
Abstract
Background:
Surgical correction for recurrent patellar dislocation (RPD) can improve femoral trochlear morphology; nonetheless, the effects of surgical correction on femoral condyle morphology are unclear.
Purpose:
To investigate the morphological changes in the posterior femoral condyle in skeletally immature patients with RPD and trochlear dysplasia (TD) after surgical correction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 20 skeletally immature patients with bilateral RPD and TD were included in this study. For each patient, the knee that was dislocated more frequently or had sustained a recent injury was treated with medial patellar retinaculum plasty (group S; n = 20 knees), and the asymptomatic or only occasionally dislocated contralateral knee was treated conservatively (group C; n = 20 knees). The lengths of the anterior medial and lateral femoral condyles and the lengths of the posterior medial and lateral femoral condyles were evaluated preoperatively and at the final follow-up. Trochlear morphological characteristics, tibial tuberosity–trochlear groove distance, and patellar tilt angle were compared between preoperative and final follow-up values with the 2-sample paired Student t test and were compared between groups S and C with the independent-samples t test.
Results:
The mean follow-up time was 60.7 ± 4.8 months. No knee in group S experienced a redislocation, whereas 80% (16/20) of knees in group C experienced a dislocation. There were significant group differences in the ratio of the posterior medial femoral condyle (PMFC) to the posterior lateral femoral condyle (PLFC) (group S, 1.08 ± 0.05; group C, 1.14 ± 0.06; P = .042). There was no significant difference in the ratio of the anterior lateral femoral condyle to the anterior medial femoral condyle (group S, 1.16 ± 0.13; group C, 1.18 ± 0.09; P = .635). In group S, all trochlear morphological characteristics and patellofemoral joint characteristics improved compared with preoperatively (P≤ .047 for all). In addition, all values significantly differed between groups S and C at the final follow-up (P≤ .044 for all).
Conclusion:
The study findings demonstrated that the morphology of the posterior femoral condyle in skeletally immature patients with bilateral RPD and TD changes after surgical correction, with the PLFC growing faster than the PMFC.
Keywords
Recurrent patellar dislocation (RPD) is a common orthopaedic disorder.9,36 The cause of patellar dislocation is multifactorial and includes trochlear dysplasia (TD), patella alta, lower limb malalignment, and relative rotation of the femur and tibia.5,6,30 Dejour et al 5 reported that 85% of patients with RPD had TD. However, some studies have found that patients with RPD have not only an increased rate of TD but also a morphological abnormality in the posterior femoral condyle.3,34 A study by Roger et al 34 reported that the posterior part of the lateral condyle is shorter and smaller than the medial condyle in patients with RPD and TD. Biedert and Bachmann 3 found that the posterior lateral femoral condyle (PLFC) was smaller and the posterior medial femoral condyle (PMFC) was larger in patients with TD than in normal controls. Moreover, valgus alignment is another risk factor for hypoplasia of the lateral distal femoral condyle and lateral patellar instability, which increases the Q angle and contributes to maltracking of the patella.38,33 Excessive rotation can be expected during extension in patients with hypoplasia of the PLFC, contributing to patellar dislocation. 12
Controversy still remains on how to manage skeletally immature patients with RPD and TD. Excellent results have been reported with medial patellofemoral ligament (MPFL) reconstruction in adults, whereas cases of failure have been reported in skeletally immature adolescents after MPFL reconstruction.2,11,35,15 Considering the significant contribution of the distal femoral growth plate to longitudinal growth, injury of the physes must be avoided to prevent leg-length deformities of the limb. 15 In recent years, a soft tissue surgical technique called the medial patellar retinaculum plasty was proposed.8,16,20 In this surgery, the vastus medialis oblique head and joint capsule are used to reconstruct the medial complex, which is thought to restore the MPFL by avoiding the femoral growth plate. 16 Excellent clinical results of soft tissue surgery have been demonstrated in the literature.8,10,23,25
The morphology of the trochlea can be significantly changed by early soft tissue surgery in skeletally immature patients with RPD and TD.2,10 A study by Benoit et al 2 with an 11-year clinical follow-up period reported that the realignment surgery could remodel the TD at a young age. Another study also demonstrated that the femoral trochlear morphology could be changed by surgical correction in children with RPD and TD. 10 However, no author has focused on the morphological changes in the posterior femoral condyle for skeletally immature patients with RPD and TD after surgical correction.
Our study aimed to investigate the changes in the posterior femoral condyle after soft tissue surgery in skeletally immature patients with RPD and TD. It was hypothesized that the morphology of the posterior femoral condyle would change and that the PLFC would grow faster than the PMFC after surgical correction.
Methods
We followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for this study. Ethical approval for the study protocol was acquired from our institutional ethics board, and informed consent was obtained from all patients before the initiation of this study.
All included patients were initially evaluated at our institution between January 2014 and August 2017. The patients were selected based on the following inclusion criteria: (1) bilateral RPD; (2) adolescent patients with open femoral growth plates—open femoral growth plates as confirmed on knee radiographs; (3) Dejour type A TD and a flat trochlea—Dejour type B 5 ; and (4) concomitant MPFL injury. The exclusion criteria were as follows: (1) patients with previous knee surgery; (2) patients with closed physes; (3) patients with a convex trochlea—Dejour type B; (4) patients with high-grade TD (Dejour types C-D)—when high-grade TD is present, it is necessary to perform other procedures to counteract the adverse effect; (5) patients with concomitant cruciate ligament or collateral ligament injury; (6) patients with rheumatoid arthritis or osteonecrosis with cartilage damage >grade 2 (Outerbridge classification), as evaluated by arthroscopy; (7) patients who did not complete conservative treatment for at least 12 months.
Ultimately, 20 skeletally immature patients were included in our study. All patients were diagnosed with bilateral RPD and TD. For each patient, the knee that was more frequently dislocated or sustained the most recent injury underwent surgical medial patellar retinaculum plasty (group S; n = 20), and the asymptomatic or only occasionally dislocated contralateral knee was treated conservatively (group C; n = 20). A flowchart of patient selection is shown in Figure 1.

A flowchart of patient selection in this study. RPD, recurrent patellar dislocation; TD, trochlear dysplasia.
Surgical Technique: Medial Patellar Retinaculum Plasty
All operations were performed by a senior orthopaedic surgeon (X.W.) with 20 years of experience in knee surgery, who specializes in osteoarthritis and patellar dislocation. The diagnostic arthroscopic assessment was performed, and chondral lesions and concomitant pathology were addressed in all patients before medial patellar retinaculum plasty was performed. Arthroscopic lateral retinacular release (ALRR) has been indicated for patients with lateral retinacular tightness or large patellar tilt. 40 A force-directed medial shift of the patella by less than one-fourth of its width indicates excessive tension of the lateral retinaculum. 10 For such patients, ALRR is often required. 40
For medial patellar retinaculum plasty, the vastus medialis oblique head, the fascia, and the joint capsule were used to construct the new, stable medial complex, which formed a vector structure to prevent redislocation of the patella and avoid damage to the distal femoral physes.10,25
First, a longitudinal incision was made at the border between the medial border of the patella and the vastus medialis muscle, and the fascia and reticulum were identified. Then, a transverse incision was made at the junction of the vastus medialis muscle and the medial retinaculum of the patella to mobilize it. The knee joint was flexed 30°, and then the patella was held in the proper position within the trochlear groove. Second, after the position of the patella was adjusted, the medial retinaculum of the patella was pulled proximally and temporarily sutured to the proximal medial edge of the patella using polydioxanone synthetic absorbable suture (PDS-I) (DePuy Synthes). The vastus medialis muscle fibers were pulled distally and sutured to the distal end of the patella. The position of the patella during knee flexion and extension was evaluated to ensure that the patellofemoral joint closely matched the correct position. 16 Finally, the wound was rinsed thoroughly and sutured in layers.
Postoperative Rehabilitation
Group S
All patients were guided by the same rehabilitation therapist and adopted the same rehabilitation method. Patients were asked to wear a motion-restricting knee brace after surgery. Quadriceps strength training, such as straight-leg raising, was started immediately after surgery. Then patients continued partial weightbearing. After 4 weeks, the knee brace was removed, and full weightbearing was resumed. Knee flexion up to 30° was permitted for 1 week, and up to 90° was permitted for 4 weeks. Patients were allowed to return to normal activities of daily living after 2 months and to resume normal sports after 4 months.
Group C
Nonoperative treatment on the contralateral knee was started immediately after surgery. First, a motion-restricting knee brace was used to protect the patella from lateralization and limit the range of motion (ROM). Quadriceps muscle strengthening to restore the dynamic component of the patellar soft-tissue stabilizers and kinesiotherapy to recover full ROM were necessary for patients.28,32 The most common strategy includes isometric and isotonic quadriceps strengthening exercises, such as straight-leg raises, squats, and lunges. 24
Outcome Evaluation
Axial computed tomography (CT) scans were performed preoperatively and at the final follow-up in all patients to assess the morphology of the femoral condyle and femoral trochlea as well as the changes in patellar positioning. All measurement methods are shown in Table 1. At the final follow-up, CT scans were undertaken again to evaluate the changes in the femoral condyle. Patellar, femoral trochlear, and condylar morphologies were measured with the transcondylar axis as the reference line, respectively. 5 The best CT cross-section of the Roman dome was selected to show the morphology of the femoral trochlea and femoral condyle (Figure 2). 37 Given that the medial condyle was flat in patients with TD, the vertical distance from the inflection point or vertex of the medial trochlea to the transcondylar line was selected to express the length of the medial anterior condyle. The measurements of the femoral condyle characteristics are shown in Figure 2. To reduce the effect of individual height on bone volume, the ratio of the lengths of the femoral condyles was used to show the relative changes: anterior lateral femoral condyle (ALFC)/anterior medial femoral condyle (AMFC) and PMFC/PLFC. The methods for evaluating trochlear morphology and the tibial tubercle–trochlear groove (TT-TG) distance are shown in Figures 3 and 4, respectively. All data were measured using RadiAnt DICOM Viewer software (Medixant Ltd), which has an accuracy of 0.01° for angles and 0.01 mm for distance.
Description of Morphometric Parameters a
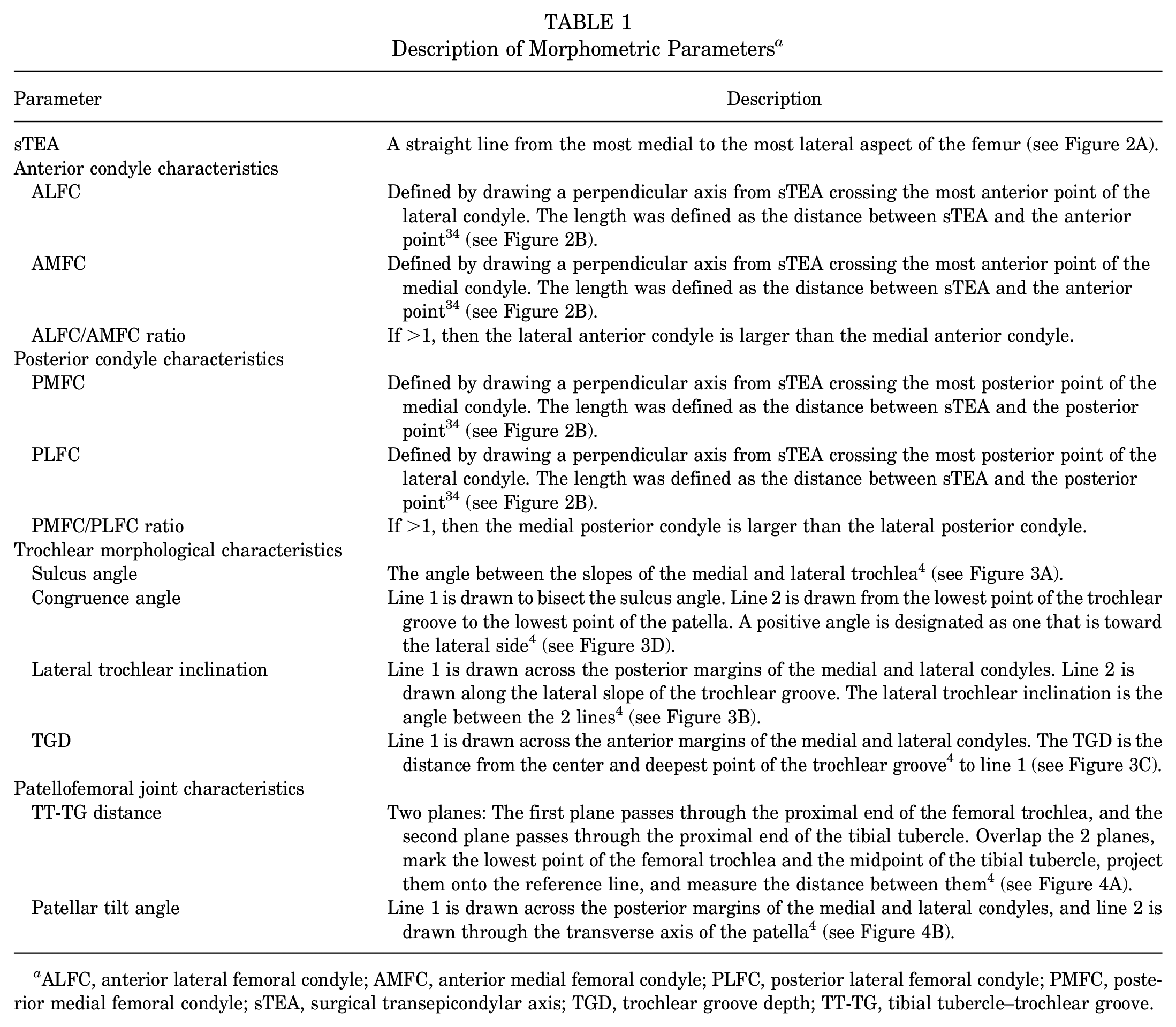
ALFC, anterior lateral femoral condyle; AMFC, anterior medial femoral condyle; PLFC, posterior lateral femoral condyle; PMFC, posterior medial femoral condyle; sTEA, surgical transepicondylar axis; TGD, trochlear groove depth; TT-TG, tibial tubercle–trochlear groove.
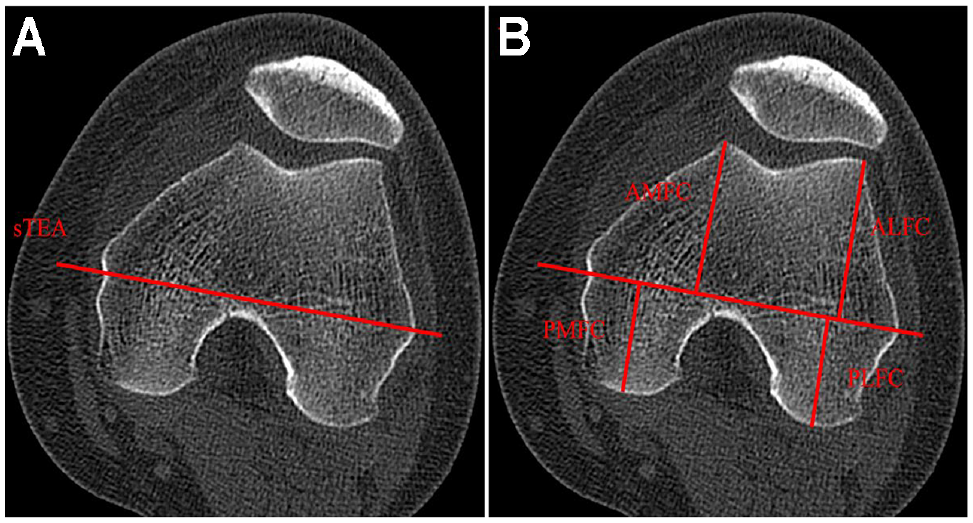
Measurement of the length of the femoral condyles. (A) The anteroposterior dimensions of the sTEA at the level of the Roman dome. (B) The characteristics of the anterior and posterior condyles. ALFC, anterior lateral femoral condyle. AMFC, anterior medial femoral condyle. PLFC, posterior lateral femoral condyle; PMFC, posterior medial femoral condyle; sTEA, surgical transepicondylar axis.

Measurements of trochlear morphological characteristics. (A) Sulcus angle: the angle between Line 1 and Line 2. (B) Lateral trochlear inclination: the angle between Line 1 and Line 2. (C) Trochlear groove depth (yellow line): the distance from the center and deepest portion of the trochlear groove to Line 1. (D) Congruence angle: Line 1 (yellow line) is drawn to bisect the sulcus angle of the trochlear groove. The congruence angle is the angle between Line 1 and Line 2.

(A) TT-TG distance: Line 1 is perpendicular to the tangent to the posterior condyle and passes through the lowest point of the femoral trochlea. Line 2 is parallel to Line 1 through the most anterior portion of the tibial tuberosity. The TT-TG distance (yellow line) is the distance between a and b. (B) Patellar tilt angle: Line 1 is the tangent line of the medial and lateral posterior condyle, and Line 2 is across the maximum transverse diameter of the patella. The patellar tilt angle is the angle between them. TT-TG, tibial tubercle–trochlear groove.
Statistical Analysis
Statistical analysis was performed using SPSS statistical software Version 26.0 (SPSS Inc). All data are expressed as the mean ± standard deviation. The Kolmogorov-Smirnov test was used to test the normality of numerical data; all numerical variables showed a normal distribution or equal variance. Measurements between the preoperative assessment and the final follow-up were compared using the 2-sample paired Student t test, and the Student t test was used to compare the differences in variables between groups S and C. Also, statistical significance was set at P < .05. Given the effect of ALRR, subgroup analysis was conducted by stratifying the results according to whether the ALRR was performed.
To reduce measurement errors, all data were measured by 2 researchers (Z.S. and A.F.) under the same conditions, and after a 6-week interval, all data were measured again by a single researcher (Z.S.). The intraclass correlation coefficient (ICC) was used to test the intra- and interrater reliability of the measurements. An ICC of >0.75 indicated excellent reliability. An a priori power analysis with a prespecified alpha level of .05 and an effect size of 0.8 showed that a minimum sample size of 18 participants was necessary for this study.
Results
The mean age of the 20 study participants was 13.7 ± 1.9 years (range, 10-15 years). Thirteen patients had patellar dislocation due to trauma, while the other 7 patients had no history of trauma. The mean follow-up time was 60.7 ± 4.8 months (range, 53-67 months). The characteristics of patients are summarized in Table 2. At the final follow-up, no knee in group S experienced patellar redislocation; however, occasional discomfort was felt in 2 knees, and these patients could not return to sports activities. Sixteen knees in group C experienced another instance of patellar dislocation.
Characteristics of the Study Population (N = 20) a

Data are reported as mean ± SD (range) or n (%). BMI, body mass index.
Evaluation of the Femoral Condyle
Preoperatively, the ratio of the anterior femoral condyle length to the posterior femoral condyle length was not significantly different between the 2 groups (P≥ .884) (Table 3). At the final follow-up, the ALFC/AMFC ratio was not significantly different between the 2 groups. However, significant group differences were observed in the PMFC/PLFC ratio (group S: 1.08 ± 0.05; group C: 1.14 ± 0.06; P = .042). The outcomes of the subgroup analysis regarding the influence of arthroscopic lateral retinacular release are shown in Table 4. In group S, 12 of 20 knees underwent medial patellar retinaculum plasty combined with ALRR, and 8 of 20 knees underwent isolated medial patellar retinaculum plasty in group S. We noted no significant difference between groups with versus without ALRR in the length ratio of the posterior and anterior femoral condyles (Table 4).
Characteristics of Femoral Condyles Preoperatively and at the Final Follow-up a

Data are reported as mean ± SD. Bold P values indicate statistically significant differences between groups (P < .05). ALFC, anterior lateral femoral condyle; AMFC, anterior medial femoral condyle; PLFC, posterior lateral femoral condyle; PMFC, posterior medial femoral condyle.
Student t test.
Paired Student t test.
Subgroup Analysis of the Changes in Femoral Condyles Between Knees Undergoing Medial Patellar Retinaculum Plasty With Versus Without ALRR a

Data are reported as mean ± SD. Bold P values indicate statistically significant differences between groups (P < .05). ALFC, anterior lateral femoral condyle; ALRR, arthroscopic lateral retinacular release; AMFC, anterior medial femoral condyle; PLFC, posterior lateral femoral condyle; PMFC, posterior medial femoral condyle.
Student t test.
Paired Student t test.
Evaluation of Trochlear Morphology and Patellofemoral Joint Stability
There were no significant differences in any of the trochlear morphological and patellofemoral joint characteristics between the groups preoperatively. At the final follow-up, however, significant group differences were seen on all variables, including the sulcus angle (SA) (group S, 132.67°± 7.16°; group C, 143.89°± 6.95°; P = .004), congruence angle (group S, 19.25°± 10.46°; group C, 31.50°± 9.89°; P = .03), lateral trochlear inclination (group S, 26.50°± 3.73°; group C, 21.43°± 3.78°; P = .034), patellar tilt angle (PTA) (group S, 18.65°± 5.86°; group C, 24.11°± 3.80°; P = .044), trochlear groove depth (TGD) (group S, 4.87 ± 1.17 mm; group C, 3.84 ± 0.61 mm; P = .033), and TT-TG distance (group S, 12.01 ± 2.33 mm; group C, 16.54 ± 2.59 mm; P = .004) (Table 5). In addition, all parameters improved significantly in group S compared with their preoperative values (P≤ .047 for all).
Morphological Characteristics Preoperatively and at the Final Follow-up a

Data are reported as mean ± SD. Bold P values indicate statistically significant differences between groups (P < .05). LTI, lateral trochlear inclination; PTA, patellar tilt angle; TGD, trochlear groove depth; TT-TG, tibial tuberosity-trochlear groove distance.
Student t test.
Paired Student t test.
The ICC values for intra- and interrater reliability of all measurements are shown in Table 6. Most of the ICCs of the radiological measurements were excellent. The intraobserver ICCs ranged from 0.503 to 0.989, and the interobserver ICCs ranged from 0.670 to 0.987, indicating that the radiographic measurements were highly reliable.
Intra- and Interrater Reliability of the Measurements a

Data are reported as ICC (95% CI). ALFC, anterior lateral femoral condyle; AMFC, anterior medial femoral condyle; ICC, intraclass correlation coefficient; PLFC, posterior lateral femoral condyle; PMFC, posterior medial femoral condyle; TT-TG, tibial tuberosity–trochlear groove distance.
Discussion
The most important finding of our study was that the morphology of the posterior femoral condyle in skeletally immature patients with RPD and TD changed after surgical correction, with the PLFC growing faster than the PMFC. When the ratio of femoral condyles between the knees that underwent surgical versus conservative treatment was compared, significant changes were found at the final follow-up (P = .042). In addition, the PMFC/PLFC ratio decreased from 1.11 ± 0.07 preoperatively to 1.08 ± 0.05 at the final follow-up in the surgically treated knees (P = .015). We conducted a subgroup analysis considering the effects of ALRR on patients; however, there were no significant differences observed between patients with versus without ALRR. To our knowledge, this is the first study to investigate the changes in the femoral condyle after medial patellar retinaculum plasty.
The morphology of the trochlear and femoral condyles has been found to differ between people with versus without RPD.17,22,39 Van Haver et al 39 also found the same phenomenon reported by Roger et al 34 and Liu et al 22 and explained the abnormal changes in femoral condyles as a compensatory enlargement to maintain the overall morphology of the femur. The morphology of the distal femur is affected by genes and acquired mechanical alignment.13,14,21,26 Early surgical intervention was able to change the morphology of the femoral trochlea in pediatric patients, and we believe that femoral changes are not isolated but have effects throughout the distal femur; early surgical intervention appears to affect not only the trochlea but also the posterior femoral condyle.
The TT-TG distance has been described as an important measure to gauge coronal-plane malalignment as a risk factor for patellar instability. 27 A TT-TG distance of ≥20 mm represents an excessively lateral position of the tuberosity and malalignment of patellar tracking.18,19,27 Patellar tracking is governed by a complex interaction between soft tissues and bony structures. 18 Therefore, a medializing osteotomy is necessary for patients with a TT-TG distance of ≥20 mm, given that soft tissue surgery cannot correct malalignment of patellar tracking.1,29,31 The mean TT-TG distance was <20 mm in both study groups (group S, 16.50 ± 4.67 mm; group C, 16.72 ± 3.99 mm; P > .05); therefore, the soft tissue surgery for skeletally immature patients with RPD and TD was able to treat patellar dislocation.
The PTA is an excellent indicator for evaluating the change in patellar position. Dejour et al 5 compared the PTA of healthy people to that of people with patellar dislocation and concluded that the inclination angle of the patella in the patients with PD was 16.3°± 3.3°. The PTA was 24.75°± 4.27° preoperatively and 18.65°± 5.86° postoperatively in group S, representing a statistically significant change (P = .026). Benoit et al 2 evaluated children with patellar dislocation for an mean of 13 years and found that surgically treated patients with patellar dislocation had significant changes in the SA. The SA was also significantly different between groups S and C (132.67°± 7.16° vs 143.89°± 6.95°, respectively; P = .004). Dejour et al 5 found that 85% of knees with patellar instability had a depth that measured ≤4 mm. The TGD significantly differed between groups (group S: 4.87 ± 1.17 mm; group C: 3.84 ± 0.61 mm; P = .033). Charles et al 4 and Escala et al 7 showed that the mean TGD in healthy people was >6 mm, while a TGD of <4 mm indicated patellar instability and TD. The results found in the present study were consistent with the measurements reported by Fu et al. 10
There is a lack of relevant research on the changes in the femoral anterior condyle after soft tissue surgery. Roger et al 34 mentioned how to measure the bilateral anterior condyles on axis CT but did not explain the difference between the bilateral anterior condyles of patients with RPD and those of healthy people. In our study, the ALFC/AMFC ratio was not significantly different between groups (group S, 1.16 ± 0.13; group C, 1.18 ± 0.09; P = .635); nonetheless, the values of TGD were significantly different, which suggested that the major changes took place in the trochlear groove after surgery. Therefore, the mechanism of morphology about the anterior femoral condyle is complicated and requires further research.
Limitations
This study is not without limitations. The sample size was too small; increasing the sample size would make the study results more accurate. CT assessment can accurately reflect the development of bones; nevertheless, this study did not consider the influence of cartilage factors in the population with patellar dislocation, and different cartilage thicknesses also affected the measurement of the length of the posterior femoral condyle. Finally, without a healthy control group, we cannot conclusively infer what is normal or abnormal or determine whether the changes in the posterior femoral condyles would tend to normalize or abnormalize over time. All of these questions need further investigation.
Conclusion
Study findings indicated that the morphology of the posterior femoral condyle in skeletally immature patients with RPD and TD had changed, and the PLFC grew faster than the PMFC after surgical correction.
Footnotes
Acknowledgements
The authors thank the staff of the participating departments for their support during the study.
Final revision submitted August 12, 2023; accepted August 17, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Third Hospital of Hebei Medical University (ref No. 2022-072-1).