
Abstract
Background:
Promising short- and midterm outcomes have been seen after anatomic coracoclavicular ligament reconstruction (ACCR) for chronic acromioclavicular joint (ACJ) injuries.
Purpose/Hypothesis:
To evaluate long-term outcomes and shoulder-related athletic ability in patients after ACCR for chronic type 3 and 5 ACJ injuries. It was hypothesized that these patients would maintain significant functional improvement and sufficient shoulder-sport ability at a long-term follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included were 19 patients (mean age, 45.9 ± 11.2 years) who underwent ACCR for type 3 or 5 ACJ injuries between January 2003 and August 2014. Functional outcome measures included the American Shoulder and Elbow Surgeons (ASES), Rowe, Constant-Murley, Simple Shoulder Test (SST), and Single Assessment Numeric Evaluation (SANE) scores as well as the visual analog scale (VAS) for pain, which were collected preoperatively and at the final follow-up. Postoperative shoulder-dependent athletic ability was assessed using the Athletic Shoulder Outcome Scoring System (ASOSS). Shoulder activity level was evaluated using the Shoulder Activity Scale (SAS), while the Subjective Patient Outcome for Return to Sports (SPORTS) score was collected to assess the patients’ ability to return to their preinjury sporting activity.
Results:
The mean follow-up time was 10.1 ± 3.8 years (range, 6.1-18.8 years). Patients achieved significant pre- to postoperative improvements on the ASES (from 54.2 ± 22.6 to 83.5 ± 23.1), Rowe (from 66.6 ± 18.1 to 85.3 ± 19), Constant-Murley (from 64.6 ± 20.9 to 80.2 ± 22.7), SST (from 7.2 ± 3.4 to 10.5 ± 2.7), SANE (from 30.1 ± 23.2 to 83.6 ± 26.3), and VAS pain scores (from 4.7 ± 2.7 to 1.8 ± 2.8) (P < .001 for all), with no significant differences between type 3 and 5 injuries. At the final follow-up, patients achieved an ASOSS of 80.6 ± 32, SAS level of 11.6 ± 5.1, and SPORTS score of 7.3 ± 4.1, with no significant differences between type 3 and 5 injuries. Four patients (21.1%) had postoperative complications.
Conclusion:
Patients undergoing ACCR using free tendon allografts for chronic type 3 and 5 ACJ injuries maintained significant improvements in functional outcomes at the long-term follow-up and achieved favorable postoperative shoulder-sport ability, activity, and return to preinjury sports participation.
Keywords
Multiple surgical techniques have been proposed in the literature to achieve sufficient reduction in the setting of acute and chronic acromioclavicular joint (ACJ) injuries.2,4 As such, anatomic coracoclavicular ligament reconstruction (ACCR) techniques utilize a semitendinosus or peroneus longus allograft to replicate the coracoclavicular ligaments in their anatomic location.5,9,17 Biomechanically, along with other anatomic reconstruction techniques using free tendon grafts, this approach has been shown to be highly effective in restoring native ACJ properties.11,13,14,16,18
More importantly, this technique has been found to achieve high subjective satisfaction rates among patients with a significant reduction in pain levels and improvement in shoulder function in the short- and midterm.10,19,20,28 At a minimum 2-year follow-up, a recent study reported a significant improvement in functional outcomes and sufficient radiographic reduction after ACCR for type 3 and 5 ACJ injuries. 20 Similarly, Cerciello et al 10 found a significant improvement in shoulder function at a mean follow-up of 3.8 years. Interestingly, there was no significant correlation between the improvement of clinical outcomes and maintenance of radiographic ACJ reduction.10,20
Although these short- to midterm clinical data and biomechanical investigations are promising, evidence pertaining to long-term functional outcomes of patients undergoing ACCR using free tendon grafts is scarce. In addition, remaining sports-related impairments after ACCR for chronic ACJ injuries have not yet been investigated. As patients sustaining ACJ injuries usually have a high functional demand and are frequently participating in sports, the evaluation of postoperative sports ability, activity, and return to preinjury level is of great clinical relevance.
This study aimed to evaluate the long-term functional outcomes and athletic ability in shoulder sports of patients undergoing ACCR for the treatment of chronic type 3 and 5 ACJ injuries. It was hypothesized that patients undergoing ACCR would maintain significant functional improvements along with sufficient athletic ability in shoulder sports at a long-term follow-up.
Methods
Patient Selection
After receiving institutional review board approval for the study protocol, we conducted a retrospective chart review on patient data collected prospectively from an institutional shoulder registry based on a single surgeon’s practice (A.D.M.) between January 2003 and August 2014. Included were patients aged ≥18 years with a primary, chronic (time from injury to surgery >3 weeks), 3 type 3 or 5 ACJ injury who underwent an ACCR procedure using a free tendon allograft after failing at least 1 month of nonoperative treatment. Some patients from a previous study 20 conducted at the institution were also included. Patients with revisions, preoperative fractures of the clavicle, type 1, 2, 4, or 6 ACJ injuries, and those who had undergone successful nonoperative management were excluded. Subsequently, patients with a minimum follow-up of <6 years were excluded. Nineteen patients with chronic ACJ injuries were included in the final study analysis (Figure 1) .

Flowchart visualizing the patient population for this study after accounting for the inclusion and exclusion criteria and those lost to follow-up. ACCR, anatomic coracoclavicular ligament reconstruction; ACJ, acromioclavicular joint;.
Surgical Technique
All patients underwent the ACCR procedure using a tendon allograft and interference screw fixation according to a previously described technique. 17 Surgery was performed with the patient in the beach-chair position. After the skin incision, the surrounding soft tissue was dissected to the deltotrapezial fascia using electrocautery. The fascia was elevated off the clavicle by creating full thickness flaps. Two bone tunnels of the same size were drilled into the clavicle at the anatomic locations of the conoid and trapezoid ligament. A 5-mm posteromedial tunnel was drilled approximately 45 mm medial to the ACJ according to the anatomic insertion of the conoid ligament. Subsequently, a second anterolateral 5-mm tunnel was made, positioned 20 to 25 mm lateral to the center of the conoid tunnel, simulating the trapezoid ligament. 17
Grafts were prepared from either semitendinosus or peroneus longus allograft tendons. The graft was passed beneath the coracoid process from medial to lateral during direct visualization using a suture passing device. The 2 limbs of the graft were then crossed before being shuttled through the bone tunnels at the undersurface of the clavicle. For additional augmentation of the ACJ capsule using the anterolateral limb, the posteromedial limb was kept 2 cm shorter. After visual and radiographic confirmation of ACJ reduction, the graft limbs were secured (first medial limb, then lateral limb) using interference screws (5.5 × 8–mm PEEK screw; Arthrex) while maintaining accurate reduction. Interference screws were placed along the anterior aspect of each tunnel, with tension being applied on the graft limb. Graft limbs were then secured to the superior aspect of the clavicle, and the longer limb was used to reinforce the superior and posterior parts of the repaired ACJ capsule. Last, closure of the deltotrapezoidal fascia was performed. 17
Postoperative Rehabilitation
Postoperative management was performed using a shoulder unloader brace (Lerman Shoulder Orthosis; DonJoy) for 6 weeks. This allowed for the unloading of the shoulder to avoid stress being placed on the ACJ reconstruction. Patients were allowed to initiate upright range of motion exercises 2 months after surgery. If the patient was pain-free, strengthening exercises were implemented after 12 weeks, focusing on scapular stabilizers to reduce ACJ loads. Weight training was incorporated within 3 to 5 months, and return to contact athletic activity began as early as 6 months after surgery. 12
Functional Outcomes
Functional outcome measures included the American Shoulder and Elbow Surgeons (ASES), Rowe, Constant-Murley, Simple Shoulder Test (SST), and Single Assessment Numeric Evaluation (SANE) scores as well as the visual analog scale (VAS) for pain. ASES, Rowe, Constant-Murley, SST, SANE, and VAS pain scores were assessed preoperatively by a research assistant or physician assistant during the visit in the outpatient clinic (C.G.D.). At the final follow-up, patients were contacted by the research assistant via phone and scheduled for the postoperative functional assessment in the outpatient clinic, which was performed by a physician assistant. The few patients who could not come to the outpatient clinic in person received a survey via mail—including pictures illustrating the required motions—which was then filled out with the support of a research assistant (C.G.D.).
Shoulder Sports Ability, Activity Level, and Return to Sports
Postoperative shoulder-dependent athletic ability was assessed using the Athletic Shoulder Outcome Scoring System (ASOSS). The ASOSS records the subjective shoulder sports-associated perception of pain, instability, muscular strength and endurance, intensity, and proficiency level, with each category being graduated and compared with the before-injury score, which is defined21,24 as 100%. In addition, the shoulder activity level was evaluated using the Shoulder Activity Scale (SAS) proposed by Brophy et al, 8 which has been shown to have excellent reliability and construct validity in assessing the activity level of patients with shoulder disorders. Last, the Subjective Patient Outcome for Return to Sports (SPORTS) score was collected to evaluate the patients’ ability to return to their preinjury sporting activity after surgery.6,7
Statistical Analysis
Given that this was a retrospective analysis, the availability of data determined the sample size. A power analysis was performed to assess the capability of the sample size to detect a clinically meaningful change in the ASES score from pre- to postoperative. Assuming a standard deviation of 20 points, a sample size of 13 patients would provide a power of 80% to detect a 17-point difference between pre- and postoperative ASES scores at a level of .05.
Descriptive statistics—including means ± standard deviations for continuous variables and frequency and proportion for categorical variables—were calculated to characterize the study groups. Preoperative, postoperative, and delta (change in scores from pre- to postoperative) ASES, SST, Rowe, Constant-Murley, SANE, and VAS pain scores were compared using an independent t test after confirming that the data were normally distributed. Results of inferential analysis are presented as 95% CIs. P < .05 was considered statistically significant. All analyses were performed with Stata statistical software (StataCorp 2017, Stata Statistical Software: Release 15; StataCorp).
Results
The mean age of the 19 study patients was 45.9 ± 11.2 years (range, 22.3-60.9 years), with a mean follow-up of 10.1 ± 3.8 years (range, 6.1-18.8 years). The mean time from injury to surgery was 102 ± 206.8 weeks (range, 5.5-835 weeks). Patient characteristics are shown in Table 1.
Patient Characteristics (N = 19) a

Data are reported as mean ± SD or n (%).
Functional Outcomes
At the final follow-up, a significant improvement was observed in the ASES, Rowe, SST, Constant-Murley, SANE, and VAS pain scores when compared with preoperative scores (P < .001 for all) (Table 2). No significant differences were found in the pre- to postoperative improvements for any of the outcome scores when comparing type 3 and type 5 injuries.
Preoperative to Postoperative Improvement in Outcome Scores a
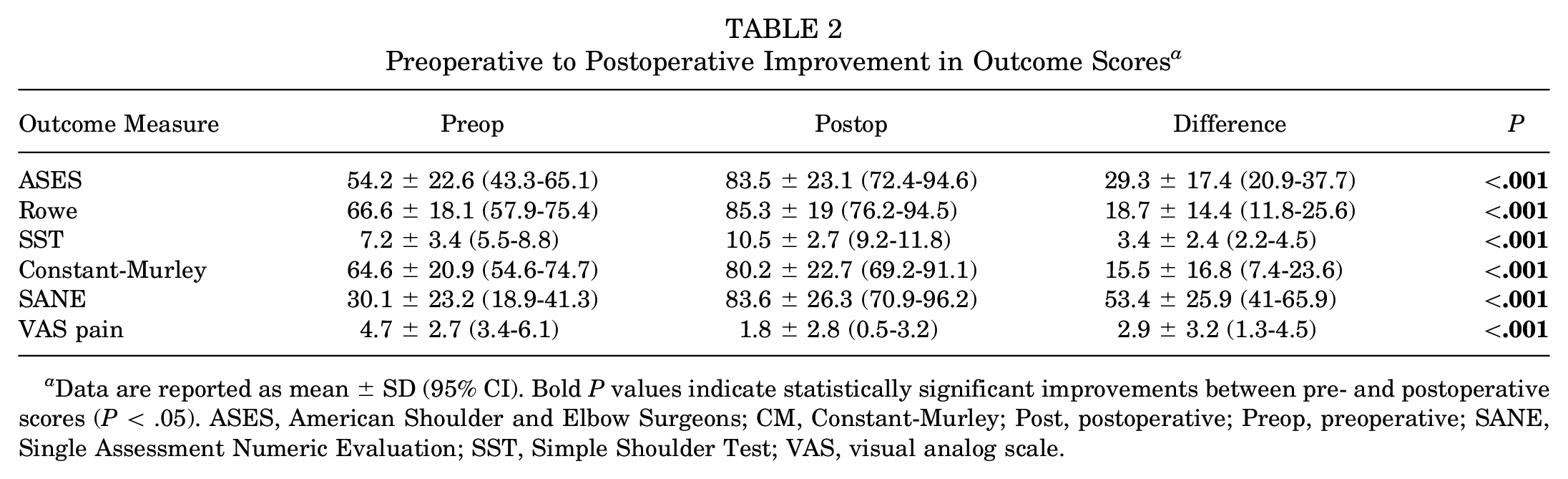
Data are reported as mean ± SD (95% CI). Bold P values indicate statistically significant improvements between pre- and postoperative scores (P < .05). ASES, American Shoulder and Elbow Surgeons; CM, Constant-Murley; Post, postoperative; Preop, preoperative; SANE, Single Assessment Numeric Evaluation; SST, Simple Shoulder Test; VAS, visual analog scale.
Athletic Ability in Shoulder Sports, Activity Level, and Return to Sports
At the final follow-up, patients achieved an ASOSS of 80.6 ± 32, SAS level of 11.6 ± 5.1, and SPORTS score of 7.3 ± 4.1, demonstrating an overall favorable postoperative shoulder sports ability, activity level, and return to their preinjury sports participation. No significant differences were found in the ASOSS, SAS level, and SPORTS scores when comparing type 3 and type 5 injuries (P > .05, respectively).
Complications
Overall, 4 patients (21.1%) were found to have postoperative complications. One patient (5.3%) had a heterotopic ossification around the ACJ, which required debridement and distal clavicle excision for pain. Another patient (5.3%) had a superficial wound infection that resolved with antibiotic treatment. In addition, 1 patient (5.3%) had a distal clavicle fracture due to a direct fall on the shoulder, which needed open reduction and internal fixation. Last, 1 patient (5.3%) had painful ACJ osteoarthritis, requiring distal clavicle excision.
Discussion
The most important finding of the present study was that patients undergoing ACCR for chronic type 3 and 5 ACJ injuries maintained significant improvements in functional outcomes at the long-term follow-up. In addition, patients achieved a favorable postoperative shoulder sports ability, activity, and return to preinjury sports participation. While these long-term findings are consistent with previous studies reporting on clinical short- to midterm outcomes after ACCR using free tendon grafts, ¶ the present study further provides insights pertaining to remaining postoperative impairments during sports participation after ACCR.
A previously published case series of 43 patients who underwent the same ACCR technique for acute and chronic type 3 and 5 ACJ injuries demonstrated similar improvements in shoulder function and maintained radiographic reduction at a mean follow-up of 3.4 years. 20 Similarly, Cerciello et al 10 found a significant functional improvement after ACCR for patients with chronic ACJ injuries at a minimum 1-year follow-up. Both case series showed no correlation between functional outcomes and the maintenance of radiographic reduction, inferred from the postoperative side-to-side difference in the coracoclavicular distance.10,20 As these previous studies were mainly limited to a short follow-up period, the results of the present study highlight the maintained functional improvement in the long term. There was no difference in clinical outcome scores when comparing type 3 and 5 ACJ injuries, which was consistent with the previously reported short- to midterm outcomes of patients undergoing ACCR.10,20
However, recent studies have emphasized the necessity of shoulder sport-specific questionnaires to detect remaining sports-associated limitations after shoulder surgery, as commonly used outcome measures only cover shoulder function during activities of daily living.21,24 This is especially important in the setting of ACJ injuries, as these patients usually have a high functional demand and are frequently engaged in sports. With an ASOSS of 80.6 ± 32, SAS level of 11.6 ± 5.1, and SPORTS score of 7.3 ± 4.1, the present study found an overall favorable postoperative shoulder sports ability, activity level, and return to preinjury sports level.
In the setting of arthroscopically assisted anatomic reconstruction of acute type 5 ACJ injuries using 2 independent suture-button devices, Saier et al 23 reported that all of the 42 patients participated in sporting activities at a mean follow-up of 31 months—although at a significantly reduced intensity and level of competition. Interestingly, no correlation was found between functional outcome scores and return to activity. In a prospective randomized controlled trial, Müller et al 21 compared postoperative sports-related impairments after acute ACJ stabilization using either an open clavicular hook plate or an arthroscopically assisted double double-suture-button technique. 21 The authors found that the anatomic double double-suture-button technique achieved significantly superior sport-specific outcomes compared with the nonanatomic clavicular hook plate at the final 2-year follow-up. More specifically, only athletes who underwent the anatomic procedure returned to a similar sports ability and activity level of the control group of healthy athletes. 21 With an ASOSS of 91.4 ± 10.3, the study by Müller et al 21 showed a higher score for the anatomic double double-suture-button group when compared with patients undergoing the ACCR procedure using a free tendon graft (80.6 ± 32). This may be explained by the longer time from injury to surgery (102 ± 206.8 weeks vs 9 ± 3 days), older age of included patients (45.9 ± 11.2 years vs 34.6 ± 9.4 years), and longer follow-up time (10.1 ± 3.8 years vs 30.8 ± 8.4 months) of patients in the present study. 21
There was an overall postoperative complication rate of 21.1% (4 patients) at the final follow-up in the present study, including 1 patient with a heterotopic ossification around the ACJ, 1 superficial wound infection, 1 distal clavicle fracture due to a direct fall on the shoulder, and 1 patient with symptomatic ACJ osteoarthritis. These findings are comparable with the complication rate of 25.8% observed by Millett et al 19 at a 2-year follow-up. In general, the relatively high complication rate after ACCR in the present cohort may be attributable to the long period of injury to surgery, with a mean of 102 ± 206.8 weeks.
Limitations
There were several limitations to the study. First, although outcomes were collected prospectively, data were reviewed retrospectively, which could create selection bias. Second, the patient population was relatively small. Based on this limitation, intergroup comparisons between type 3 and 5 ACJ injuries may be subject to a statistical type II error. Third, radiographic imaging of the shoulder was not performed at the final follow-up. Consequently, loss of radiographic reduction, as well as the potential presence of iatrogenic fractures, tunnel widening, heterotopic ossifications, osteoarthritis, or osteolysis around the ACJ, could not be evaluated. Fourth, a control group (eg, conservative treatment) was not included to compare the increased benefit of undergoing the ACCR procedure. Although all patients underwent a trial of conservative treatment for at least 1 month, further studies are needed to truly identify whether greater improvement is seen with operative management. Finally, the patient population in the present study was older than the younger athletic population in whom these injuries usually occur,2,4 limiting the external validity and generalizability of the results.
Conclusion
Patients undergoing ACCR using free tendon allografts for chronic type 3 and 5 ACJ injuries maintained significant improvements in functional outcomes at the long-term follow-up. Furthermore, patients achieved a favorable postoperative athletic ability in shoulder sports, activity, and return to preinjury sports participation.
Footnotes
Final revision submitted August 4, 2023; accepted August 21, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from Arthrex by The University of Connecticut Health Center and UConn Musculoskeletal Institute. A.D.M. has received grants from Arthrex; consulting fees from Arthrex and Astellas Pharma; and nonconsulting fees from Arthrex and Kairos Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Connecticut (ref No. 17-066-3).