
Abstract
Objectives:
Rates of anterior cruciate ligament (ACL) injury in the pediatric population have increased in the last 20 years. While many risk factors have been investigated, to the authors knowledge no study has analyzed the difference in the posterior femoral condyles in patients who have sustained ACL rupture. Therefore, this case control study sought to understand the relationship between the medial and lateral posterior condyles, as well as examining distal femoral version. The authors hypothesized that pediatric patients who suffered ACL rupture will have a relatively larger medial posterior femoral condyle leading to increase structural valgus in flexion.
Methods:
Pediatric patients with a pre-operative knee MRI who underwent ACL reconstruction between February 2016 and June 2020 at a tertiary orthopedic hospital were collected. Cases were matched to controls based on sex, laterality of injury, and age at imaging within 1.5 years. Medial and lateral posterior condylar height was measured for each participant. Condylar difference was calculated as medial posterior condylar height minus lateral posterior condylar height. The distal femoral version was calculated as the angle between the femoral posterior cortical axis and the posterior condylar axis. Mann-Whitney U tests were used to compare continuous variables. Significance was set as a p≤0.05.
Results:
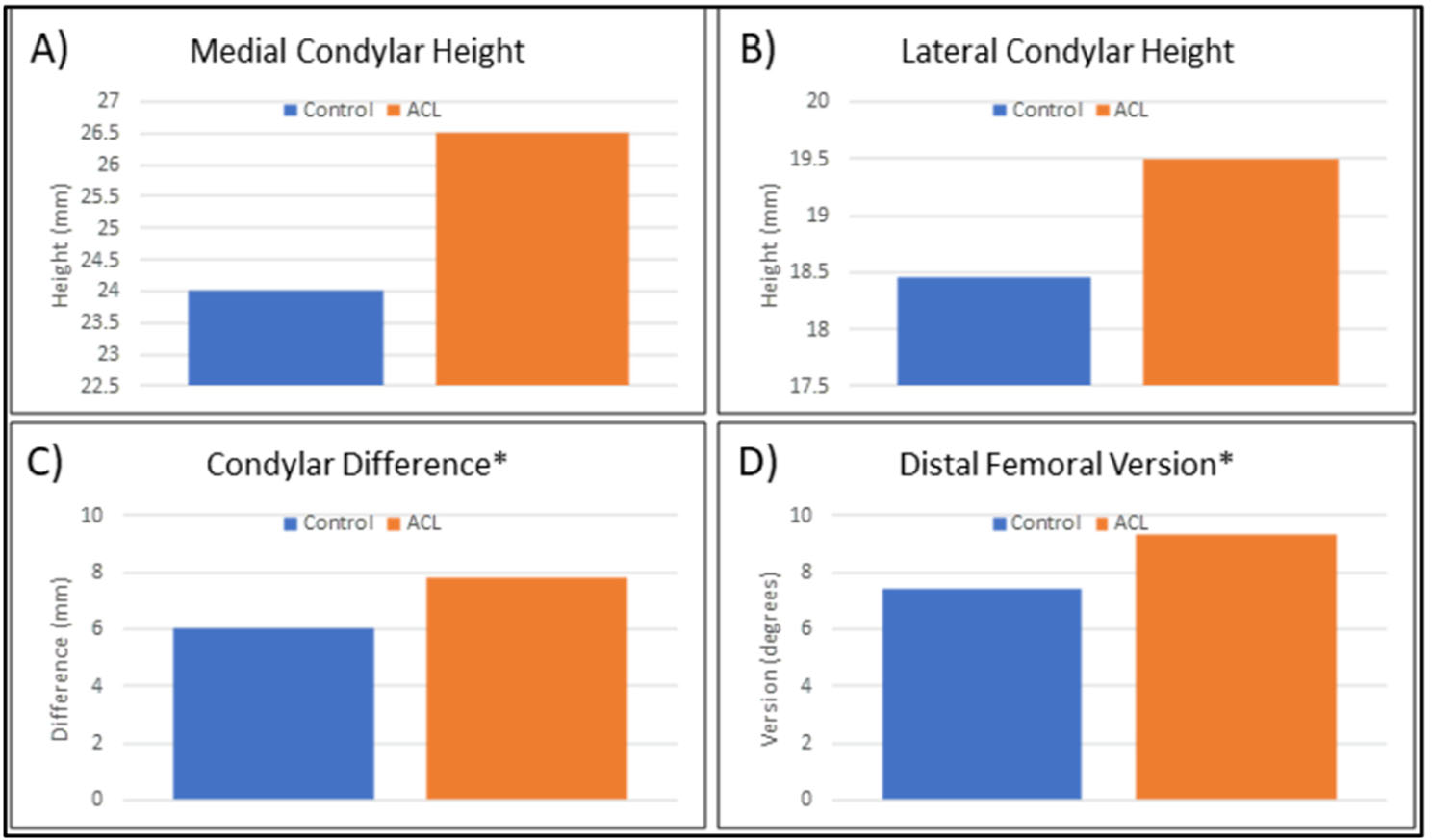
A total of 72 participants were included in this analysis - 36 cases and 36 controls. Median age was 13.5 ± 3.3 years for all participants. Condylar difference was noted to be 1.8 mm greater in cases than controls (p=0.038), while distal femoral version was noted to be 2.0° greater in cases than controls (p=0.025).
Conclusions:
This study demonstrated a significantly greater posterior condylar height difference and distal femoral version among pediatric patients who suffered ACL rupture compared to a matched control group. We speculate that this morphology leads to a relative increase in knee valgus in flexion.
A) Femoral posterior cortical axis (FPCA) shown in red. This is a line along the posterior cortex at the level just proximal to the superior trochlear groove. B) The blue line represents the posterior condylar axis which intersects with the most posterior aspect of the medial and lateral femoral condyle. C) The distal femoral version, shown as 6.1 degrees, was calculated as the angle between the FPCA (red) and the posterior condylar axis (blue). D) the medial (25.2 mm) and lateral (20.2 mm) condylar height was calculated as the perpendicular distance from the FPCA to the midpoint on the condyle that intersects with posterior condylar axis.
Demographic information for ACL cases and controls. Continuous variables are presented as median ± IQR, while categorical variables are presented as n 9%).


A) Medial Posterior Condylar high, B) Lateral Posterior Condylar height, C) Condylar Difference, D) Distal Femoral Version by controls (blue) and ACL cases (orange). Significant differences are denoted with a “*”.