
Abstract
Background:
An accurate and objective criterion is needed to determine candidates who are suitable for hip arthroscopy in patients with femoroacetabular impingement (FAI).
Purpose:
To determine whether improvement in pain after ultrasound (US)-guided intra-articular hip injection during standardized examinations can be used to predict the outcomes of hip arthroscopy in patients with FAI.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We enrolled 119 patients with FAI who underwent US-guided intra-articular hip injection of local anesthesia during standardized examinations, carried out from May 2018 to February 2020 (within 2 weeks before hip arthroscopy). All patients had undergone a minimum of 6 months of nonoperative treatment without remission and had 2-year follow-up data. Pain visual analog scale (VAS) scores (0-10) were recorded for 7 different physical examination tests, and a total score (0 [best] to 70 [worst]) was obtained. In addition, International Hip Outcome Tool–12 (iHOT-12) and modified Harris Hip Score (mHHS) scores were recorded before hip arthroscopy and at final follow-up. According to whether patients achieved the substantial clinical benefit (SCB) on the iHOT-12, they were divided into SCB and non-SCB groups, and the improvement in VAS pain scores from preinjection to postinjection (ΔVAS pain) was compared between the 2 groups. Logistic regression analysis was used to predict the achievement of SCB, and the area under the receiver operating characteristic curve (AUC) was used to estimate the accuracy of the prediction.
Results:
There was a significant pre- to postoperative increase in iHOT-12 (31.6 points; P < .001) and mHHS (20.0 points; P < .001) scores, and 84 (70.6%) patients achieved the SCB. The ΔVAS pain score was significantly greater in the SCB versus the non-SCB group (16.0 vs 7.0 points; respectively; P < .001). Logistic regression analysis demonstrated an optimal cutoff value of 8.5 points for ΔVAS pain (AUC, 0.772; 95% CI, 0.687-0.858). For patients with more severe symptoms (total preinjection VAS pain score of >10 out of 70), the accuracy of the prediction for ΔVAS pain had a better evaluation value (AUC, 0.834; 95% CI, 0.676-0.992).
Conclusion:
Improvement in pain after US-guided intra-articular hip injection predicted the outcomes of hip arthroscopy in patients with FAI in this study, especially for patients with more severe pain.
Keywords
Femoroacetabular impingement (FAI) is defined as a collection of hip-shape abnormalities that cause impingement between the femoral neck and the rim of the acetabulum 12 that may lead to pathological intra-articular changes such as chondral injury and labral damage and now is suggestive of early osteoarthritis. 4 Treatment options for FAI include nonsurgical treatment, hip arthroscopy, 7 and open surgery. Nonsurgical treatments cannot provide curative treatment for shape abnormalities. 28 Open surgery, as a more invasive treatment, comes with higher risks such as the development of intra-articular adhesions and the need for conversion to total hip arthroplasty.2,24 Hip arthroscopic surgery has demonstrated similar outcomes to open surgery 21 and is now gaining popularity for the treatment of FAI. 26 Multiple studies have reported favorable short- and intermediate-term clinical outcomes of hip FAI arthroscopy, ranging from good to excellent.23,26 Nevertheless, treatment failure, such as remaining pain symptoms or poor functional outcomes, does occur due to improper selection of surgical indications. 29 Therefore, accurate selection of patients before hip arthroscopy is important to optimize patient outcomes and minimize complications.
The criteria formulated to evaluate whether a patient is a suitable candidate for hip arthroscopy are based on factors including clinical characteristics and imaging manifestations.18,27 Intra-articular hip injection of anesthetic has been used to identify the source of pain, to diagnose FAI, and to predict the outcomes of arthroscopy.1,8,11,14 A 2021 study by Li et al 13 showed that arthroscopic treatment of FAI in patients with a postinjection International Hip Outcome Tool–12 (iHOT-12) score of ≥10 yielded a satisfaction rate of 96.6%. However, that study had a short follow-up period (12 months) and a relatively small sample size (60 patients).
The visual analog scale (VAS) score for pain during hip physical examination may provide an objective response to hip joint damage, and a comparison of VAS pain scores before and after intra-articular hip injection may help to evaluate patients’ pain relief more objectively and quantitatively. Ultrasound (US) is a convenient real-time dynamic imaging guidance method that does not involve radiation, which may achieve more accurate satisfactory results than fluoroscopic-guided injections.
The purpose of this study was to determine whether the improvement in VAS pain scores after US-guided intra-articular hip injection of anesthetic can be used to predict the outcomes of hip arthroscopy in patients with FAI.
Methods
Patients
From May 2018 to February 2020, a total of 119 patients (63 male and 56 female) with a mean age of 37.0 ± 12.5 years (range, 14-69 years) were consecutively enrolled in this study. Their clinical data, including age, sex, height, weight, body mass index (BMI), and symptom duration, were recorded. The protocol for this study was approved by the institutional review board of our hospital, and informed consent for treatment procedures was obtained from each participant.
The inclusion criteria were as follows: (1) patients with a clinical diagnosis of FAI made by a combination of physical examination and imaging findings (for cam impingement: alpha angle ≥50° on frog leg lateral view or Dunn lateral view radiographs or radial oblique magnetic resonance imaging; for pincer impingement: presence of a crossover sign or a lateral center-edge angle ≥40°; for combined impingement: patients meeting both of the above criteria) 10 ; (2) no improvement after 6 months of nonoperative treatment; (3) patients who received US-guided intra-articular hip injection of anesthesia within 2 weeks of arthroscopic surgery for FAI; and (4) patients with ≥2 years of follow-up data. The exclusion criteria were as follows: (1) acetabular dysplasia and a lateral center-edge angle of <25° (anteroposterior view of the pelvis); (2) hip osteoarthritis (Tönnis grade ≥2); (3) history of hip fracture or surgery; (4) lumbar spine disease, ankylosing spondylitis, or sacroiliac joint lesions; (5) rheumatic diseases or femoral head necrosis; and (6) no improvement in total VAS pain scores from before to after the hip injection. A flowchart of the inclusion and exclusion of patients is displayed in Figure 1.

Flowchart of patient inclusion and exclusion.
US-Guided Intra-articular Hip Injection
US-guided intra-articular hip injection was performed using a Mylab Twice US System (Esaote) with a CA541 convex transducer (central frequency, 4.5 MHz; ranging from 1 to 8 MHz) by the senior sonographer (M.-B.Z.), who had >10 years of experience in interventional and musculoskeletal US.
The patient lay supine with the affected hip in natural abduction and external rotation. First, a survey scan of the hip joint was performed by US, enabling visualization of the anterior rim of the acetabulum, femoral head, femoral neck, and anterior recess. Second, the patient's anterior hip and groin area were sterilized. Longitudinal sections of the femoral neck were displayed by US. A 21-gauge 200-mm core needle (Hakko) was introduced from head to foot along the articular capsule to the anterior recess of the hip joint by the intraplane technique. Third, a small amount of liquid was injected to observe resistance. In the case of no resistance, we continued the injection; otherwise, we adjusted the direction of the tip until there was no resistance to the injection. An anesthetic mixture of 4 mL 2% lidocaine (200mg/10mL; Suicheng Pharmaceutical) and 4 mL 1% ropivacaine (100 mg/10 mL; AstraZeneca) was injected into the hip cavity.
VAS Pain Measured During Hip Physical Examination Testing
Before and 20 minutes after the injection, 7 physical examination tests were performed: the log roll test (internal rotation); log roll test (external rotation); internal rotation with the hip flexed 90°; external rotation with the hip flexed 90°; hyperflexion; flexion, abduction, internal rotation (FADIR) test; and the flexion, abduction, external rotation (FABER)/Patrick test. 15 The VAS pain score (0 [no pain] to 10 [worst possible pain]) before and after US-guided intra-articular injection of anesthesia for each examination position was recorded by the senior sonographer within a standard report format (Figure 2). A total VAS pain score (range, 0 [best] to 70 [worst]) was calculated by summing the results of the scores for the 7 physical examination tests. In addition, we calculated the relative percentage improvement in VAS pain (termed the “VAS remission rate”) by dividing the difference in total VAS pain scores by the preinjection score: Remission rate = [(Preinjection VAS – Postinjection VAS)/Preinjection VAS] × 100%.

The report format of VAS pain scores during physical examination before and after ultrasound-guided intra-articular injection. CDFI, color Doppler flow imaging; FABER, flexion, abduction, external rotation; FADIR, flexion, abduction, internal rotation; VAS, visual analog scale.
Hip Arthroscopy and Rehabilitation
Hip arthroscopy was performed by an experienced orthopaedic surgeon (C.-B.L.) who was blinded to the patient's VAS pain scores. Patients were positioned supine on a traction table. 5 The anterolateral, midanterior, and distal accessory portals were established under traction to provide visualization of the central and peripheral compartments. Additional exposure was provided by a T-type capsulotomy. 5 Acetabuloplasty was performed to correct pincer deformities. A looped circumferential stitch or the pierce-through technique was used to fix the torn labrum. If the labrum had severely degenerated or calcified, it was selectively debrided until a stable portion remained. If a cam deformity was present, femoral osteochondroplasty was performed to restore the native head-neck offset. The articular capsule was sutured at the end of the operation.
All patients underwent a standardized rehabilitation protocol. The surgical leg was restricted to 30% foot flat weightbearing, and the hip joint was allowed to passively flex to 90° the day after the operation. At week 4, patients were allowed to wean off crutches if they could tolerate ambulation without significant pain. At week 6, patients were allowed to use the elliptical machine. Patients were allowed to progress to sport-specific activities at week 24. 19
Postoperative Outcome Measures
All patients completed the iHOT-12 and modified Harris Hip Score (mHHS) before and at minimum 2-year follow-up after the hip arthroscopy procedure to evaluate surgical outcomes, and all scores were recorded by a single sonographer (Y.-J.S.) who was blinded to VAS pain scores. Follow-up outcome data were collected by telephone. The definition of substantial clinical benefit (SCB) in the context of hip arthroscopy, which objectively indicated satisfactory results of the procedure, was based on a previously published SCB change score of 28 points on the iHOT-12.10,16 According to whether patients achieved the SCB on the iHOT-12, they were divided into SCB and non-SCB groups.
Statistical Analysis
All statistical analyses were performed using SPSS Version 19.0 (IBM) and MedCalc Version 20.114 statistical software. Age, height, weight, BMI, symptom duration, VAS pain, and iHOT-12 scores were reported as mean ± SD (range) or median (interquartile range), and pain location and patient sex were reported as numbers (ratios). The paired t test was used to compare the difference before and after arthroscopy in terms of the iHOT-12 score and mHHS. The Student t test, Mann-Whitney U test, and chi-square test were used to evaluate the differences in features and the improvement in VAS pain from preinjection to postinjection (ΔVAS pain) between the SCB and non-SCB groups. Then, univariate and multivariate binary logistic regression models were established to estimate the achievement of SCB. Receiver operating characteristic (ROC) curves of the regression model were constructed, and the area under the ROC curve (AUC), sensitivity, specificity, and accuracy were calculated to estimate their diagnostic accuracy for SCB achievement. Comparisons between AUCs were made by using the Delong test. P values <.05 were considered statistically significant.
Results
Clinical Characteristics of the Patients
The baseline clinical characteristics of the patients are displayed in Table 1. No significant differences in sex, age, weight, height, BMI, symptom duration, location of disease, and preoperative mHHS score were detected between the SCB and non-SCB groups.
Comparison of Clinical Data Between the SCB and Non-SCB Groups a
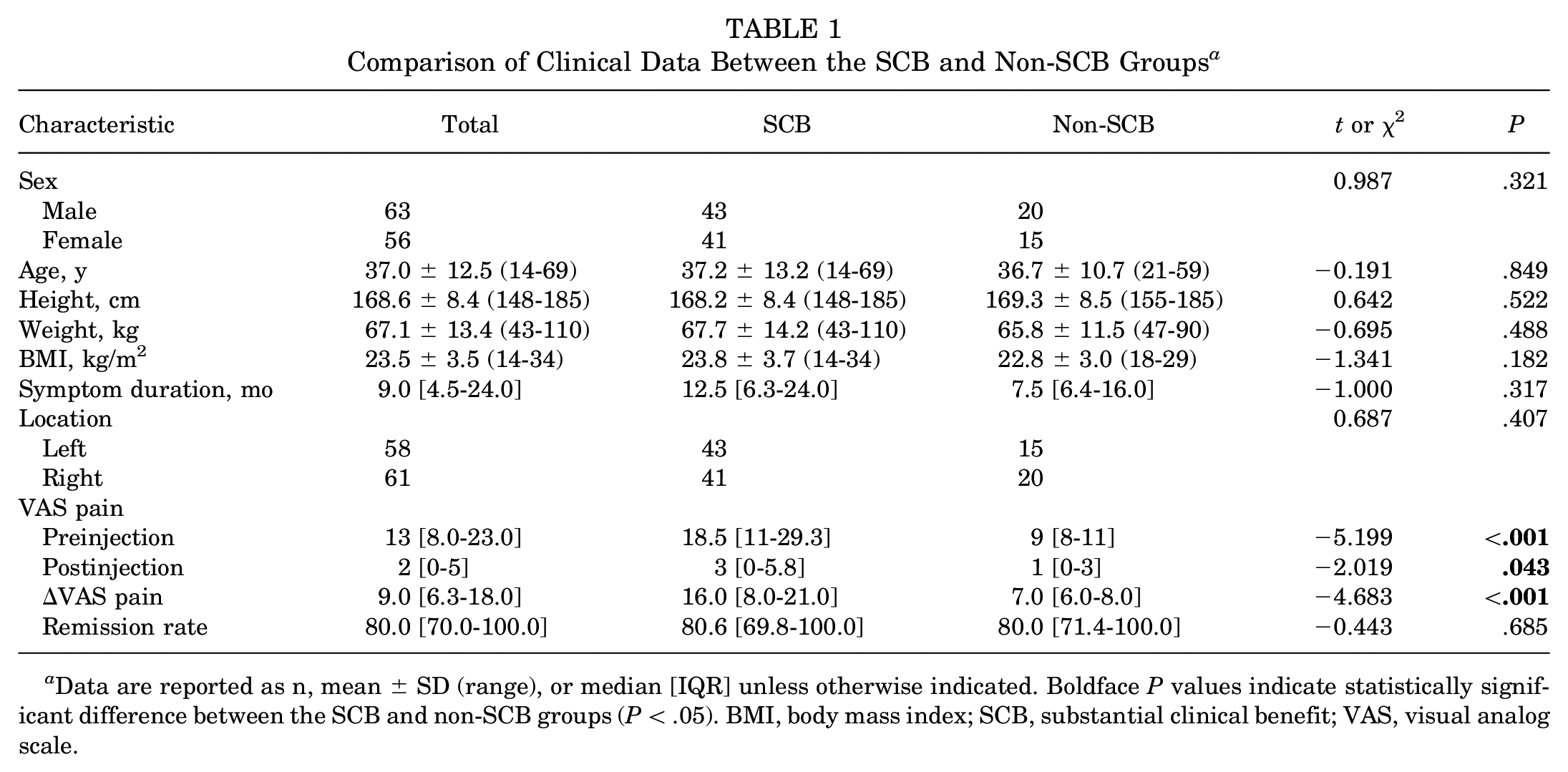
Data are reported as n, mean ± SD (range), or median [IQR] unless otherwise indicated. Boldface P values indicate statistically significant difference between the SCB and non-SCB groups (P < .05). BMI, body mass index; SCB, substantial clinical benefit; VAS, visual analog scale.
Outcomes After Hip Arthroscopy
For the entire cohort, there was a significant improvement in iHOT-12 scores after hip arthroscopy, from 46.8 ± 17.3 preoperatively to 78.4 ± 12.9 postoperatively (P < .001), with a difference of 31.6 ± 16.0 points. The mean mHHS scores also improved significantly, from 62.0 (IQR, 51.0-70.0) preoperatively to 87.0 (IQR, 80.0-91.0) postoperatively (P < .001), a difference of 20.0 points (IQR, 12.0-33.0 points). Overall, 84 patients (70.6%) achieved the SCB for the iHOT-12. Both the mHHS and iHOT-12 scores improved significantly after hip arthroscopy in both the SCB and the non-SCB subgroups (P < .001) (Table 2).
Comparison of iHOT-12 and mHHS Before and After Arthroscopy a
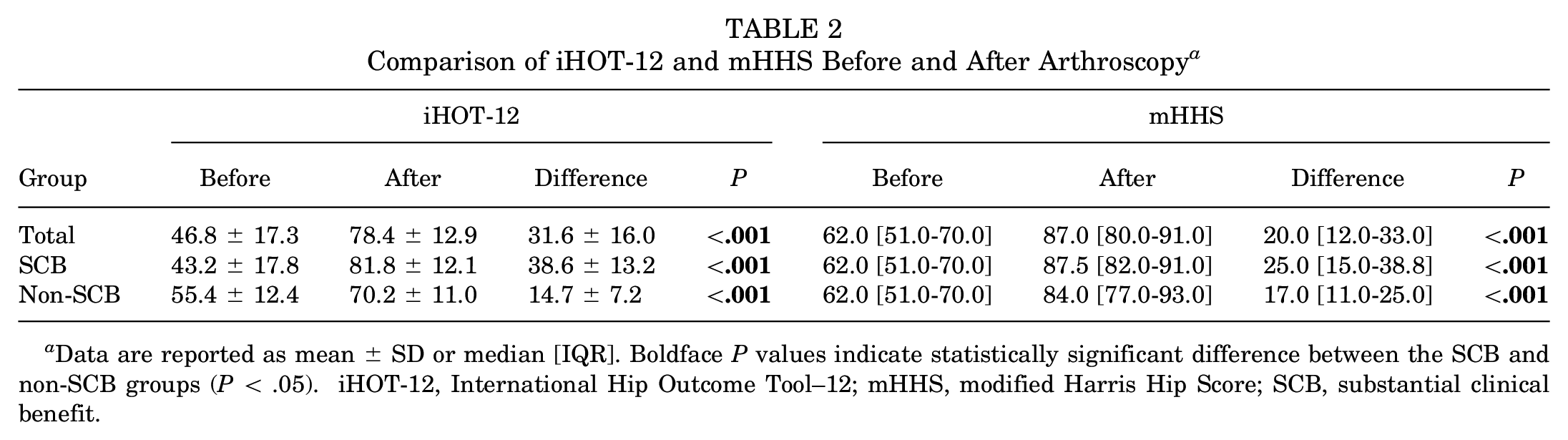
Data are reported as mean ± SD or median [IQR]. Boldface P values indicate statistically significant difference between the SCB and non-SCB groups (P < .05). iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; SCB, substantial clinical benefit.
VAS Pain After Injection
The total VAS pain score decreased (ie, improved) significantly, from 13.0 (IQR, 8.0-23.0) preinjection to 2.0 (IQR, 0-5.0) postinjection, with the median ΔVAS pain of 9.0 points (IQR, 6.3-18.0 points). In addition, VAS pain after hip injection significantly improved for the individual tests of internal rotation with the hip flexed 90°, external rotation with the hip flexed at 90°, hyperflexion, FADIR, and FABER tests. The discrepancies between the total pain score and these pain subscores were significantly greater in the SCB group when compared with the non-SCB group (P < .001, P = .001, P = .006, P = .006, P = .035, and P = .014, respectively). The VAS remission rate was also used as a predictor for SCB; however, the distinction of remission rate was not statistically significant (P = .685) (Table 1).
Binary Logistic Regression Analysis of SCB
Multivariate analysis showed that ΔVAS pain (P < .001) was a positive predictor of SCB, while a preoperative mHHS score was a negative predictor. The results of the binary logistic regression analysis are shown in Table 3.
Results of Binary Logistic Regression Analysis for Patients With SCB a

Dashes indicate multivariable analysis was not performed. Boldface P values indicate statistical significance (P < .05). FABER, flexion, abduction, external rotation; FADIR, flexion, abduction, internal rotation; OR, odds ratio; mHHS, modified Harris Hip Score; SCB, substantial clinical benefit; VAS, visual analog scale
Prediction of SCB After Hip Arthroscopy
To facilitate clinical application, we utilized a single value, ΔVAS pain, to predict SCB. The AUC, sensitivity, specificity, and accuracy were 0.772 (95% CI 0.687-0.858), 69.0% (58/84 participants), 85.7% (30/35 participants), and 73.9% (88/119 participants), respectively, with a cutoff value of 8.5 points. The multivariable logistic regression equation for SCB was as follows:

The AUC, sensitivity, specificity, and accuracy were 0.794 (95% CI, 0.713-0.875), 54.8% (46/84 participants), 97.1% (34/35 participants), and 67.2% (80/119 participants), respectively, with a cutoff value of 0.80 points. It was found that the diagnostic AUC of the multivariable logistic regression equation was not significantly different from that of the ΔVAS pain (P = .414).
We also found that when the total preinjection VAS pain score was >10, the binary logistic regression had the highest AUC of 0.834 (95% CI 0.676-0.992), with a sensitivity, specificity, and accuracy of 70.3% (45/64 participants), 90.0% (9/10 participants), and 73.0% (54/74 participants), respectively, at a cutoff value of 12.5 points. However, when the preinjection VAS pain score was ≤10, there was no significant change in the ΔVAS pain (Table 4 and Figure 3).
Prediction of SCB According to Binary Logistic Regression Formulas a
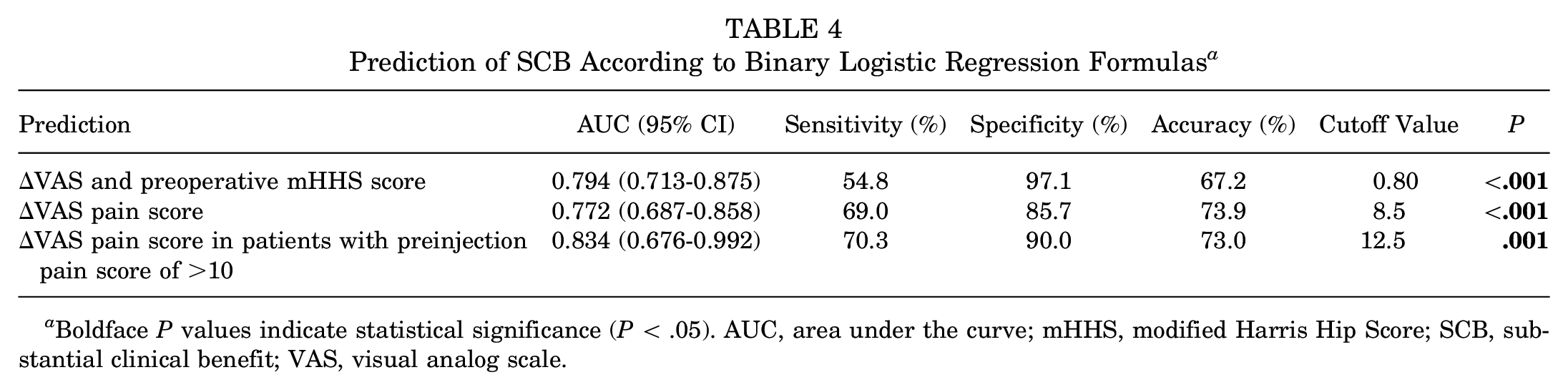
Boldface P values indicate statistical significance (P < .05). AUC, area under the curve; mHHS, modified Harris Hip Score; SCB, substantial clinical benefit; VAS, visual analog scale.

AUC of ΔVAS pain and preoperative mHHS scores in the prediction of SCB. (A) All patients. (B) AUC of ΔVAS pain score in patients with a preinjection VAS pain score of >10. AUC, area under the curve; mHHS, modified Harris Hip Score; Preop, preoperative; SCB, substantial clinical benefit; VAS, visual analog scale.
Discussion
In this study, ΔVAS pain after US-guided intra-articular hip injection was able to predict SCB in patients after hip arthroscopy for FAI. The ΔVAS pain score was significantly greater in the SCB versus the non-SCB groups (16.0 vs 7.0 points, respectively; P < .001). We determined that patients who experience a ΔVAS of >8.5 points after undergoing intra-articular hip injection would be able to achieve SCB after arthroscopy with an AUC of 0.772 (95% CI 0.687-0.858). For patients with more severe symptoms (eg, a preinjection VAS score of >10), a cutoff value of 12.5 points should be used.
Our results also showed that patients with preinjection VAS scores of >10 had better AUC (0.834 vs 0.772), sensitivity (70.3% vs 69.0%), and specificity (90.0% vs 85.7%) versus all patients. It suggests that patients with higher VAS pain scores before injection have better predictive values, which may due to the fewer uncertain factors. In addition, multivariate analysis showed that the ΔVAS pain was a positive predictor of SCB, while the mHHS score before hip arthroscopy was a negative predictor. The total ΔVAS and mHHS score before hip arthroscopy showed a high diagnostic specificity (97.1%), making them reliable exclusion indicators. This can help avoid unnecessary surgeries and improve clinical benefits for patients.
Although all enrolled patients were radiographically consistent with the FAI diagnosis, the outcome of arthroscopic treatment was different. The patients who did not see any significant improvement in pain (ie, a ΔVAS pain score of <8.5 points) might have had extra-articular pathology as the origin of pain, in which case hip arthroscopic treatment would be unnecessary.
The iHOT-12 is recommended for the evaluation of FAI treatment according to the Warwick Agreement. 16 According to the iHOT-12, the outcome of hip arthroscopy can be divided into 3 grades: minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and SCB.9,22 MCID is defined as the smallest perceptible change patients recognize as beneficial and is considered the lower threshold for clinical success. PASS is defined as the minimum score above which patients are satisfied with the state of their condition and is an intermediate between MCID and SCB. SCB refers to a difference between the preoperative and postoperative conditions that patients believe indicates significant improvement and represents an exceptionally excellent outcome. An increase in the iHOT-12 score of >28 was defined as SCB based on previous literature. 25 It is the ideal psychological expectation and the goal in terms of defining clinical success. In addition, SCB reflects the difference between the preoperative and postoperative conditions, which intuitively illustrates the benefits of arthroscopy. Therefore, this study used SCB achievement as the main outcome indicator.
Studies have focused on the prediction of hip arthroscopy outcomes. However, most clinical characteristics and imaging manifestations still lack accuracy 18 and objectivity. Intra-articular anesthetic injection was used to evaluate postoperative outcomes by Ayeni et al 1 in 2014. The mixture has an esthetic effect and can temporarily relieve the pain caused by intra-articular soft tissue injury. It can help patients return to the baseline activity state after injection, simulating the improvement of intra-articular pain in patients after hip arthroscopy. However, the predictive powers are relatively limited, without specific cutoff values. 1
In this study, the VAS pain score was used rather than the iHOT-12, mHHS, or other scales to evaluate the situation in the hip before and after injection because these scales include questions about function that cannot be assessed immediately after injection, such as the farthest walking distance, sexual ability, and pain level after activity. The VAS scale is easy to understand and operate. In addition, we used a combined VAS score of 7 standardized examination tests instead of separate static VAS scores to better reflect the functional status of the hip joint.
A series of standardized hip physical examination tests were performed. The FABER test is the most widely used hip provocation test, suggesting that the pain originates from the sacroiliac joint and lower lumbar facet joints, which has a sensitivity of 88% for identifying patients with labral tears. 17 Narvani et al 20 found that the internal rotation with the hip flexed at 90° was able to predict magnetic resonance arthrography–visible labral tears with a sensitivity of 75%. Hyperflexion suggests an intra-articular injury as well as a lesion at the acetabular labral junction. 6 Log roll test is only the movement of the femoral head relative to the acetabulum and joint capsule, and no pressure is exerted on the muscles, tendons, or nerve tissue. 3 Therefore, a positive log roll test indicates pathological damage to the acetabulum and labrum of the hip joint. It is highly specific in diagnosing FAI. However, a negative outcome from the test does not completely eliminate the possibility of hip joint pathology. In this study, our results showed the ΔVAS pain score of the log roll test was not significantly different between the SCB and non-SCB groups, which may be related to the limitation of sample size and the existence of the above-mentioned factors. In the future, we will expand the sample size and further explore the predictive ability of the log roll test on the outcome of hip arthroscopy.
The mHHS is used to assess the patient's basic functional status, which provides a comprehensive assessment of hip function after arthroscopy. A high preoperative mHHS score suggests that the patients’ basic functional status is still acceptable and that there is limited range for improvement by surgery. For such patients, nonoperative management may be more appropriate. In contrast, a low preoperative mHHS indicates that the patients with more severe symptoms could achieve satisfactory improvement after arthroscopy.
The authenticity results of intra-articular injection depend on a reliable injection method. US has been proven to be a safe, effective, and convenient tool, 14 which has the advantage of real-time visualization of the needle. In this study, the needle insertion pathway we used was from head to foot, which differed from traditional pathways. 8 The advantages of this pathway include a shorter needle pathway, better visualization of the needle, and better avoidance of the lateral circumflex femoral artery, which is critical to the blood supply of the femoral head.
Limitations
There were several limitations in the study. First, this study was carried out in a single center, and multicenter studies with larger sample volumes are warranted. Second, US-guided hip injection was performed and evaluated by the same sonographer. The prediction performance of different operators was not evaluated, and the learning curve needs to be further evaluated. Third, the surgical technique of the orthopaedic surgeon is also a key factor in determining the postoperative outcome, and in this study, the arthroscopy was performed by a senior orthopaedic surgeon in one center, and the multicenter application value of our model was not validated.
Conclusion
Improvement in pain after US-guided intra-articular hip injection predicted the outcomes of hip arthroscopy in patients with FAI in this study, especially for patients with more severe pain (total preinjection VAS pain score of >10 out of 70). It can provide indications for hip arthroscopy and help orthopaedists to make appropriate treatment decisions. Based on our results, we recommend an improvement in the preinjection-to-postinjection VAS pain score of 8.5 points as the cutoff for SCB prediction.
Footnotes
Final revision submitted July 20, 2023; accepted August 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Grants were received from the National Natural Science Foundation of China (82071924) and Youth Science Foundation of Chinese PLA General Hospital (22QNCZ041). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chinese PLA General Hospital (reference No. S2021-091-01).