruction group) and 49 patients who underwent the modified Broström procedure (MBP group). Clinical outcomes were compared using the Foot and Ankle Outcome Score (FAOS) and the Karlsson score. The rates of return to preinjury level in high-demand sports, sprain recurrence, and range of motion between the 2 groups were also compared.
Results:
The mean follow-up duration was 38.3 months in the reconstruction group and 43.7 months in the MBP group. The FAOS and Karlsson scores improved significantly after surgery in both groups (P < .001 for all), with the reconstruction group having significantly higher postoperative FAOS-Sports scores (87.9 ± 8.9 vs 80.5 ± 11.6; P = .015) and Karlsson scores (86.9 ± 6.1 vs 82 ± 8.4; P = .025) than the MBP group. The rate of return to preinjury high-demand sports was higher in the reconstruction group than in the MBP group (73.3% vs 38.9%; P = .034). The MBP group had a significantly higher rate of sprain recurrence (22.4% vs 0%; P = .027). More patients reported dorsiflexion restriction in the reconstruction group (n = 4; 21.1%) than in the MBP group (n = 1; 2%) (P = .019); nonetheless, there was no noticeable effect on daily life and sports.
Conclusion:
Better clinical outcomes, less sprain recurrence, and a higher rate of return to preinjury high-demand sports were found after anatomic reconstruction with free tendons compared with the modified Broström procedure in patients with GJL. Anatomic tendon reconstruction can be recommended for such patients, especially those participating in high-demand sports.
Keywords
Lateral ankle sprains, which involve the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (CFL), are among the most common sports injuries. 7 Patients with failed nonoperative treatment are likely to develop chronic lateral ankle instability (CLAI) with persistent ankle pain, swelling, and giving way.5,8 The modified Broström procedure is the gold standard for CLAI and has been proven to allow favorable outcomes.10,16,32 However, some authors recommend restoring stability by reconstructing the ankle with free tendons in patients participating in high-demand sports, those with poor residual ligament quality, or those with generalized joint laxity (GJL).18-20 In such cases, poor outcomes and recurrent instability were reported, while anatomic reconstruction using autografts to duplicate the ligaments in the origin and insertion can restore functional and mechanical stability.
GJL, defined as increased joint range of motion (ROM) beyond normal limits with a Beighton score25,31≥4, is considered to contribute to the stretch out of repaired ligament as a result of inherent connective tissue extensibility. 22 GJL is identified as a predisposing factor for primary traumatic anterior shoulder dislocation and is negatively associated with stability and functional outcomes after anterior cruciate ligament reconstruction (ACLR).12,13 Regarding the ankle, some studies have reported poor outcomes after the open modified Broström procedure in GJL cases.21,33 Although anatomic reconstruction with autografts or allografts is recommended in such cases, no studies have compared the outcomes between anatomic reconstruction with free tendons and the modified Broström procedure. Evidence to support anatomic reconstruction surgery in these patients is lacking.
The purpose of the present study was to compare the clinical outcomes and return to preinjury sports between anatomic reconstruction with gracilis tendon autografts and modified Broström repair for CLAI in patients with GJL. It was hypothesized that anatomic reconstruction would achieve superior clinical outcomes, ankle stability, and sports recovery compared with the modified Broström procedure in GJL cases. The results of this study may provide additional evidence for indications for anatomic reconstruction surgery, thereby informing surgical strategy choices in CLAI patients with GJL.
Methods
The study protocol received institutional review board approval. All patients who underwent the modified Broström procedure and anatomic reconstruction with an autologous gracilis tendon between January 2017 and December 2020 were reviewed. The decision to perform the surgical procedure was based on the quality of the residual ligament. The inclusion criteria were as follows: (1) a traumatic history of at least 1 significant ankle sprain; (2) persistent clinical symptoms—including pain, swelling, “giving way” sense, feeling of instability, or recurrent sprain for at least 6 months—and 3 months of failed conservative treatment, such as physical rehabilitation and strengthening exercises; (3) mechanical instability, confirmed by ankle anterior drawer test and varus stress test; (4) magnetic resonance imaging findings of an attenuated, thickened, or absent ATFL; and (5) GJL, defined as a Beighton score ≥4. The exclusion criteria were as follows: (1) previous history of ankle surgery; (2) deltoid ligament injury, severe fracture, or open trauma; (3) severe osteochondral lesions of the talus (OLTs) requiring osteochondral transplantation; (4) early-stage ankle arthritis (Takakura arthritis classification stage ≥3); and (5) neuromuscular disorders. Based on the inclusion and exclusion criteria, 74 patients with GJL were enrolled in this study—19 underwent anatomic reconstruction (reconstruction group), and 55 underwent the modified Broström procedure (MBP group). All patients in the reconstruction group completed the follow-up (follow-up rate, 100%), and 49 patients in the MBP group completed the follow-up (follow-up rate, 49/55 = 89.1%) (Figure 1). In the reconstruction group, 15 patients (2 patients were professional athletes) participated in high-demand sports (defined as cutting, pivoting, or jumping sports; eg, basketball, badminton, boxing, and soccer), and the remaining 4 patients participated in recreational sports (eg, skiing, dancing, and running). In the MBP group, 36 patients (1 patient was a professional athlete) participated in high-demand sports, 6 participated in recreational sports, and 7 did not participate in any sports. Patient characteristics are described in Table 1.

A diagram showing patients’ enrollment procedure in the study. BMI, body mass index; MBP, modified Broström procedure.
Characteristics of the Study Patients a

Data are reported as mean ± SD or n. BMI, body mass index; MBP, modified Broström procedure.
Surgical Technique
All procedures were performed by D.J., Q.G., Y.H., and C.J. from the same department. The patient was placed in a supine position under general or spinal anesthesia. Arthroscopy was routinely performed to evaluate intra-articular lesions—including OLTs, osteophytes, avulsion fractures, etc—and address them if necessary. The residual ligament quality was also inspected by arthroscopic examinations. When the ligament was absent under arthroscopy, the open anatomic reconstruction with a gracilis autograft was performed. The open modified Broström procedure or open anatomic reconstruction with a gracilis autograft was performed according to previous studies.26,27
For the modified Broström procedure, an arc-shaped incision of 4 cm was made along the lower edge of the lateral malleolus. The remnant of the ATFL and the CFL was identified and anatomically repaired with 2 or 3 suture anchors (Mitek Mini-GII; Johnson & Johnson). After reinforcement with the inferior extensor retinaculum, the ankle was stabilized with slight dorsiflexion and eversion.
When an absent ligament was found, open anatomic reconstruction was performed. A gracilis tendon of the ipsilateral knee was harvested and prepared for autologous transplantation. A 4- to 5-cm oblique incision was made at the distal fibula. One merged tunnel of 4.5 mm was drilled at the fibular insertion of both the ATFL and the CFL. Two 4.5-mm transversely penetrating tunnels were drilled at the center of the ATFL and CFL footprints through the talus and calcaneus, respectively. With the help of guide sutures, the prepared autograft was folded, and the folded end was introduced into the fibular tunnel and fixed by an interference screw (5 mm Milagro; Johnson & Johnson). The 2 ends were led through the talar and calcaneal tunnels and fixed with 2 interference screws (5 mm Milagro; Johnson & Johnson) in the neutral ankle position.
Postoperative Rehabilitation
All patients followed the same rehabilitation plan as follows. After the surgery, the ankle was immobilized using a short leg cast for the first 2 weeks. Partial weightbearing was allowed at weeks 2 through 4 and gradually transitioned to full weightbearing with a walking boot. From week 6, rehabilitation procedures were performed, including concentric and eccentric muscle strengthening of the hip, knee, and ankle joints and balance exercises. Then, the patients were allowed to return to daily activities and sports within their tolerance.
Clinical Evaluations
GJL was assessed by the Beighton 9-point scoring system as reported by previous studies21,33: (1) 1 point was awarded if the metacarpophalangeal joint was passively dorsiflexed more than 90°; (2) 1 point was awarded for passive apposition of the thumbs to the flexor aspects of the forearms; and (3) the elbows and knees were each scored 1 point if they could be hyperextended over 10°. In addition, 1 point was awarded if the palms rested easily on the floor with the knees straight.
The Foot and Ankle Outcome Score (FAOS) 23 and the Karlsson score 11 were used to assess clinical outcomes before surgery and at the final follow-up. The FAOS questionnaire with 42 items and 5 subscales (Pain, Other Symptoms, Activities of Daily Living, Sport and Recreation Function [Sports], and Quality of Life) scored up to 100 points and is used to assess patient-relevant outcomes. The Karlsson scoring system is used to evaluate the function of the ankle joint and includes 8 items (ankle instability, pain, swelling, stiffness, work, stair climbing, running, and support) scored up to 100 points.
In addition, the rate of return to preinjury level for athletes of high-demand sports and the rate of sprain recurrence were assessed. Passive ROM of the ankle joint was measured using a goniometer with the patients seated at follow-up, and ROM restriction was defined as a deficit of ≥5° on the operated side compared with the contralateral nonoperated side. 26 All the assessments were performed by 2 independent reviewers.
Statistical Analysis
All the data are presented as the mean ± standard deviation for normally distributed variables, median (interquartile range) for skewed variables, and frequency (percentage) for categorical data. The Shapiro-Wilk normality test was used for normal distributions. The independent-samples t test or the Wilcoxon signed-rank test was applied to compare clinical outcomes between the reconstruction and MBP groups. The Pearson chi-square test was used to compare differences in categorical data (ie, rate of return to sports, rate of sprain recurrence, and ROM) between the 2 groups. Statistical analysis was performed using the Statistical Package for the Social Science (SPSS 25.0; IBM) software. Statistical significance was established at P < .05.
The sample size calculation was processed by Power Analysis and Sample Size (PASS 15.0; NCSS). Given the difference in the Karlsson score between the 2 groups, we calculated that 19 patients in the reconstruction group and 38 patients in the MBP group would provide a power of 83.4% when the significance level was set at .05.
Results
At the final follow-up, the FAOS and Karlsson scores were significantly improved compared with the preoperative levels in the 2 groups (P < .001 for all). The postoperative FAOS-Sports score (87.9 ± 8.9 vs 80.5 ± 11.6; P = .015) and the Karlsson score (86.9 ± 6.1 vs 82 ± 8.4; P = .025) in the reconstruction group were significantly higher than those in the MBP group. In the reconstruction group, 12 patients returned to preinjury sports—11 patients returned to high-demand sports, and 1 patient returned to preinjury recreational activities. In the MBP group, 20 patients returned to preinjury sports—14 returned to high-demand sports and 6 returned to preinjury recreational activities. The rate of high-demand athletes who returned to preinjury level sports was significantly higher in the reconstruction group than in the MBP group (73.3% vs 38.9%; P = .034). There was a significantly higher rate of sprain recurrence in the MBP group than in the reconstruction group (22.4% vs 0%; P = .027) (Table 2).
Comparison of Outcomes Between the Reconstruction and the MBP Groups a

Data are reported as mean ± SD or n (%). Bold P values indicate statistically significant differences between groups (P < .05). FAOS, Foot and Ankle Outcome Score; MBP, modified Broström procedure; Postop, postoperative; Preop, preoperative; QOL, Quality of Life.
There were 15 athletes of high-demand sports in the reconstruction group and 36 in the MBP group.
Additional Procedures and Complications
There were no significant differences in intra-articular lesions, including OLTs, osteophytes, and avulsion fractures, in the distal fibula between the 2 groups (Table 3). No wound healing delay or infection was reported, and no patients underwent revision surgeries in either group. In the reconstruction group, no patient reported disability from the graft harvest. The incidence of dorsiflexion restriction in the reconstruction group (n = 4; 21.1%) was higher than that in the MBP group (n = 1; 2%) (P = .019) at the final follow-up (Table 2). These patients could not squat fully but had no difficulty in daily and sports activities.
Comparisons in Intra-articular Lesions Between the Reconstruction Group and the MBP Group a
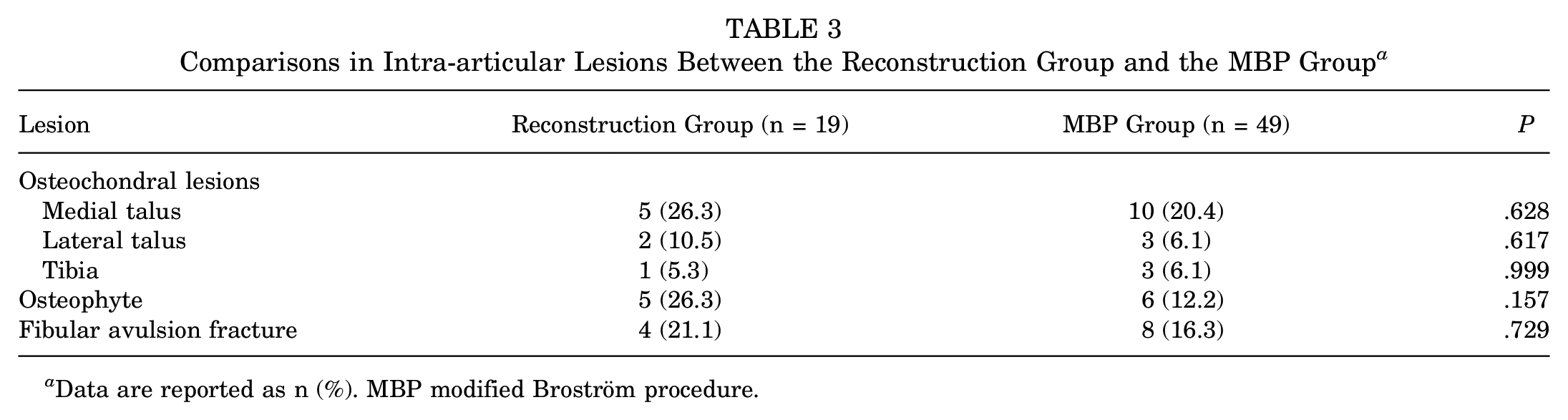
Data are reported as n (%). MBP modified Broström procedure.
Discussion
The most important finding of this study was that better clinical outcomes, less sprain recurrence, and a higher rate of return to preinjury level in high-demand sports were shown for anatomic reconstruction with free tendons compared with modified Broström repair in CLAI patients with GJL. Anatomic reconstruction with tendons might be more recommended for such patients, especially those with high exercise requirements. To our knowledge, this is the first study to compare the clinical outcomes and return to sports between the modified Broström procedure and anatomic reconstruction using autografts in GJL patients.
In this study, anatomic reconstruction with gracilis autografts yielded significantly better FAOS-Sports scores (87.9 ± 8.9 vs 80.5 ± 11.6; P = .015) and Karlsson scores (86.9 ± 6.1 vs 82 ± 8.4; P = .025) than modified Broström repair in patients with GJL. Some studies have reported similar short- or long-term outcomes between these procedures in non-GJL patients.18,19,27 However, previous studies indicated that GJL was a risk factor for inferior clinical outcomes after modified Broström repair21,33 Xu and Lee 33 reported a Karlsson score of 87.4 after modified Broström repair in GJL patients with a 27.4-month follow-up. Park et al 21 reported a Karlsson score of 82.8 after repair with a 62.3-month follow-up. The present study showed a similar Karlsson score (82) in the MBP group, which might be associated with GJL on ligament repair. Nonetheless, significantly higher FAOS-Sports and Karlsson scores were found in the reconstruction group than in the MBP group in this study. This might be due to different surgical techniques. Although the modified Broström repair was the gold standard for treating CLAI, it was based on remnant ligamentous quality. In patients with GJL, the repaired ligament is likely to stretch out as a result of inherent tissue extensibility. 22 The anatomic reconstruction technique uses tendons to replace the damaged ligaments in the anatomic insertions and restore joint function, which may provide a more stable ankle. 30
In the present study, the rate of returning to preinjury level in high-demand athletes was significantly higher in the reconstruction group versus the MBP group. Previous studies indicated no significant difference in activity level measured by the Tegner activity score between anatomic reconstruction and repair in non-GJL cases.18,19 The exact effect of GJL is still under investigation. Muscle strength, postural stability, and neuromuscular control were also related to return to sports.14-16 In CLAI patients, postural stability, neuromuscular control and muscle strength, or endurance has been found to decrease. 15 Modified Broström repair may improve muscle strength and endurance and dynamic postural stability.9,16 However, no study has investigated these factors in anatomic lateral ankle ligament reconstruction with free tendons, and future studies are needed. Some authors have reported that the signal-to-noise ratio (SNR) of the ATFL was correlated with the remnant ligamentous quality, and a lower SNR was associated with a higher rate of return to sports after modified Broström repair.1,17 The SNRs of the tunnel walls and intraosseous tendon graft decreased with the revascularization process during bone-tendon healing after ACLR. 28 However, there have been no studies on bone-tendon healing after anatomic lateral ankle ligament reconstruction with free tendons. The effect of the SNR on the healing process and the return to sports deserves investigation in the future.
No sprain recurrence was found in the reconstruction group, while 11 (22.4%) patients resprained the ankle after surgery in the MBP group. The rate of recurrent sprain in the MBP group was similar to the results in a previous study, 21 and no study has reported the recurrence of sprain after anatomic reconstruction in patients with GJL. In a long-term follow-up study in non-GJL patients, Su et al 27 reported a significantly higher proportion of sprain recurrence after the modified Broström procedure compared with anatomic reconstruction. The present study showed similar results to Su et al in patients with GJL. The lower resprain rate in the reconstruction group might have resulted from increased mechanical stability compared with direct repair. Joint stability mostly relies on ligaments, muscles, tendons, joint capsule, and surrounding soft tissue. 29 The inherent collagen abnormality present during tissue healing may be associated with ligamentous laxity and instability2,24 and may increase sprain recurrence after the modified Broström procedure. Anatomic reconstruction with autografts was reported to provide increased biomechanical strength and stiffness, resulting in a stable ankle. 4 In addition, the relatively shorter follow-up time and smaller sample size in the reconstruction group might also have influenced the results.
In terms of ankle ROM, 4 patients (21.1%) in the reconstruction group reported dorsiflexion restriction, while 1 patient (2%) had dorsiflexion limitation in the MBP group, which was a significant group difference (P = .019). Although the patients with dorsiflexion restriction could not squat fully, they had no difficulty in daily and sports activities. Ligament reconstruction with free tendons does have the potential risk of limited ROM and might result in inferior outcomes. Ellis et al 6 reported that 6 patients (54.5%) had ROM restrictions, and 1 complained of moderate activity restrictions. Su et al 26 reported a 12.5% ROM restriction rate after anatomic reconstruction with the Y-graft technique. This might be due to the greater tension of graft reconstruction than repair. Li et al 18 reported that the thickness of the graft tendon was twice that of the repaired ligament, which might result in a tension increase and ROM restriction. The locations of bone tunnels, graft length, and fixation position of the ankle might also add to the potential for overstraining and even affect the ROM. Additional studies are needed to explore the impact of these factors to avoid ROM restriction.
Limitations
There were some limitations here. First, the level of evidence was limited by its retrospective design. Although 83.4% of power was achieved by power analysis, the sample size was relatively small. Prospectively designed studies with larger sample sizes are needed in the future. Second, most assessments were subjective, and stress radiography was not performed to evaluate ankle stability. Third, the indications of the 2 groups were somewhat different and might lead to selection bias. Although there was no difference in baseline data between the 2 groups, those in the anatomic reconstruction group with poor ligament quality might be associated with decreased muscle strength and more significant overall ankle instability compared with those in the MBP group. Further prospective studies with a large sample and longer follow-ups are needed to provide more evidence about the surgical strategy choice for CLAI patients with GJL. Third, many surgeons now use an internal brace or suture tape to augment the modified Broström procedure. Cho et al 3 have also reported favorable outcomes in patients with GJL to treat CLAI. Therefore, future comparison between modified Broström repair with suture tape augmentation and modified Broström repair or anatomic reconstruction with free tendons in patients with GJL is worth investigating.
Conclusion
Better clinical outcomes, less sprain recurrence, and a higher preinjury sports recovery rate were shown for anatomic reconstruction with free tendons compared with the modified Broström procedure in CLAI patients with GJL. Anatomic tendon reconstruction can be recommended for such patients, especially those participating in high-demand sports.
Footnotes
Final revision submitted July 15, 2023; accepted August 21, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A grant was received from the National Key Research and Development Program of China (2019YFB1706905). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital Medical Science Research Ethics Committee (ref No. M2022515).