Abstract
Objectives:
Reduced joint space at the time of joint-preserving hip arthroscopy has been shown to be correlated with rates of eventual conversion to total hip arthroplasty (THA). With an increasingly aging population and increased utilization of hip arthroscopy, it is important to identify factors that may predict early failure and the eventual need for arthroplasty. For some patients, hip arthroscopy may provide symptomatic relief for years, while others garner limited benefit and require conversion THA soon after their index surgery. This study sought to determine if quantitative differences in joint space width (JSW) between the operative and non-operative hip predicted the likelihood of conversion to THA at the time of hip arthroscopy.
Methods:
After obtaining institutional review board approval, a retrospective review identified 105 patients treated for labral tears with arthroscopic hip surgery by a single-surgeon with a minimum of 5- year follow-up. Patients were stratified into cohorts based on whether they received a subsequent THA. Preoperative, anteroposterior pelvic radiographs were obtained for each patient and semi-automated, quantitative JSW measurements were performed at 3 predefined fixed locations per hip (10, 30, and 50 degrees with respect to a polar coordinate system;
Results:
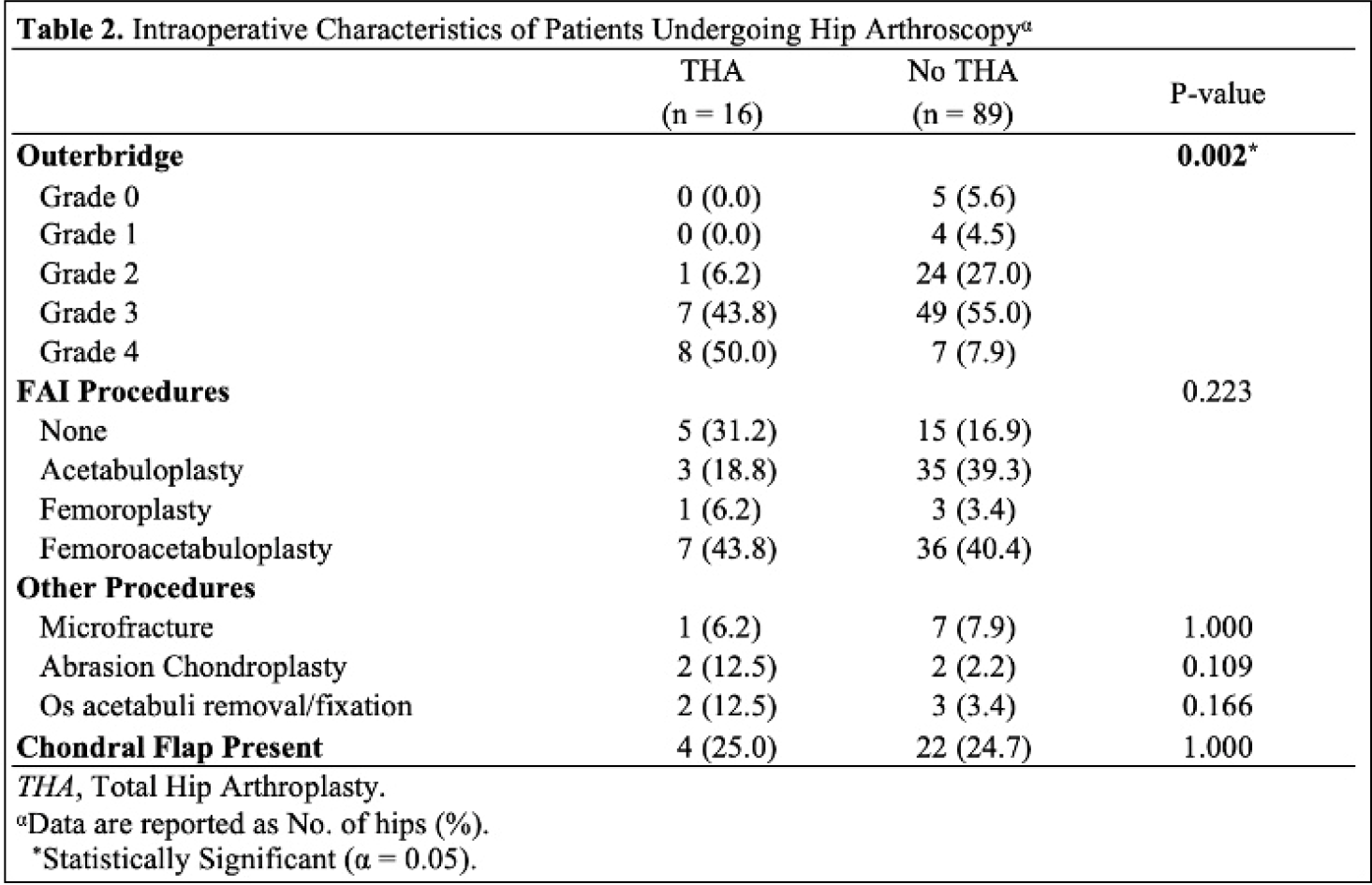
Mean [standard deviation (SD)] follow-up was 8.81 [2.68] years, identifying 16 (15.2%) patients that converted to THA and 89 (84.8%) that did not. When comparing baseline demographic and intraoperative characteristics between cohorts, THA patients were found to have higher mean [SD] age 41.8 [13.4; p=0.003], BMI 29.3 [4.2; p<0.001], Tönnis grade (p<0.001), Outerbridge grade (p=0.002) and higher percentage of males (p=0.014;
Conclusions:
To best educate patients on the risk of THA following hip arthroscopy, identifying objective predictors of early failure is imperative during preoperative evaluation. This study identified that differences in JSW at 30° between the operative and non-operative hip were significantly associated with increased risk of conversion after controlling for demographic and intraoperative factors. Analysis was limited by predetermined locations for JSW and future studies may identify stronger correlations by incorporating additional measurements within the acetabular sourcil. Quantitative differences in JSW comparing the operative hip to the contralateral side predicts patients progressing to THA at the time of hip arthroscopy.