
Abstract
Background:
There is no consensus among sports medicine surgeons in North America on postoperative rehabilitation strategy after meniscus repair. Various meniscal tear types may necessitate a unique range of motion (ROM) and weightbearing rehabilitation protocol.
Purpose:
To assess the current landscape of how sports medicine practitioners in the American Orthopedic Society for Sports Medicine (AOSSM) rehabilitate patients after the repair of varying meniscal tears.
Study Design:
Cross-sectional study.
Methods:
A survey was distributed to 2973 AOSSM members by email. Participants reviewed arthroscopic images and brief patient history from 6 deidentified cases of meniscus repair—in cases 1 to 3, the tears retained hoop integrity (more stable repair), and in cases 4 to 6, the tear patterns represented a loss of hoop integrity. Cases were shuffled before the presentation. For each case, providers were asked at what postoperative time point they would permit (1) partial weightbearing (PWB), (2) full weightbearing (FWB), (3) full ROM, and (4) ROM allowed immediately after surgery.
Results:
In total, 451 surveys were completed (15.2% response). The times to PWB and FWB in cases 1 to 3 (median, 0 and 4 weeks, respectively) were significantly lower than those in cases 4 to 6 (median, 4 and 6 weeks, respectively) (P < .001). In tears with retained hoop integrity, the median time to PWB was immediately after surgery, whereas in tears without hoop integrity, the median time to PWB was at 4 weeks postoperatively. Similarly, the median time to FWB in each tear with retained hoop integrity was 4 weeks after surgery, while it was 6 weeks in each tear without hoop integrity. However, regardless of tear type, most providers (67.1%) allowed 0° to 90° of ROM immediately after surgery and allowed full ROM at 6 weeks. Most providers (83.3%) braced the knee after repair regardless of hoop integrity and utilized synovial rasping/trephination with notch microfracture—a much lower proportion of providers utilized biologic augmentation (9%).
Conclusion:
Sports medicine practitioners in the AOSSM rehabilitated meniscal tears differently based on hoop integrity, with loss of hoop stresses triggering a more conservative approach. A majority braced and utilized in situ adjuncts for biological healing, while a minority added extrinsic biologics.
The meniscus plays a key role in protecting the knee joint and preserving the articular cartilage through load distribution, shock absorption, and lubrication.5,10,31 Loss of meniscal tissue via injury or meniscectomy can lead to altered joint kinematics that increases local tibiofemoral contact forces, resulting in early degenerative changes.14,30,36 Alongside improved operative instrumentation and surgical techniques, meniscus repair has increased in popularity relative to meniscectomy, with the hope of preserved joint mechanics and prevention of secondary osteoarthritis.1,12,17,42 From 2005 to 2011, meniscus repair incidence doubled, while meniscectomy incidence remained stable. 1 Newer studies have demonstrated excellent functional outcomes and suggest decreased rates of osteoarthritis after meniscus repair compared with meniscectomy.21,30,37
Long-term repair outcomes after meniscus repair depend not only on injury pattern, patient characteristics, intraoperative repair technique, but also on diligent adherence to postoperative rehabilitation protocols.27,41 Patient-specific adaptations to rehabilitation protocols may be important, as different tear morphologies have unique biomechanical considerations across repair sites, each possibly necessitating a tailored range of motion (ROM) and weightbearing protocol. 34 For example, repair of longitudinal and bucket handle tears may benefit from early weightbearing and unrestricted passive ROM due to hoop stresses from axial loading in extension that compress the repair site.25,27,33 On the other hand, radial or meniscus root tears representing complete disruptions of the longitudinal hoop integrity may warrant more conservative weightbearing and ROM progression due to the risk for otherwise additional hoop stresses causing distraction across the repair site.27,33,42 Thus, efforts to elucidate the optimal postoperative rehabilitation for each tear type are of significant importance.
There is no consensus on postoperative rehabilitation strategy after meniscus repair among sports medicine practitioners in the United States, particularly with the advent of accelerated rehabilitation protocols.6,20,24 While previous systematic reviews have examined meniscus repair rehabilitation protocols and correlated them with outcomes, 27 there is a paucity of studies with level 1 evidence to enforce the adoption of any specific meniscus repair rehabilitation protocol. In the absence of higher-level data, surveying current practice trends among sports medicine practitioners would be of value in order to understand the collective expertise on how rehabilitation restrictions should be applied to various tear types.
This study aimed to survey the current contextual landscape of how sports medicine practitioners who were members of the American Orthopedic Society for Sports Medicine (AOSSM) recommend rehabilitating patients after repair by tear type. The secondary purpose of this study was to survey the use of perioperative meniscus repair adjuncts, such as biologics and bracing. We hypothesized that practitioners would tend to rehabilitate meniscus repairs differently based on tear morphology, with loss of hoop integrity (such as complete radial or root tears) warranting delayed weightbearing and ROM.
Methods
Study Design
This cross-sectional survey-based observational study disseminated to a single cohort of 2973 members of the AOSSM member directory, which included orthopaedic surgeons, sports medicine physicians, and physical therapists. Institutional review board exemption was obtained before survey distribution. Surveys were distributed 3 times in the third quarter of 2021 via email with a description of the study background, the purpose of the survey, and instructions for completion. All survey responses were obtained anonymously and did not contain any identifiers.
Survey Design
The survey was administered via the institutional Research Electronic Data Capture (RedCap) website. A copy of the survey is available separately as Supplemental Material. The survey detailed 6 cases of isolated meniscus repair, each presented with a brief patient history appropriately indicated for meniscus repair and arthroscopic images displaying the meniscal tear before and after repair (Figure 1). The 6 cases were as follows: (1) medial meniscus red-zone longitudinal peripheral tear; (2) medial meniscus red-white zone bucket-handle tear; (3) lateral meniscus horizontal tear; (4) lateral meniscus radial tear at midbody anterior horn junction; (5) medial meniscus posterior root tear; and (6) lateral meniscus complete radial tear at popliteal hiatus. These 6 tear types were chosen for their representation of the spectrum of injury in meniscal tear types, with sufficient variety in tear patterns involving both medial and lateral menisci and patterns that demonstrate both intact and loss of hoop integrity. For instance, tears 1 to 3 retained hoop integrity (more stable repair), while tears 4 to 6 did not (less stable repair). The order of these 6 cases was shuffled in the distributed version of the survey to minimize anchoring bias in the participants’ response selections.

The arthroscopic images used for the 6 meniscal tear cases in the survey. Cases were grouped randomly according to tears that retained hoop integrity as follows: (1) medial meniscus red-zone longitudinal peripheral tear; (2) medial meniscus red-white zone bucket-handle tear; and (3) lateral meniscus horizontal tear; and tears that showed loss of hoop integrity as follows: (4) lateral meniscus radial tear at mid-body anterior horn junction; (5) medial meniscus posterior root tear; and (6) lateral meniscus complete radial tear at popliteal hiatus.
For each case, 4 questions were asked, designed to elicit responses for (1) time until permitted partial weightbearing (PWB); (2) time until permitted full weightbearing (FWB); (3) time until permitted full ROM; and (4) permitted ROM immediately after surgery. Exacting terminology for PWB restrictions—such as by percentage, weight, or toe-touch/touchdown/flat-foot weightbearing—was avoided to maintain survey generalizability.
Secondarily captured were the demographic characteristics of the study respondents, including primary academic/professional degree, years in practice, practice type, location of practice, and sports medicine board certification. Routine use of meniscus repair adjuncts—including bracing and biologics (synovial rasping or trephination, notch microfracture, classic fibrin clot, platelet-rich plasma, bone marrow aspirate concentrate)—was also obtained within the survey.
Data Analysis
Responses were collected in RedCap, and output tables were exported into Microsoft Excel (Microsoft) and Stata 16 statistical software (Stata). Descriptive statistics of the categorical data were displayed as proportions and percentages, while those for ordinal data were expressed as medians and interquartile ranges (IQRs). Response distributions were then compared between cases 1 to 3 (retained hoop integrity) and cases 4 to 6 (lost hoop integrity) using either the Mann-Whitney U test or chi-square test. Statistical significance was set at P < .05. A consensus rehabilitation recommendation was said to be achieved if there was >50% agreement among the respondents in their response to a particular question.
Results
Respondent Demographic Characteristics
After 3 solicitations for responses, 451 completed surveys were collected, representing a 15.2% response rate. Respondent demographic characteristics are detailed in Table 1. Most responses (96.4%) were obtained from physicians and orthopaedic surgeons, with varied practice types and years of experience. Nonsurgeon and non–board certified responses were included with equal weighting in the data analysis, since nonsurgeon practitioners also treat meniscal tears on a consistent basis, and/or may perform academic research relevant to meniscal biomechanics, and thus may contribute equally to our understanding of appropriate meniscus repair rehabilitation. Figures 2A, 2B, and 2C display the cumulative distribution of postoperative time to permissive PWB, FWB, and full ROM, respectively, and Figure 3 represents the distribution of ROM permitted immediately after surgery.
Respondent Demographic Characteristics (N = 451) a

Data are reported as n (%). DO, doctor of osteopathic medicine; DPT, doctor of physical therapy FRCSC, fellow of the Royal College of Surgeons of Canada; MBBS, bachelor of medicine and bachelor of surgery; MD, medical doctor; PA-C, certified physician assistant; PhD, doctor of philosophy.

Cumulative distribution (in %) of time to permitted (A) partial weightbearing, (B) full weightbearing, and (C) full range of motion.
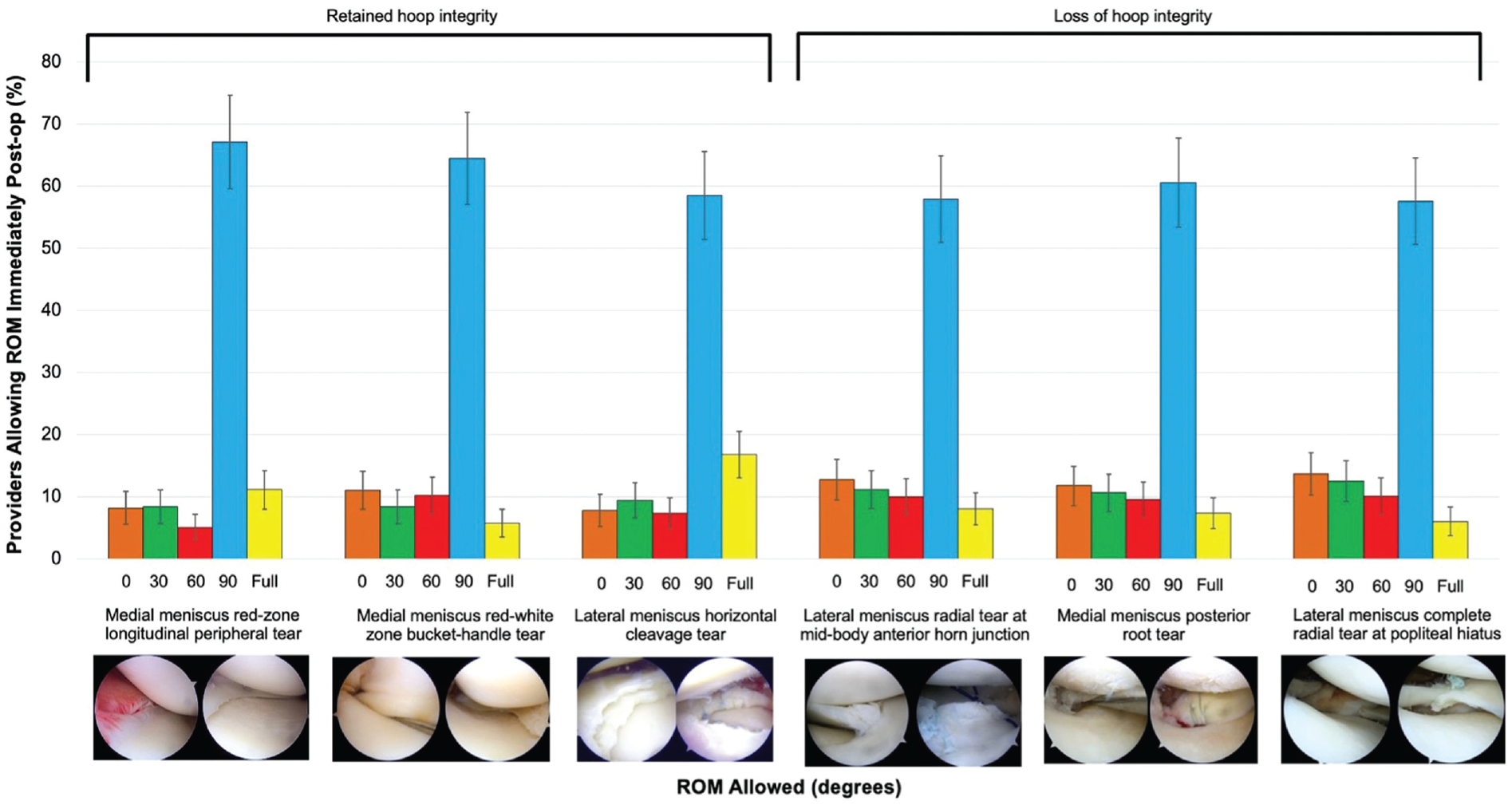
Distribution of range of motion permitted immediately after surgery.
Cases 1 to 3: Tears That Retained Hoop Integrity
Case 1: Medial Meniscus Red-Zone Longitudinal Peripheral Tear
Regarding case 1, most providers (64.4%) permitted PWB immediately after surgery. However, there was variation in the time to permitted FWB, with the most common being 6 weeks (33%), followed by immediately (31.7%), and 4 weeks after surgery (22.2%) (median, 4 weeks; IQR, 0-6 weeks). With regard to ROM, most providers (52.7%) permitted full ROM at 6 weeks after surgery (median, 6 weeks; IQR, 4-6 weeks). Finally, most providers (67.1%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 90°-90°).
Case 2: Medial Meniscus Red-White Zone Bucket-Handle Tear
Similarly, for case 2, most providers (55.2%) permitted PWB immediately after surgery (median, 0 weeks; IQR, 0-4 weeks). With regard to time to FWB, 6 weeks was the most popular (42.6%), followed by immediately (25.9%), and 4 weeks after surgery (17.6%) (median, 4 weeks; IQR, 0-6 weeks). In addition, most providers (58.0%) permitted full ROM at 6 weeks (median, 6 weeks; IQR, 4-6 weeks). Finally, most providers (58.5%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 60°-90°).
Case 3: Lateral Meniscus Horizontal Tear
Regarding case 3, most providers (57.6%) permitted PWB immediately after surgery (median, 0 weeks; IQR, 0-2 weeks). Similar to cases 1 and 2, the most popular time point for permitting FWB was 6 weeks (36.3%), followed by immediately (30.5%), and 4 weeks after surgery (20.3%) (median, 4 weeks; IQR, 0-6 weeks). Regarding ROM, half of the providers (50%) permitted full ROM at 6 weeks (median, 6 weeks; IQR, 4-6 weeks). Finally, most providers (58.5%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 90°-90°).
Cases 4 to 6: Tears With Loss of Hoop Integrity
Case 4: Lateral Meniscus Radial Tear at Midbody Anterior Horn Junction
For case 4, PWB was most commonly permitted at 6 weeks after surgery (41.3%), followed by 4 weeks (27.2%), and immediately after surgery (19.4%) (median, 4 weeks; IQR, 2-8 weeks). FWB was permitted by most providers at 6 weeks (51.5%), followed by 8 weeks after surgery (26%) (median, 6 weeks; IQR, 6-8 weeks). Full ROM was permitted by most providers at 6 weeks (56.4%), followed by 4 weeks after surgery (17.4%) (median, 6 weeks; IQR, 4-6 weeks). Most providers (57.9%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 60°-90°).
Case 5: Medial Meniscus Posterior Root Tear
Similarly, for case 5, PWB was most commonly permitted at 6 weeks (38.6%), followed by 4 weeks (24.33%) and immediately after surgery (23.7%) (median, 4 weeks; IQR, 2-8 weeks). Most providers permitted FWB at 6 weeks (55.4%), followed by 8 weeks after surgery (23.4%) (median, 6 weeks; IQR, 6-8 weeks). Full ROM was permitted by most providers at 6 weeks (58.9%), followed by 4 weeks after surgery (13.6%) (median, 6 weeks; IQR, 6-6 weeks). Most providers (60.6%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 60°-90°).
Case 6: Lateral Meniscus Complete Radial Tear at Popliteal Hiatus
For case 6, PWB was most commonly permitted at 6 weeks (46.4%), followed by 4 weeks (25.2%), and immediately after surgery (16.9%) (median, 4 weeks; IQR, 2-8 weeks). Most providers permitted FWB at 6 weeks (50.5%), followed by 8 weeks after surgery (28.7%) (median, 6 weeks; IQR, 6-8 weeks). Full ROM was permitted by most providers at 6 weeks (55.5%), followed by 4 weeks after surgery (14.8%) (median, 6 weeks; IQR, 6-6 weeks). Finally, most providers (57.6%) permitted 0° to 90° ROM immediately after surgery (median, 90°; IQR, 30°-90°).
Tears That Retained Versus Lost Hoop Integrity
Generally, rehabilitation restrictions were similar for all tear types with intact hoop integrity and again for all tear types with loss of hoop integrity (Table 2). However, the median times to permitted PWB and FWB were significantly lower (P < .001 for both) after repair of tears that retained hoop integrity compared with those that did not. On the other hand, time to full ROM and immediate ROM had similar medians and IQRs but demonstrated significantly different distributions between tears that retained and lost hoop integrity.
Rehabilitation Response Characteristics for Tears With Retained and Lost Hoop Integrity a
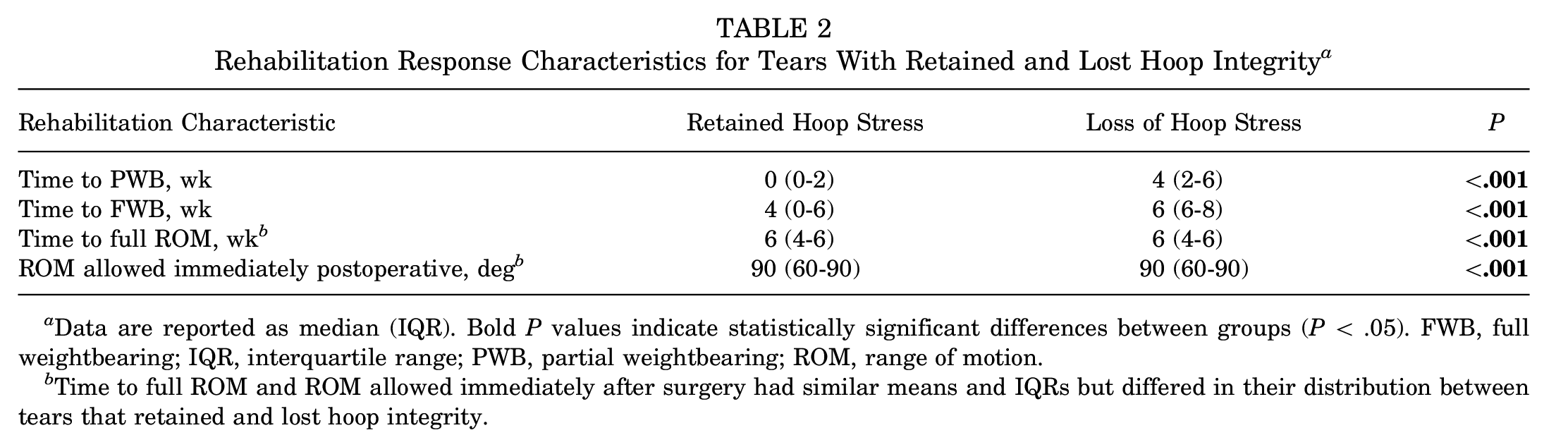
Data are reported as median (IQR). Bold P values indicate statistically significant differences between groups (P < .05). FWB, full weightbearing; IQR, interquartile range; PWB, partial weightbearing; ROM, range of motion.
Time to full ROM and ROM allowed immediately after surgery had similar means and IQRs but differed in their distribution between tears that retained and lost hoop integrity.
Perioperative Adjuncts
Most providers routinely prescribed a knee brace after meniscus repair, although a higher proportion of providers prescribed bracing for tears that lost hoop integrity (83.3%) than retained hoop integrity (76%) (P = .005). It can only be presumed that bracing was primarily used for ROM control, as further granularity cannot be established from survey responses. A majority of providers reported routine use of synovial rasping/trephination (86%) and notch microfracture (66.5%), while a minority reported use of more involved biologic supplementations—including classic fibrin clot (4.9%), platelet-rich plasma (8.9%), and bone marrow aspirate concentrate (2.9%).
Consensus Recommendations for Rehabilitation
The consensus responses to each case and question on the survey are displayed in Table 3. Consensus recommendations (ie, responses that reached >50% agreement among respondents) were achieved for each case provided.
Rehabilitation Recommendations Based on Consensus (>50% Agreement) by Tear Type a

Bold items indicate >50% agreement reached among respondents. FWB, full weightbearing; postop, postoperative; PWB, partial weightbearing; ROM, range of motion. b Use of classic fibrin clot (4.9%), platelet-rich plasma (8.9%), and bone marrow aspirates (2.9%) did not reach agreement threshold.
Discussion
The major findings of this study were that sports medicine providers offer rehabilitation for meniscal tears differently based on tear morphology and primarily by assessment of hoop integrity. The median time to permitted partial and FWB in cases 1 to 3 (tears that retained hoop integrity) was significantly lower than that of cases 4 to 6 (tears that lost hoop integrity) (P < .001). In tears with retained hoop integrity, the median time to PWB was immediate, whereas in tears without hoop integrity, the median time to PWB was 4 weeks after surgery. Similarly, the median time to FWB in tears with retained hoop integrity was 4 weeks after surgery, while it was 6 weeks after surgery in tears without hoop integrity. With regard to time to full ROM, results were similar, irrespective of tear type. All cases had a median time to full ROM of 6 weeks postoperatively. Moreover, most providers allowed 0° to 90° ROM immediately after meniscus repair, regardless of hoop integrity.
With regard to perioperative adjuncts, a majority of providers prescribed knee braces after repair regardless of hoop integrity, although they were more likely to do so for tears with loss of hoop integrity. In addition, most providers utilized synovial rasping/trephination along with notch microfracture, while only a minority used biologic augmentation.
There is a developing body of work advocating for tears with retained and lost hoop integrity to be rehabilitated differently compared with tears without hoop integrity. 19 However, meniscus study group consensus statements for repair rehabilitation from AOSSM and ESSKA (European Society for Sports Traumatology, Knee Surgery, and Arthroscopy) have yet to be published. From a biomechanical standpoint, tears with a preserved hoop tensile stress effect behave differently from tears with disruption of circumferential hoop fibers.7,34,35 Axial loading of longitudinal and bucket-handle tear repairs has been shown to compress and reduce the repair site due to the preservation of the hoop tensile stress in combination with circumferential loading.3,7,15,32 On the other hand, loading of radial and root tear repairs, in which the circumferential collagen fibers were disrupted, risks distraction across the repair site.8,26 Recent studies have advocated for accelerated weightbearing protocols with longitudinal vertical/horizontal and bucket-handle lesions but more conservative advancement of weightbearing for radial and root lesions.33,41 Interestingly, however, cadaveric and biomechanical studies have shown ROM to have less of an impact on the forces applied across various tear types. Becker et al 7 and Ganley et al 15 investigated knee flexion on meniscal healing and found no significant gapping at increased degrees of flexion, even with loading. Lin et al 22 demonstrated minimal tear or repair gapping in a cadaveric model at high degrees of flexion (up to 135°). Finally, a study by Ahmed 2 measuring in vitro static measurements supported 90° of motion, as 85% of the load travels through the meniscus with 90° of flexion, while <50% of the load passes through the meniscus in extension. These biomechanical studies are well aligned with our findings, which suggest that immediate postoperative ROM from 0° to 90° is agreeable among AOSSM members regardless of tear morphology.
Clinical studies have demonstrated success with accelerated protocols allowing early PWB and flexion for lesions with retained hoop integrity. A randomized controlled trial by Lind et al 23 compared free and restricted PWB and ROM after the repair of vertical tears and found no difference in 2-year functional scores and healing rates with the accelerated protocol. A retrospective study by Perkins et al 29 found no difference in failure rates with a weightbearing as tolerated protocol compared with a restricted weightbearing protocol after repair of peripheral, vertical meniscal tears. Suganuma et al 38 studied bucket-handle tears with inside-out fixation rehabilitated with an accelerated protocol and achieved a 100% success rate with no repair failures or patients with lingering symptoms. Kocabey et al 18 proposed tailoring rehabilitation based on tear characteristics, advocating for weightbearing as tolerated and 0° to 125° of flexion for longitudinal tears. Finally, Mariani et al 24 allowed immediate weightbearing and unrestricted ROM for 22 patients with repair of longitudinal posterior horn tears and only had 3 patients retear with 1 mm of gapping. Taken in aggregate, recent systematic reviews have recommended employing accelerated rehabilitation protocols for tears with preserved hoop tensile stress.9,27,33,41 The results of these studies are reflected in this survey of AOSSM members, a majority of whom allow immediate PWB and 90° of flexion postoperatively for tears with preserved hoop integrity. Both of these statements reached a consensus in this study.
However, in tears with loss of hoop tensile stress, including radial and root tears, there remains concerns with accelerated protocols, particularly early weightbearing. Studies have demonstrated excellent outcomes in these tears with restricted protocols. Choi et al 11 used a toe-touch weightbearing protocol for 6 weeks with 0° to 90° of flexion for radial tears and demonstrated a 7% repair failure rate while Haklar et al 16 used a dual restriction protocol with nonweightbearing and complete immobilization for 6 weeks with no repair failures. Thus, a recent systematic review has advocated for a restricted rehabilitation protocol with 0° to 90° ROM and no weightbearing for the first 6 weeks postoperatively. 9 The results of these clinical studies, compounded with the biomechanical evidence supporting early ROM, were reflected in the AOSSM membership as shown in the present study, where the most common time to PWB in cases with lost hoop integrity was 6 weeks postoperatively, while the immediate ROM allowed was 0° to 90°. In fact, 90° of immediate postoperative ROM was found to be a consensus recommendation (>50% agreement among respondents), while the 6-week time to PWB did not reach the consensus target, perhaps reflecting the paucity of clear evidence in this domain as well as the cautious attitude of AOSSM members toward radial tear types.
Postoperative bracing was performed routinely regardless of tear type by most respondents in the survey. Although not explicitly elicited in our survey, this likely reflects brace utilization for ROM control. In addition, mechanical augmentation with rasping/trephination, as well as notch microfracture, were utilized by most providers. Preclinical studies have found that these mechanical methods may stimulate tissue healing and remodeling in animal models.4,28,45 Applied clinically, patients with trephination and synovial rasping intraoperatively in conjunction with meniscus repair have been shown to have excellent outcomes and reduced failure rates compared with controls.13,39,40,44 Biological augmentation, on the other hand, remains controversial. A recent systematic review by Zaffagnini et al 43 suggested that platelet-rich plasma (PRP) may be useful in decreasing meniscus repair failure rates but that other methods do not have sufficient evidence to support their use. As such, the survey findings indicated that biological augmentation was used much less frequently than mechanical stimulation, with only 9% routinely using PRP intraoperatively, 5% using fibrin clot, and 3% using bone marrow aspirate concentrate.
To our knowledge, no previous study has assessed the current practice of meniscus repair rehabilitation for the various tear types on a national scale. We believe that the present study is timely, especially with recent literature advocating tailored rehabilitation strategies based on tear type and the rising popularity of accelerated rehabilitation protocols. Our findings indicate that many sports medicine practitioners do indeed see the need for tailored rehabilitation based on the integrity of hoop stress and subsequently allow earlier weightbearing for tears with retained hoop stress while allowing 0° to 90° ROM immediately regardless of tear type.
Limitations
This study is subject to limitations. First, this was an observational survey-based study and is therefore subject to sample and cognitive bias. Second, response options for questions in the survey were limited to multiple-choice responses, which may not comprehensively represent rehabilitation practices among respondents. Third, this survey was limited to a single orthopaedic sports medicine society, which may not be fully representative in its membership of national or international medical providers that treat meniscal tears. However, AOSSM does represent a group of often academic practitioners well respected in the field of sports medicine. Fourth, because of its survey-based design, this study is subject to a high nonresponse rate, as evidenced by the 15.2% response rate. However, this study was still able to garner over 400 responses; thus, it represents a reasonable sample of practitioners who treat meniscal tears. Finally, there is no definitive comparative evidence that accelerated or restricted protocols translate into improved clinical outcomes postoperatively, and this study could not address this clinical question.
Despite these limitations, information from the survey could be translated into consensus-based recommendations and may contribute to future guidelines for rehabilitation protocols based on tear types. Future studies should correlate the various rehabilitation protocols for each tear type to clinical outcomes to outline each tear's optimal rehabilitation strategy. In addition, future work may focus on repair and rehabilitation options based on additional clinical factors, such as intraoperative tissue quality, and may address return to play for various tear morphologies in relation to sports and athletes.
Conclusion
Sports medicine practitioners who were surveyed saw the need for tailored rehabilitation of meniscal tears based on the integrity of hoop stress and generally permitted earlier weightbearing for tears with retained hoop stress while allowing 0° to 90° ROM immediately after surgery, irrespective of tear type. Most practitioners braced and utilized in situ adjuncts for biological healing, while a minority added extrinsic biologics. Rehabilitation recommendations could be provided for each tear type, which is important, as there remains a paucity of level 1 evidence studies to inform rehabilitation guidelines for meniscus repair.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231226134 – Supplemental material for Current Practices for Rehabilitation After Meniscus Repair: A Survey of Members of the American Orthopaedic Society for Sports Medicine
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231226134 for Current Practices for Rehabilitation After Meniscus Repair: A Survey of Members of the American Orthopaedic Society for Sports Medicine by Ting Cong, Rajiv P. Reddy, Arielle J. Hall, Akhmad Ernazarov and James Gladstone in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted May 25, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.G. has received financial or material support from Springer; education payments from Gotham Surgical Solutions & Devices; consulting fees from Mitek, Trice Medical, Medical Device Business Services, and DePuy Synthes Products; nonconsulting fees from Mitek and Trice Medical; royalties from Springer; and stock options from Trice Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Mount Sinai Hospital (ref No. STUDY-21-00236).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.