
Abstract
Background:
Ruptures of the quadriceps tendon present most frequently in older adults and individuals with underlying medical conditions.
Purpose:
To examine the relationship between patient-specific factors and tear characteristics with outcomes after quadriceps tendon repair.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective review was conducted on all patients who underwent quadriceps tendon repair between January 1, 2016, and January 1, 2021, at a single institution. Patients <18 years and those with chronic quadriceps tendon tears (>6 weeks to surgery) were excluded. Information was collected regarding patient characteristics, presenting symptoms, tear characteristics, physical examination findings, and postoperative outcomes. Poor outcome was defined as a need for revision surgery, complications, postoperative range of motion of (ROM) <110° of knee flexion, and extensor lag of >5°.
Results:
A total of 191 patients met the inclusion criteria. Patients were aged 58.5 ± 13.2 years at the time of surgery, were predominantly men (90.6%), and had a mean body mass index (BMI) of 32.2 ± 6.3 kg/m2. Patients underwent repair with either suture anchors (15.2%) or transosseous tunnels (84.8%). Postoperatively, 18.5% of patients experienced knee flexion ROM of <110°, 11.3% experienced extensor lag of >5°, 8.5% had complications, and 3.2% underwent revision. Increasing age (odds ratio [OR], 1.03 [95% CI, 1.004-1.07]) and female sex (OR, 3.82 [95% CI, 1.25-11.28]) were significantly associated with postoperative knee flexion of <110°, and increasing age (OR, 1.08 [95% CI, 1.04-1.14]) and greater BMI (OR, 1.14 [95% CI, 1.05-1.23]) were significantly associated with postoperative extensor lag of >5°. Current smoking status (OR, 15.44 [95% CI, 3.97-65.90]) and concomitant retinacular tears (OR, 9.62 (95% CI, 1.67-184.14]) were associated with postoperative complications, and increasing age (OR, 1.05 [95% CI, 1.02-1.08]) and greater BMI (OR, 1.08 [95% CI, 1.02-1.14]) were associated with risk of acquiring any poor outcome criteria.
Conclusion:
Patient-specific characteristics—such as increasing age, greater BMI, female sex, retinacular involvement, and current smoking status—were found to be risk factors for poor outcomes after quadriceps tendon repair. Further studies are needed to identify potentially modifiable risk factors that can be used to set patient expectations and improve outcomes.
Ruptures of the quadriceps tendon are potentially devastating injuries that can lead to significant morbidity. Although relatively uncommon, they present most frequently in older adults and those with underlying medical conditions. 12 Specifically, spontaneous bilateral ruptures have been shown to be associated with gout, diabetes, and steroid use. 16 However, acute traumatic tears classically present after a fall, with the patient unable to extend the knee. 26 While some tears can be treated conservatively, surgical repair is usually indicated to fully restore the functionality of the extensor mechanism of the knee. 17 A majority of quadriceps tears are avulsions from the proximal pole of the patella, and the repair of the quadriceps tendon is usually performed using either suture anchors or transosseous tunnels through the patella to restore the bone-tendon interface. 37
Patient-specific factors have been shown to be predictive of poor outcomes after surgical treatment of several other knee conditions. 28 For example, a body mass index (BMI) of >30 kg/m2 has been shown to increase the risk of complications after multiligamentous knee injuries and to be predictive of an inferior range of motion (ROM) after knee arthroplasty.10,33 However, there is a paucity of literature regarding the effect of risk factors—such as age, BMI, and smoking—on outcomes of quadriceps tendon repair.
This study aimed to examine the effect of different patient and intraoperative factors on the outcome after quadriceps tendon repair. It was hypothesized that older age, higher BMI, and a history of smoking would be associated with worse outcomes after quadriceps tendon repair.
Methods
A retrospective review was conducted on patients who underwent quadriceps tendon repair between January 1, 2016, and January 1, 2021, at a single institution, searching the patient database using Current Procedural Terminology codes 27835 and 27836. Patients with definitive documentation of a quadriceps tendon tear within the operative report were included in the study. Those patients with (1) multiligamentous knee injury, (2) age <18 years, or (3) previous ipsilateral quadriceps tendon tear were excluded. Information was collected regarding patient characteristics, presenting symptoms, tear characteristics, physical examination findings, and postoperative outcomes. This study was considered exempt from institutional review board approval.
Preoperative Characteristics
Preoperative descriptive data and intraoperative findings listed in Table 1 were collected. Moreover, the presence of potential risk factors and comorbidities that affect soft tissue healing was determined in each patient—including body mass index (BMI), hypertension, hyperlipidemia, diabetes mellitus, thyroid dysfunction, chronic kidney disease, history of steroid or fluoroquinolone use, and smoking history (eg, current, former, never). For this study, age and BMI were analyzed as continuous variables.
Patient Characteristics (N = 191) a

Data are reported as mean ± SD or n (%). BMI, body mass index.
Radiographic Evaluation
Magnetic resonance imaging (MRI) was utilized to determine tear thickness, location, concomitant pathology, amount of retraction, retinacular involvement, tendon degeneration, and presence of arthritic changes, which were collected as well. Retinacular involvement was defined as edema and thickening of the retinaculum compatible with a partial tear. On MRI, tendon degeneration was defined as a thickened tendon with signal heterogeneity instead of the usual low signal intensity associated with a healthy tendon. The amount of retraction was calculated by measuring the distance from the tendon stump to the retracted muscle belly tendon.
Surgical Technique and Postoperative Rehabilitation
The quadriceps tendon repair techniques used were either fixation through transosseous patellar tunnels or with suture anchors in the proximal pole of the patella. Regardless of the fixation method, Fiberwire (Arthrex ) was passed through the medial and lateral halves of the quadriceps tendon in a Krakow fashion. For the transosseous tunnel group, 3 bone tunnels were drilled in the patella from the proximal pole of the patella to the distal pole and through the patellar tendon. Then, the free limbs of the FiberWire were passed through the tunnels and tied over the bony bridge on the distal pole of the patella. For the suture anchor group, the medial and lateral free limbs of the FiberWire were loaded into 2 SwiveLock anchors (Arthrex ), respectively, and those anchors were then placed in the proximal pole of the patella. Both fixation constructs are secured with the knee in full extension.
The initial postoperative rehabilitation protocol included a 6-week period in a hinged knee brace locked in extension for ambulation with a ROM of 0° to 30° at 2 weeks postoperatively, 0° to 70° at 4 weeks postoperatively, 0° to 90° at 6 weeks postoperatively, and full ROM at 8 weeks postoperatively. Weightbearing was allowed immediately postoperatively with a hinged knee brace locked in full extension for the first 6 weeks. After 6 weeks, the brace was unlocked for 2 weeks and then discontinued at 8 weeks. Patients were allowed to return to full activities by 4 months postoperatively.
Postoperative Outcome Measures
Poor outcomes were defined as follows: (1) requiring revision tendon repair/reconstruction; (2) reported complications; (3) postoperative knee flexion ROM <110° as measured passively with a goniometer; and (4) extensor lag of >5° as measured using active motion with a goniometer. Complications that were considered poor outcomes included postoperative infection, quadriceps retear, arthrofibrosis, deep vein thrombosis, flexion contracture, septic arthritis, and persistent gapping of the repair site. The final ROM was recorded at the 6-month postoperative visit.
Statistical Analysis
A 2-tailed t test or the Mann-Whitney U test (continuous variables) and the chi-square test or the Fisher exact test (categorical variables) were used to determine significant risk factors for poor outcomes. Statistical significance was set at P < .05. Variables with a significant value for bivariate comparison were then analyzed for prediction potential using a multivariate logistic regression model for each category of poor outcome. Because of the limited occurrences within certain poor outcome cohorts, only variables with the most significant P value on bivariate analysis were chosen for multivariate regression to minimize overfitting the regression model. All statistical analyses used R Studio Version 4.1.2 (R Project for Statistical Computing).
Results
The study cohort comprised 191 patients (173 men and 18 women), with a mean age of 58.5 ± 13.2 years (Table 1). The mean age of women in this cohort was 58 ± 13.2 years as compared with men, which was 59 ± 13.2 years. The mean BMI for this cohort was 32.2 ± 6.3 kg/m2, with no differences in baseline characteristics between sexes. The most common surgical procedure was transosseous fixation (n = 162), followed by suture anchors (n = 29). Preoperative Tegner scores were not significantly associated with the poor outcomes examined. The mean time to surgery for this cohort was 15 ± 8 days. The time to surgery was not significantly associated with any of the predetermined poor outcomes (Table 2).
Radiographic Findings in the Overall Cohort a
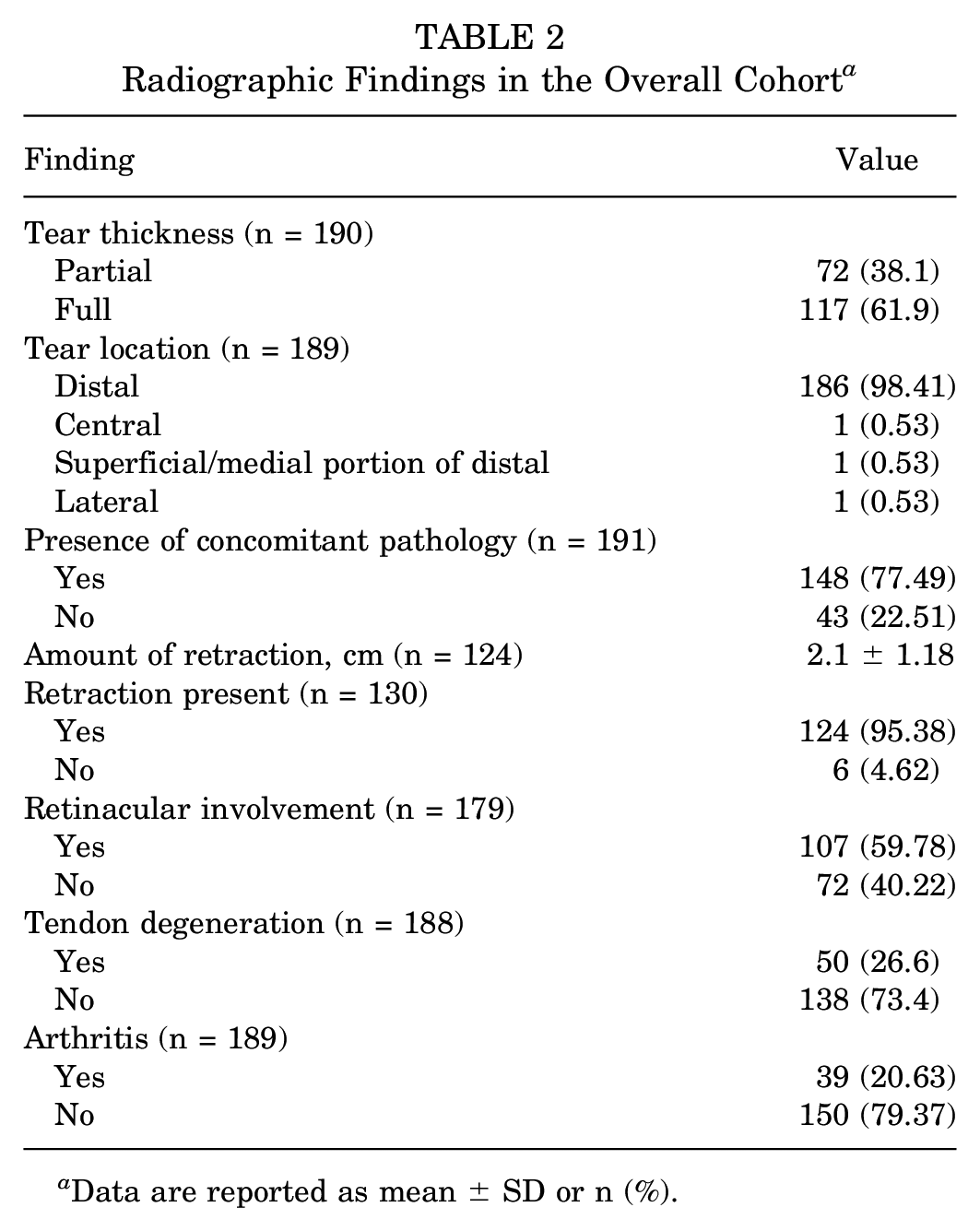
Data are reported as mean ± SD or n (%).
Radiographic Findings
Tear location was assessed via magnetic resonance imaging (MRI) and predominantly distal (98.4%), with a large portion of patients experiencing concomitant pathology (77.5%), such as meniscal injury, anterior cruciate ligament tear, and extra articular ligamentous injury (Table 3). A significant difference was found in those with MRI evidence of retinacular involvement that subsequently developed complications (OR, 9.62 [95% CI, 1.67-184.14]).
Postoperative Outcomes in the Overall Cohort a

Data are reported as mean ± SD or n (%). ROM, range of motion.
Loss of Knee Flexion ROM
Of the 191 patients within this cohort, 178 had postoperative ROM data. The mean postoperative knee flexion for the cohort was 124.3°± 18°. On postoperative physical examination, 18.54% of patients experienced loss of ROM categorized as <110° of knee flexion, with a mean ROM of 122.79°± 18.92°. Bivariate analysis demonstrated that sex (P = .020), endocrine disorders (P = .005), and chronic kidney disease (P = .032) were associated with decreased postoperative ROM. Logistical regression showed that increased age (odds ratio [OR], 1.03 [95% CI, 1.004-1.07]) and female sex (OR, 3.82 [95% CI, 1.25-11.28]) were associated with postoperative knee flexion of <110° (Table 4). Although significant in bivariate analysis, endocrine disorders and chronic kidney disease were not analyzed in the regression because of the limited occurrences within the total cohort. In addition, when subanalyzed by surgical technique, there were no significant differences in rates of loss of ROM between transosseous (16.7%) and suture anchor repair (20.6%) (P = .585).
Multivariate Analysis for Poor Outcomes (Postoperative Knee Flexion ROM <110°) a

Boldface P values indicate statistical significance (P < .05). OR, odds ratio; ROM, range of motion.
Postoperative Extensor Lag
Of the 191 patients assessed, 186 patients had documentation for knee extension strength postoperatively. On the postoperative physical examination, 11.3% experienced an extensor lag >5°. Bivariate analysis reported significance for age (P = .017), preoperative Tegner (P = .072), and smoking status (P = .044). Logistic regression demonstrated that a postoperative extensor lag of >5° was significantly associated with an increase in age (OR, 1.08 [95% CI, 1.04-1.14]) and BMI (OR, 1.14 [95% CI, 1.05-1.23]). Patient smoking status did not significantly affect postoperative extension lag (Table 5). In addition, in the subanalysis according to surgical technique, there were no significant differences in the rates of postoperative extensor lag between transosseous (10.5%) and suture anchor repair (13.8%) (P = .515).
Multivariate Analysis for Poor Outcomes (Postoperative Extensor Lag >5°) a
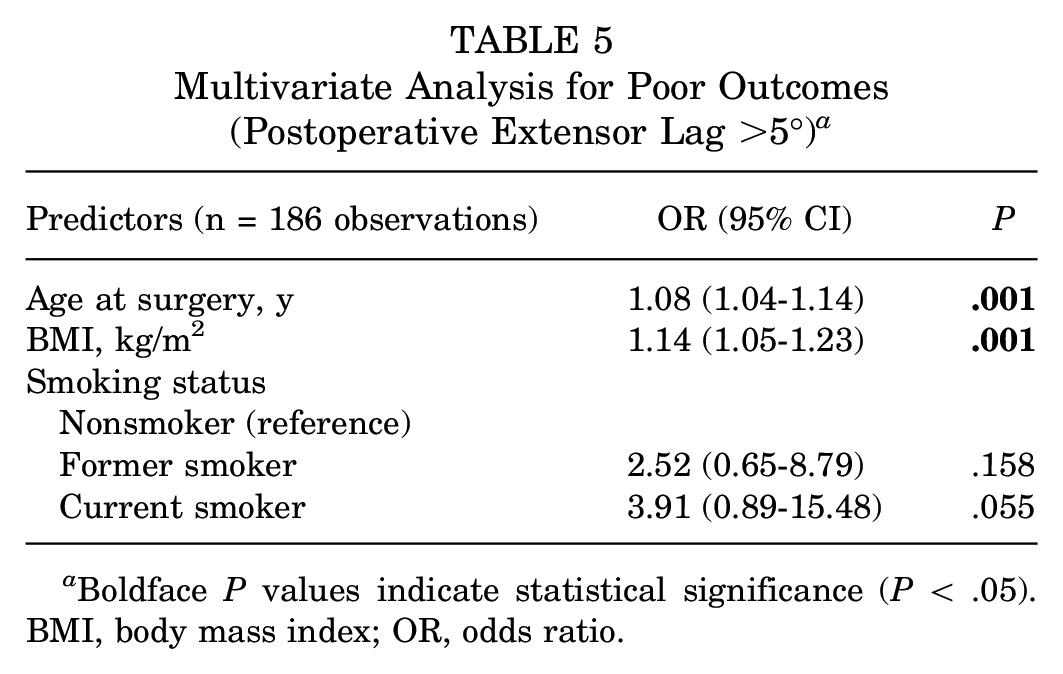
Boldface P values indicate statistical significance (P < .05). BMI, body mass index; OR, odds ratio.
Complications
Within this cohort, 8.51% had any postoperative complications, including postoperative infection (n = 2), quadriceps retear (n = 6), arthrofibrosis (n = 3), deep vein thrombosis (n = 1), septic arthritis (n = 2), and persistent gapping of the repair site (n = 2). Bivariate analysis showed a significant association with evidence of retinacular involvement (P = .008), tendon degeneration (P = .037), and smoking status (P < .001). Multivariate logistical regression showed that postoperative complications were significantly associated with current smoking status (OR, 15.44 [95% CI, 3.97-65.90]) and retinacular involvement assessed via MRI (OR, 9.62 [95% CI, 1.67-184.14]) (Table 6). Former smoking status and female sex were not significantly associated with an increased risk of postoperative complications. In addition, when subanalyzed by surgical technique, there were no significant differences in the rates of complications between transosseous (9.3%) and suture anchor repair (3.4%) (P = .474).
Multivariate Analysis for Poor Outcomes (Complications) a

Boldface P values indicate statistical significance (P < .05). OR, odds ratio.
Need for Revision Surgery
Revision quadriceps repair was required in 3.14% (n = 6) of patients in this cohort. When subanalyzed by surgical technique, there were no differences in rates of revision between transosseous (3.7%) and suture anchor repair (0%) (P = .593). Given the small sample size, regression analysis was not completed for this subgroup.
Overall Risk for Poor Outcomes
Patients who experienced any of the 4 specified poor outcomes were grouped into a “poor outcomes” cohort. Of the 191 patients, 54 were designated as poor outcome patients. Bivariate analysis according to outcomes is shown in Table 7. Logistic regression demonstrated that patients who were older (OR, 1.05 [95% CI, 1.02-1.08]) and had a greater BMI (OR, 1.08 [95% CI, 1.02-1.14]) were significantly more likely to experience 1 or more of the poor outcomes examined. Female sex did not have significance when accounting for all combined poor outcome variables. (P = .1334) (Table 8). In addition, the subanalysis of surgical techniques did not demonstrate any significant difference in rates of combined poor outcomes between transosseous repair (27.7%) and suture anchor repair (31%) (P = .893).
Bivariate Analysis According to Patients With and Without Poor Outcomes a

Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant differences between groups (P < .05). BMI, body mass index.
Multivariate Analysis for Combined Poor Outcomes a

Boldface P values indicate statistical significance (P < .05). BMI, body mass index; OR, odds ratio.
Discussion
The main findings of this study suggest that advanced age, greater BMI, female sex, evidence of retinacular involvement, and current smokers were significantly associated with poor outcomes such as loss of ROM, postoperative extensor lag, and complications. These findings are consistent with several previous studies on various orthopaedic procedures.1-3,13-15 Although not seen in the current study, other variables—such as hypertension and chronic kidney disease—have been implicated in previous studies. Lewis et al examined risk factors for infection after quadriceps tendon repair and found that hypertension and hypothyroidism were an independent risk factor for reoperation. 18 Similarly, hypertension has been shown to delay superficial wound healing and increases the risk of readmission in orthopaedic surgeries.1,5 In our study, bivariate comparisons of patients with hypertension, and all poor outcomes were not significantly associated.
The incidence of quadriceps tendon injury is classically associated with middle-aged men, peaking in the seventh decade and are regarded as uncommon in women of all age groups. 12 Many of the previous studies examining quadriceps tendon repair have an overwhelmingly large ratio of male to female participants, thereby leaving much to be known regarding outcome differences between sexes.7,8,24,31 Similarly, the cohort in this study was predominantly men. The present study found that women were significantly more likely to experience a decreased postoperative ROM (P = .015). Outcome differences between sexes are well documented in other areas of sports medicine, and authors have hypothesized that sex-specific risk factors—such as anatomic and hormonal differences—may be to blame.20,22,34 In the present study, baseline characteristics—such as age and BMI—were no different between men and women (P = .978 and P = .076, respectively) Similarly, there was no difference in time to surgery between men and women (P = .123). Given that the female sex was not statistically associated with the risk of combined poor outcomes, further studies are warranted with larger populations of female patients to discern whether differences exist between the sexes.
Spontaneous quadriceps tendon rupture usually occurs due to the degeneration of tendons in patients caused by systematic diseases such as end-stage renal disease, rheumatoid arthritis, diabetes mellitus, hyperparathyroidism, and long-term steroid use.4,29 An epidemiological study found that patients >60 years had a 3-fold increase in the incidence of spontaneous quadriceps tendon rupture compared with patients <40 years. 32 In the present cohort, there was no association between quadriceps tendon repair and hypertension, chronic kidney disease, or hyperlipidemia. Of note, the number of patients with chronic kidney disease (1.05%) was quite low in this cohort, and, as a result, there may not have been enough of a sample to observe an impact. Further, endocrine disorders were found to be significantly associated with combined poor outcomes on bivariate analysis. However, limited occurrences in the population did not support regression analysis.
Age at the time of surgery plays a significant role in our ability to recover after injury. Herron et al 15 found that orthopaedic trauma in older people is associated with a greater risk of mortality than for similar fractures in the young. 15 However, when it comes to outcomes after quadriceps tendon repair, a recent study has shown that patient reported outcomes in patients <40 years are equivalent to historical controls aged >40 years. 31 Notably, a considerable percentage of patients <40 years showed significant long-term sequelae, such as pain and stiffness, despite their youth. 31 As quadricep tendon injuries are most commonly seen in middle-aged men, our cohort aligns with the historical demographic of patients who undergo quadricep tendon repair. In contrast to previous findings, our study reveals a significant risk for decreased postoperative knee flexion, extensor lag, and poor overall outcomes as age increases. However, it is unclear whether the equivalent outcomes shown in previous studies truly capture the impact of age after quadriceps tendon repair or may be a consequence of higher demands and expectations of younger patients.
Increased BMI predisposes patients to a range of musculoskeletal and metabolic disorders. In a study by Cardoso et al, investigators found that obese patients had significantly worse long-term outcomes (namely, pain, poor function, and difficulties with activities of daily living) after an operatively treated ankle fracture with a follow-up of over a decade. 9 Similarly, in a recent systematic review by Macchi et al, 21 obesity was reported to increase the risk of tendinopathy, tendon tear, rupture, and postoperative complications after tendon surgery compared with the nonobese population. 21 Several studies that have examined soft tissue injuries of the knee have shown the negative impact of obesity on ROM, which is consistent with the findings of this study.6,19
Smoking has been implicated widely across medicine as associated with poor wound healing and an array of pathology. The documented effects of byproduct toxic compounds found within cigarette smoke—such as nicotine, carbon monoxide, and hydrogen cyanide—suggest possible mechanisms for impaired wound healing. 23 Yoshikawa and Katada 38 found that smoking could be associated with a risk of poor postoperative outcomes irrespective of the type of surgery performed. While this study does not directly investigate the effect of smoking cessation, a previous review showed that longer periods of smoking cessation are more effective for reducing the risk of complications after surgical procedures but with no threshold of time established. 36 Thus, there may still be a benefit to emphasizing smoking cessation in the perioperative period, even though quadriceps tendon tears are typically treated within a short period from initial injury. The efficacy of smoking cessation in the perioperative period is unclear, but physicians’ awareness of high-risk patients can help set expectations for outcomes.
This study did not find a significant association between time from injury to surgery and poor outcomes. However, in a previous systematic review by Ciriello et al, 11 worse outcomes were reported in delayed repairs after quadricep rupture. The mean time to surgery for this cohort was higher than reported in previous studies.27,31,35 Overall, all patients were treated within 6 weeks of injury at a mean of 15.01 ± 8.03 days. As the delay from injury to surgical repair increases, the complexity of the surgical repair also increases because of the development of scar contraction and soft tissue retraction. However, successful repair has been described up to 8 years after injury. 30 Further studies are needed with larger cohorts to determine the true effect of the timing of surgical repair on overall outcomes.
Limitations
Our study is not without limitations. First, the retrospective nature of the study limits the data collected to recorded information in the patient's electronic medical record. While 5 risk factors were found to significantly affect outcomes after quadriceps tendon repair, the cohort size was relatively small. Thus, there may be additional factors that affect outcomes that were not captured in this study. For example, risk factors such as fluoroquinolone and corticosteroid usage, which have been shown to increase the risk of any tendon rupture, may not have been found to be significant in this study because only 12 patients in the cohort were exposed to either steroids or fluoroquinolones in the time adjacent to the surgery. 25 Similarly, the limited data on female patients did not allow for a robust subanalysis of sex-based differences and thus may not adequately capture the extent of clinical differences. Another limitation of our study was the lack of reporting of contralateral uninjured leg ROM on postoperative testing. Although the threshold was set low at 110° to mitigate overstating patients identified as having poor outcomes in terms of ROM, this did not allow for a baseline comparison of ROM.
Conclusion
Patient-specific characteristics—such as increasing age, greater BMI, female sex, retinacular involvement, and smoking status—were risk factors for poor outcomes after quadriceps tendon repair. Further studies are needed to identify potentially modifiable risk factors that can be used to set patient expectations and improve outcomes.
Footnotes
Final revision submitted August 11, 2023; accepted August 21, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.K.P. has received a grant from DJO and education payments from Eclipse Technology Solutions, Paladin Technology Solutions, Smith & Nephew, and Mid-Atlantic Surgical Systems. D.W.M. has received education payments from Arthrex and Liberty Surgical and nonconsulting fees from Paladin Technology Solutions. S.B. has received nonconsulting fees from Arthrex and hospitality payments from Wright Medical Technology and Smith & Nephew. K.B.F. has received a grant from Vericel; education payments from Liberty Surgical; consulting fees from Vericel, Innocoll, and Medical Device Business Services; nonconsulting fees from Vericel; and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Philadelphia University and Thomas Jefferson University (ref No. 152).