Abstract
Objectives:
Multiple authors have observed that preinjury activity level is a strong predictor of activity level after anterior cruciate ligament (ACL) reconstruction (ACLR.) However, among subjects with a relatively high baseline activity level, predictors for a successful return to preinjury activity level after ACLR remain poorly understood.
Methods:
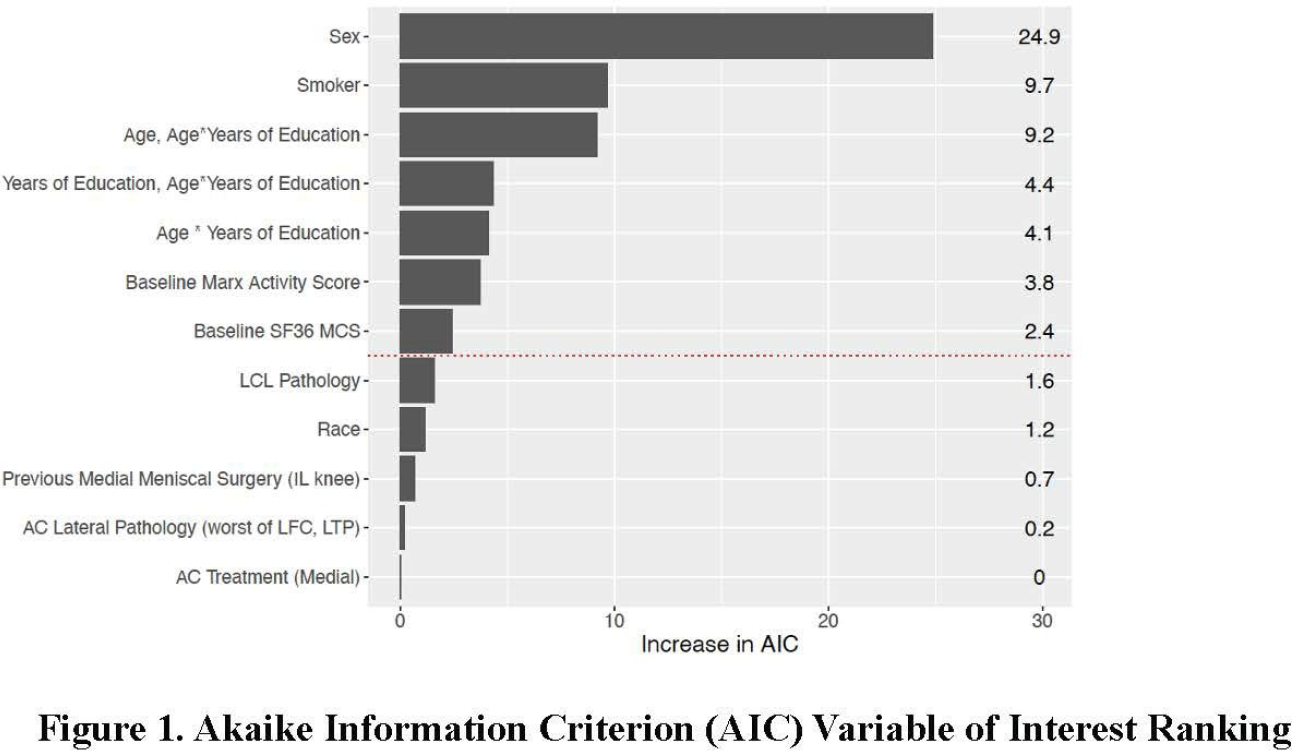
All unilateral ACL reconstructions from 2002-2008 enrolled in the MOON cohort performed in subjects with baseline preinjury Marx activity scores ranging from 12 to 16 were evaluated with specific focus on return to preinjury activity level at 2 years postoperative. Continuous variables such as age, BMI, education level, baseline Short Form-36 mental component survey (MCS), baseline Marx activity were summarized using median and interquartile ranges. Categorical variables such as sex, race, smoking status, reconstruction type (primary/revision), graft type etc. were displayed using counts and percentages. The primary outcome of interest was return to activity, which was defined as a raw difference of ≥ -2 between Marx activity score at 2-year minus baseline Marx activity. This means that anyone who had a ≥ -2 difference in Marx activity was considered returned to activity; otherwise, he/she was not considered able to return to activity. To identify predictors and possible risk factors contributing to return to activity, a multivariable logistic regression model was built. Multivariable modeling was performed to identify risk factors for subjects’ inability to return to baseline, preinjury activity level. The relative importance of each predictor was ranked according to the increase in Akaike information criterion (AIC) upon removal from the full model; the importance rankings are presented in descending order; only positive values are presented in the graphs. AIC quantifies the amount of information explained by the covariates, while penalizing variables for the number of degrees of freedom they use. An AIC-increase 2 indicated that the given variable contributed to a statistically better model.
Results:
There were 1188 patients with 2-year follow up that met the inclusion criteria. The two year follow-up for MARX activity was 82.7 % (1188/1437.) The cohort was comprised of 714 males (60.1%) and 474(39.9%) females. The median age of the cohort was 22 years (25th; 75th interquartile range: 18.0 years; 31.2 years) (Table 1.) Six hundred and forty two (54%) of subjects reported a MARX activity of 16. Overall, 466 (39.2%) subjects were able to return to activity, while 722 subjects (60.7%) were not able to return to activity (Table 2.)
Conclusions:
There are several noteworthy findings of the current study. First, only 39.2% of highly active subjects in this cohort were able to return to same high level of activity at 2 years post ACLR. Second, according to predictive modeling considering all variables of interest, female gender, positive smoking status, lower education level, lower SF-36 MCS, and higher baseline Marx activity scale were all risk factors predictive for the inability to return to preinjury activity level. Furthermore, the interaction between subjects’ age and education level resulted in a variable effect of the likelihood for returning to activity: more highly educated patients at the extremes of age were more likely to return to activity than similarly educated patients in the middle range of ages (22-32 years.) Thus, our hypothesis was only partially proven as the presence of articular cartilage and/or meniscal injuries with or without treatment did not predict a lower likelihood of subjects’ returning to activity nor did a higher baseline, preinjury Marx activity level. In fact, the opposite was true with a lower baseline, preinjury activity level predicting return to activity. To our knowledge, this is the largest cohort comprised of subjects with objectively defined high baseline, preinjury activity level analyzed with multivariable predictive modeling to identify risk factors for an inability to return to high activity at 2 years post ACLR.