
Abstract
Background:
Prevention of pitching-related elbow pain in youth baseball players is important. Overhead pitching involves a whole-body motion, including head-neck rotation. A limited range of motion of head-neck rotation may cause inefficient pitching motion; however, this association is unclear.
Purpose:
To determine whether the range of motion of head-neck rotation is associated with the history of pitching-related elbow pain in youth baseball players.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 311 youth baseball players were selected and asked to complete a questionnaire survey about their age, weight, height, sex, baseball experience, main position, pitching side, and previous/current elbow pain during pitching. The range of motion of the upper and lower limb joints, head-neck rotation, and thoracic kyphosis angle were measured. Binomial logistic regression analysis was used to identify factors associated with the history of elbow pain related to pitching.
Results:
There were 101 players with a history of pitching-related elbow pain (history group) and 142 players with no pitching-related elbow pain (no-history group). The history group had significantly lower values than the no-history group regarding the range of motion of head-neck rotation on the nondominant side (74.9°± 9° vs 77.7°± 9.6°; P = .02) and overall head-neck rotation (150.6°± 14.7° vs 154.9°± 18.4°; P = .04). Binomial logistic regression analysis identified head-neck rotation on the nondominant side (odds ratio [OR], 0.97 [95% CI, 0.94-1.00]), shoulder horizontal adduction on the dominant side (OR, 0.98 [95% CI, 0.96-1.00]), height (OR, 1.04 [95% CI, 1.00-1.08]), and playing position (pitcher) (OR, 0.40 [95% CI, 0.21-0.76]) as factors associated with a history of pitching-related elbow pain.
Conclusion:
Our cross-sectional analysis demonstrated that youth baseball players with a history of pitching-related elbow pain had limited head-neck rotation range of motion on the nondominant side, and this was a significant factor associated with the history of pitching-related elbow pain.
Baseball pitchers are at high risk of developing pitching injuries. Andrews and Fleisig 1 reported that approximately one-fourth of pitchers aged 9 to 12 years have elbow pain when pitching. Pitching injuries in youth baseball players can lead to further pain and disability in the future, making it an ideal time to prevent further pitching-related injuries. The risk factors for shoulder and elbow pain in baseball pitchers fall into 2 categories—modifiable and nonmodifiable. 20 The nonmodifiable risk factors include age, height, and years of pitching experience.12,15 Sakata et al 17 described modifiable risk factors as 100 pitches per day, pitcher position, elbow extension deficit, and thoracic kyphosis angle. These authors also reported that age, total playing experience, number of practice days per week, shoulder joint rotation on the dominant side, and passive hip internal rotation (IR) range of motion (ROM) on the nondominant side were associated with pitching injuries. 17
The baseball pitching motion consists of a kinetic chain that requires great coordination, starting with an elevation of the lower limb and moving to the trunk and upper limb. During the wind-up phase of the pitching motion, the neck rotates to the nonpitching side, influenced by the anterior scalene, sternocleidomastoid, levator scapulae, and trapezius muscles. Young et al 23 reported that the neck is associated with pitching disorders in athletes who practice overhead motions, and we postulate that tightness of the aforementioned muscles limits the rotation of the head and neck and thus affects the pitching motion. Hiramoto et al 8 identified that high school baseball players had a characteristic head-neck rotation difference between the dominant and nondominant side. A study on college baseball players found that results on the cervical flexion-rotation test were significantly lower in those with a pitching injury than in those with no injuries. 5
The results of these studies indicate that head and neck rotation is a risk factor for pitching injuries. Failure to perform proper cervical spine movement during pitching may result in compensatory movements, such as early trunk rotation and excessive lateral placement of the striding leg. Early initiation of trunk rotation may increase tensile forces on shoulder and elbow ligament structures. 3 Adequate cervical rotation during the pitching motion could be important in preventing baseball-related injuries. However, no studies to date have examined the relationship between the ROM of head-neck rotation and the history of pitching injuries in youth baseball players.
This study compared player characteristics and joint measurements and examined factors associated with a history of elbow pain during pitching. It was hypothesized that a decreased head-neck rotation ROM would be one of the causes of a history of pitching-related elbow pain.
Methods
Design and Participants
A cross-sectional study was conducted annually between February 14, 2016, and December 15, 2019. A total of 60 baseball teams registered in a junior baseball association in the city of Sagamihara were invited to participate, and 311 players (age, 6-12 years; 283 men and 28 women players) agreed to participate. The inclusion criteria were baseball players (pitchers and fielders) aged 9 to 12 years. Fielders were included, as they may have had previous pitching experience. The exclusion criteria were pain during the pitching motion and a history of elbow joint surgery. Before participation, written informed consent was obtained from all legal guardians. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol received ethics committee approval.
All participants underwent physical examinations by an orthopaedics doctor (Y.K.) and a physical therapist (M.K.) with >10 years of experience, and background information was gathered using a preliminary questionnaire—available separately as Supplementary Material. Questionnaires were distributed to the parents and coaches of the team to collect personal data before the physical assessment. The items in the preliminary questionnaire included grade in school, age, weight, height, sex, main playing position, baseball experience, pitching side, and history of or current elbow pain during pitching (phrased in the questionnaire as “Have you ever had elbow pain when pitching before the day of the medical examination?”). Based on the responses to the questionnaire, the participants were classified into 2 groups: those with a history of pitching-related elbow pain (history group) and those without a history of pitching-related elbow pain (no-history group).
Physical Measurements Related to Pitching
All participants underwent bilateral passive ROM measurements by 2 physical therapists (Y.S. and N.S.) for shoulder external rotation (ER), shoulder horizontal adduction, forearm supination, hip IR, and head-neck rotation in the upright position. In addition, the hip-buttock distance was measured. Shoulder ER at 90° of abduction was measured in the supine position with the elbow at 90° of flexion and the forearm in a neutral rotation (Figure 1A). The examiner fixed the scapula to prevent movement. Shoulder horizontal adduction was measured with the upper limb adducted across the body, starting at 90° of abduction in the supine position. 9 The examiner fixed the lateral border of the scapula to prevent movement. The humerus angle against a line perpendicular to both acromions was measured 1 time using a goniometer (Figure 1B). Forearm supination was measured in a sitting position with the bilateral examination of the pen, with the shoulder at 0° of abduction, elbow at 90° of flexion, and forearm at neutral rotation. At maximal supination, the angle of the pen against a vertical line was measured by a goniometer (Figure 1C). Hip IR and hip-buttock distance were measured in the prone position with the knee at 90° of flexion. For hip IR of the hip, the angle of the lower leg against a vertical line was measured using a goniometer (Figure 1D). To measure the hip-buttock distance, the examiner pushed the distal part of the lower leg toward the buttock to examine the anterior thigh muscle resistance. The distance between the heel and buttock was measured by the examiner’s ruler (Figure 1E).
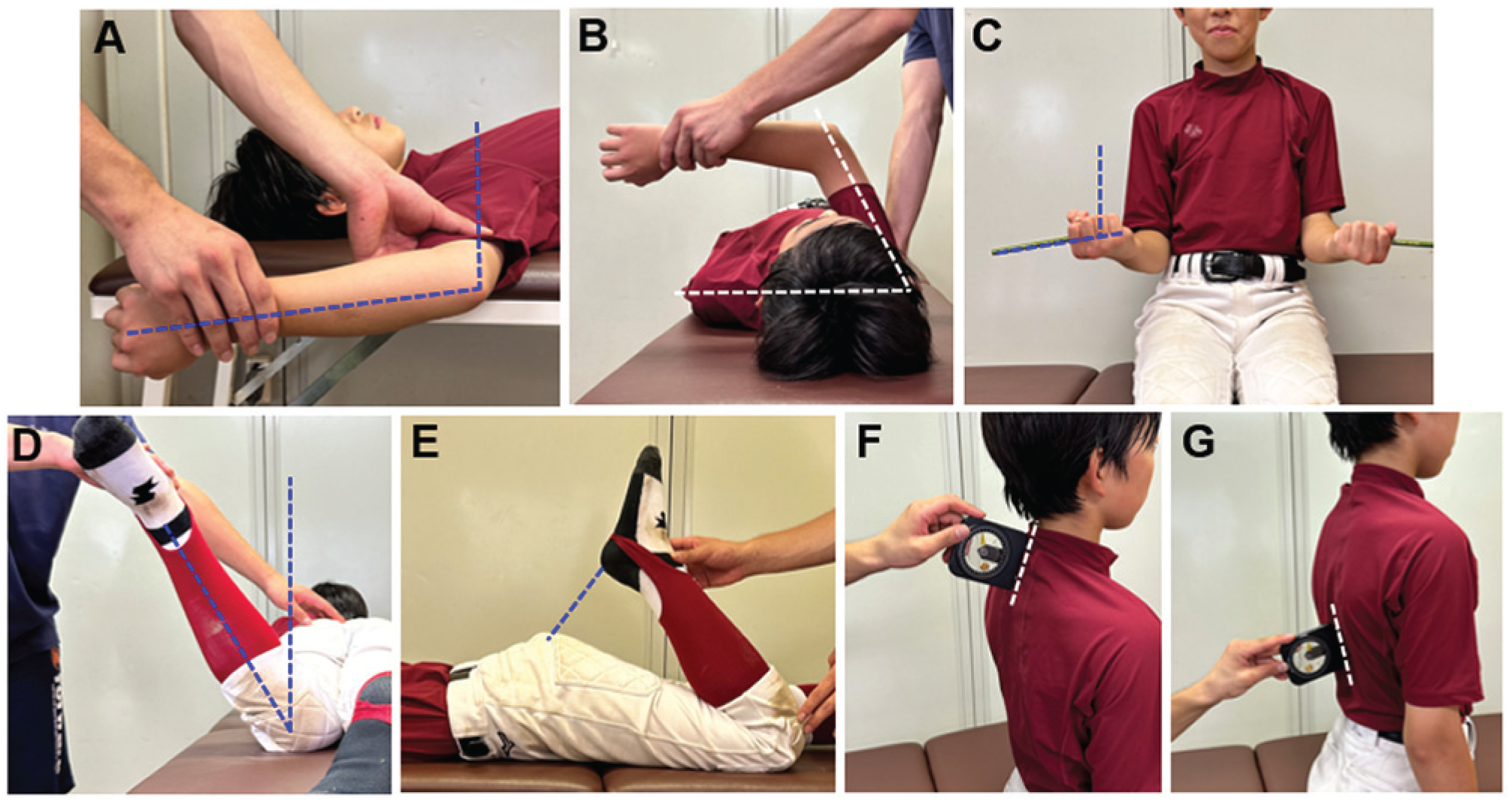
Measurements of (A) shoulder external rotation, (B) shoulder horizontal adduction, (C) forearm supination, (D) hip internal rotation, (E) hip-buttock distance, (F) angle of thoracic kyphosis between the spinous processes of the first and second thoracic spines and (G) between the 12th thoracic and 1st lumbar vertebrae. Blue and white dashed lines indicate representative angles or distances measured.
A single physical therapist (C.I.) measured the thoracic kyphosis angle using an inclinometer. The examiner placed the inclinometer between the spinous processes of the first and second thoracic spines (Figure 1F) and between the 12th thoracic and 1st lumbar vertebrae (Figure 1G) in a relaxed standing position. 17 The angle of thoracic kyphosis was summated by these angles. 14 The intratester and intertester reliability of this measurement has been reported10,11 as excellent (intraclass correlation coefficient [ICC], 0.95).
Bilateral passive ROM of head-neck rotation was measured by 3 physical therapists (M.A., T.M., and others) acting in conjunction using a standard goniometer (Figure 2). The ROM on the dominant side and the nondominant side were measured in succession, without repositioning, to not move the pelvis. While 1 examiner (M.A.) fixed the bilateral shoulder to prevent upper trunk movement, another examiner (T.M.) measured the head-neck axial rotation angle based on the nose position change from the top of the head. The third examiner watched the compensatory neck motion by lateral neck flexion. The ROM values for head-neck rotation on both sides were measured once, and the overall head-neck ROM was considered the sum of these angles. In a preliminary experiment involving 13 healthy adults, the intratester reliability of this measurement method was excellent (ICC, 0.85 [95% CI, 0.60-0.95]), although the intertester reliability was moderate (ICC, 0.65 [95% CI, 0.08-0.89]). The standard errors for intratester reliability for this measurement were 1.4° and 1.1° for the first and second tests, respectively, and those for intertester reliability were 1.4° and 1.6° for the first and second examiners, respectively.

Measuring the bilateral passive range of motion of head-neck rotation using a standard goniometer.
Statistical Analyses
Continuous variables were reported as means ± standard deviations (SD). Univariate analyses were conducted to compare the history and no-history groups using the chi-square test for the position (pitcher or fielder) and the independent t test for continuous variables. Factors related to the history of pitching pain were analyzed using binomial logistic regression models. A model was created with a history of pitching-related elbow pain as the outcome variable. The independent variables were head-neck rotation ROM on the nondominant side, participant characteristics (height, baseball experience, and playing position), and pitching-related measurements (hip IR on the nondominant side, shoulder horizontal adduction on the dominant side, and thoracic kyphosis angle). The participant characteristics and pitching-related measurements were extracted from variable and invariant risk factors for pitching injury reported in previous studies.12,15,17 The model was created using the forced entry method. The number of independent variables (n = 7 items) was judged to be sufficient for the sample size (n = 243) with reference to Peduzzi et al. 16 SPSS Statistics Version 27.0 (IBM) was used to perform all analyses. The significance level was set at P < .05 in all analyses.
Results
Of 311 initial players, 68 players were excluded because of measurement errors or being underage (6-8 years). Thus, 243 players (101 in the history group and 142 in the no-history group) completed all measurements in the study. The characteristics of both study groups are shown in Table 1. The history group was significantly taller (P = .04) and had a greater proportion of pitchers (P = .01) than the no-history group. In addition, the ROM of the head-neck rotation on the nondominant side and overall head-neck rotation for players with a history of elbow pain were significantly lower than those without a history of elbow pain (Tables 2 and 3).
Descriptive Data of the Study Groups a

Data are reported as mean ± SD unless otherwise indicated. Dashes indicate areas not applicable. Bold P values indicate statistically significant differences between groups (P < .05). ES, effect size.
Cohen d.
Comparison of Pitching-Related Measurements on Each Side According to Study Group a

Data are reported as mean ± SD. The bold P value indicates a statistically significant difference between groups (P < .05). ER, external rotation; ES, effect size; IR, internal rotation.
Cohen d.
Comparison of Thoracic and Head-Neck Measurements According to Study Group a

Data are reported as mean ± SD. The bold P value indicates a statistically significant difference between groups (P < .05). ES, effect size.
Cohen d.
Binomial logistic regression analysis identified 2 nonmodifiable factors (greater height and pitching position) and 2 modifiable factors (lower head-neck rotation ROM on the nondominant side and shoulder horizontal adduction on the dominant side) associated with a history of pitching-related elbow pain (Table 4). The Hosmer-Lemeshow test results of this model indicated goodness of fit at P = .09, with a percentage of correct classifications of 62.1%.
Independent Factors Associated With History of Pitching Pain a
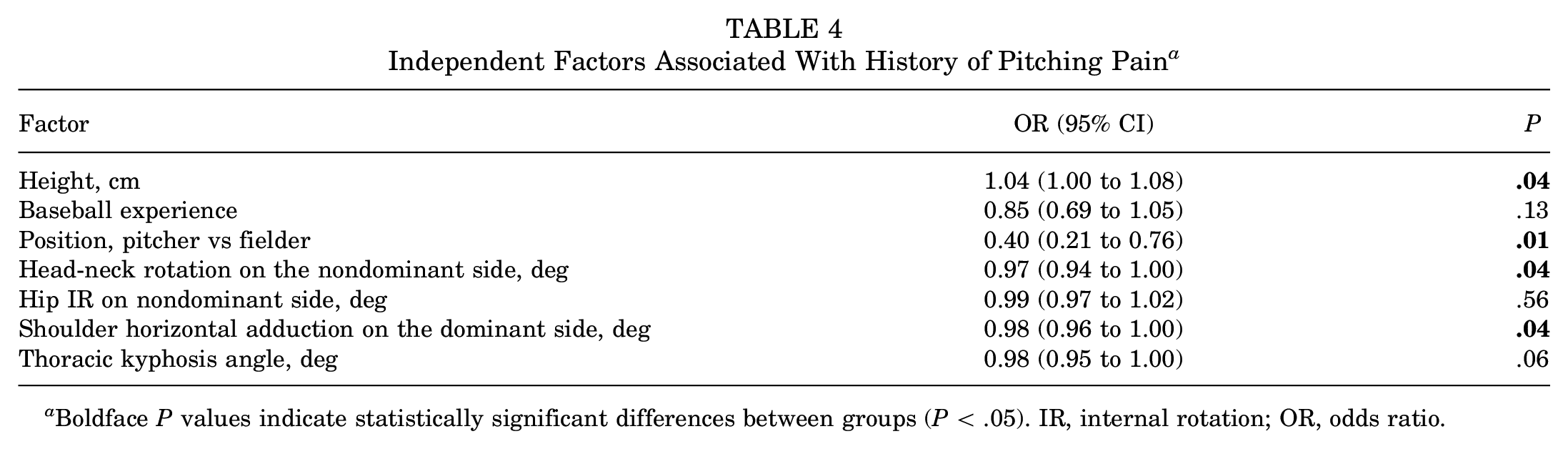
Boldface P values indicate statistically significant differences between groups (P < .05). IR, internal rotation; OR, odds ratio.
Discussion
The most important findings of the present study were as follows: (1) players with a history of pitching-related elbow pain had significantly lower values than those without a history of pitching-related elbow pain regarding head-neck rotation ROM on the nondominant side (74.9°± 9° vs 77.7°± 9.6°; P = .02) and overall head-neck rotation ROM (150.6°± 14.7° vs 154.9°± 18.4°; P = .04), and (2) head-neck rotation ROM on the nondominant side was identified as a risk factor for history of pitching-related elbow pain in youth baseball players (OR, 0.97 [95% CI, 0.94-1]).
Nonmodifiable Risk Factors
In the present study, compared with the no-history group, the history group was taller and had a greater proportion of pitchers, which is consistent with the outcomes of several previous studies.12,15,24 Lyman et al 12 reported that the number of pitches is associated with pitching pain, and Yukutake et al 24 listed height as a risk factor for pitching disability in Little League players. Olsen et al 15 indicated that increased height and weight are risk factors for pitching disorders, especially in youth baseball players with a good physique who tend to be overworked as pitchers, leading to excessive pitching and overuse. Therefore, nonmodifiable risk factors, such as height and pitching experience, must be considered in preventing pitching injuries in youth baseball players. Specific measures include limiting the number of pitches thrown and ensuring that multiple players on the team are trained as pitchers.
Modifiable Risk Factors
The study findings indicated that nondominant side and overall head-neck rotation were novel factors associated with the history of elbow pain; specifically, head-neck rotation was significantly lower in players with a history of pitching pain compared with those without (150.6°± 14.7° vs 154.9°± 18.4°; P = .04). While the difference between groups in the rotation angle was not large, the values were outside the standard error of the measurement of head-neck rotational ROM and, therefore, we consider these results to be meaningful. The limited ROM of head-neck rotation may be attributed to the tightness of the muscles attached to the scapula and clavicle, such as the trapezius, sternocleidomastoid, and anterior scalene muscles. We may speculate that tightness of these muscles can restrict the movement of the upper limbs from the scapula, which may be related to the history of elbow pain during pitching. Some studies have examined limb mobility and muscle strength while maintaining static spinal posture to investigate modifiable risk factors for pitching-related elbow pain.7,17 Despite well-established methods for measuring cervical rotation ROM,4,22 only a few studies have considered spinal column ROM during baseball-related physical examinations.5,8 A strength of the present study was that 3 examiners cooperated to measure each participant to minimize the compensatory motion of the trunk axis rotation. Further, angles were measured to the nearest 1° to minimize error. Thus, our data on head-neck rotation provide new insight into the factors related to pitching disabilities.
Risk Factors for Pitching-Related Elbow Pain
In the present study, 2 nonmodifiable and 2 modifiable factors were related to the history of pitching-related elbow pain. These factors are reasonable, and, importantly, modifiable factors can be manipulated to reduce risk, whereas this is not the case for nonmodifiable factors. In particular, the previously unreported head-neck rotation should be noted. Participants with limited head-neck rotation ROM on the nondominant side were approximately 10% more likely to have a history of elbow pain during pitching. Therefore, this factor should not be ignored, because neck rotation plays a very important role in pitching motion. The pitching motion consists of a whole-body kinetic chain using a rotational motion in the pitching direction. The efficient transfer of power from the lower limbs to the trunk and upper limbs is an important condition for efficient performance. However, Davis et al 3 reported that premature trunk rotation during the pitching phase increases elbow valgus moment and creates a risk factor for pitching-related disorders. Restricting the head-neck rotation may lead to the early rotation of the trunk toward the catcher because of short spinal axial rotation.
Interestingly, limited ROM of shoulder horizontal adduction was also found to be a risk factor for the history of pitching-related elbow pain. The limited ROM of head-neck rotation may be related to the limited ROM of shoulder horizontal adduction, causing posterior tightness of the shoulder. Early rotation of the trunk toward the catcher during pitching may induce early completion of trunk rotation, resulting in an upper limb–dependent pitching motion. Fleisig et al 6 reported that the shoulder joint was under greater traction than the body weight during the ball-release phase. This traction force is braked by the posterior component of the shoulder, which increases the tightness of the posterior component of the shoulder in baseball players. We selected ROM of shoulder horizontal adduction as an indicator of posterior shoulder tightness 21 according to the methods of Laudner et al. 9 Shanley et al 18 reported that a decrease in shoulder horizontal adduction ROM is a cause of pitching disability in youth baseball players. Thus, although there is a general consensus that posterior tightness is associated with shoulder and elbow disorders,2,13,19 additional risk factors for pitching-related injuries, such as head and neck rotation, should be discussed in future.
Limitations
This study has some limitations. First, establishing a causal relationship for the history of pitching pain was impossible because of the cross-sectional study design. Second, although the measurement methods were standardized, the participants in this study (pitchers and fielders) ranged in age from 9 to 12 years; thus, differences in developmental growth during this period may have affected the study outcomes. Third, a history of pitching pain was judged by a self-reported questionnaire. Last, this study did not clarify the relationship between head-neck rotation limitation and pitching kinematics; thus, this association should be examined in future research.
Conclusion
The findings of this study indicated that youth baseball players with a history of pitching-related elbow pain had less head-neck rotation ROM on the nondominant side when compared with players with no such history, and head-neck rotation ROM on the nondominant side was associated with a history of elbow pain.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241229079 – Supplemental material for Association of Head-Neck Rotation With History of Pitching-Related Elbow Pain in Youth Baseball Players
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241229079 for Association of Head-Neck Rotation With History of Pitching-Related Elbow Pain in Youth Baseball Players by Masumi Yoshimoto, Masashi Kawabata, Toru Miyata, Yosuke Sato, Daichi Naoi, Mitsuaki Ashihara, Nobuyuki Suzuki, Chihiro Ikoma, Hiroaki Tatsuki, Ryota Kuratsubo, Hiroyuki Watanabe, Yohei Kusaba and Daiki Watanabe in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
Final revision submitted June 11, 2023; accepted August 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the Japan Society for the Promotion of Science Grant-in-aid for Research Activity Start-up (JSPS KAKENHI, grant JP21K21228). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sagamihara Kyodo Hospital (ref No. 198).
Authors
Masumi Yoshimoto, PT, PhD (Department of Physical Therapy, Faculty of Health and Medical Science, Teikyo Heisei University, Tokyo, Japan); Masashi Kawabata, PT, PhD (Department of Rehabilitation, School of Allied Health Sciences, Kitasato University, Sagamihara, Japan; Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan; Department of Rehabilitation, School of Allied Health Sciences, Kitasato University, 1-15-1 Kitazato, Minami-ku, Sagamihara, Kanagawa 252-0373, Japan); Toru Miyata, PT, MS (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Yosuke Sato, PT (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Daichi Naoi, PT (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Mitsuaki Ashihara, PT, MS (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Nobuyuki Suzuki, PT (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Chihiro Ikoma, PT (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Hiroaki Tatsuki, PT (Department of Rehabilitation, Sagamihara Kyodo Hospital, Sagamihara, Japan); Ryota Kuratsubo, PT, MS (Department of Rehabilitation, Kitasato Institute Hospital, Kitasato University, Tokyo, Japan; Department of Sports Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan); Hiroyuki Watanabe, PT, PhD (Department of Rehabilitation, School of Allied Health Sciences, Kitasato University, Sagamihara, Japan); Yohei Kusaba, MD (Department of Orthopaedic Surgery, Yokohama City University, Yokohama, Japan; Department of Orthopaedic Surgery, Sagamihara Kyodo Hospital, Sagamihara, Kanagawa, Japan); and Daiki Watanabe, MD (Department of Orthopedic Sports Medicine, Yokohama Minami Kyosai Hospital, Yokohama, Kanagawa, Japan).
Supplemental Material
Supplemental Material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671241229079#supplementary-materials
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.