
Abstract
Background:
Studies have correlated symptomatic femoroacetabular impingement (FAI) with femoral retroversion and cam lesions.
Purpose:
To investigate any association between femoral and acetabular versions with cam deformity in a largely asymptomatic population.
Study Design:
Descriptive laboratory study.
Methods:
A total of 986 cadaveric hips were selected from a historical osteologic collection. Each hip was assessed to determine the femoral and acetabular versions, anterior offset, and alpha angle. Cam morphology was defined as an alpha angle >60°. Multiple regression analysis was performed to determine the relationship between age, femoral version, acetabular version, and either alpha angle or anterior femoral offset.
Results:
The mean alpha angle and anterior offset for the sample population were 48.1°± 10.4° and 0.77 ± 0.17 cm, respectively, with cam morphology in 149 of the 986 (15.1%) specimens. No significant difference was observed between hips with and without cam morphology with respect to the femoral (10.8°± 10° vs 10.3°± 9.6°; P = .58) or acetabular versions (17.4°± 6° vs 18.2°± 6.3°; P = .14). Multiple regression analysis did not demonstrate an association between the femoral or acetabular versions and the alpha angle, and it showed a small association between the increasing femoral and acetabular versions and a decreased anterior femoral offset (both P < .01).
Conclusion:
In a large random sample of cadaveric hips, cam morphology was not associated with femoral or acetabular retroversion. Combined with the existing literature, these findings suggest that retroversion is not associated with cam development.
Clinical Relevance:
This study provides insight into the development of cam morphology, which may eventually aid in the evaluation and treatment of FAI.
Keywords
Cam morphology of the femoral neck has a reported prevalence of 15% in the asymptomatic population.13,15,19 While there are well-recognized causes of secondary cam morphology—including slipped capital femoral epiphysis (SCFE), Legg-Calves-Perthes disease, and posttraumatic changes—the cause of idiopathic cam morphology remains incompletely understood. 30 Some evidence supports an association between idiopathic cam morphology development during adolescence associated with vigorous sporting activity.3,33,40,41,46 Furthermore, while underlying hip morphology has been investigated as a risk factor for increased physeal shear stress and SCFE,10,12,37 limited data are available on the role of hip parameters in the development of cam deformity. Previous work investigating spinopelvic parameters associated with cam morphology has focused on pelvic incidence, alpha angle, and femoral neck-shaft angle.14,34,47 Specifically, cadaveric studies have associated a decreased pelvic incidence with cam morphology, theorizing compensation using an anterior pelvic tilt leading to dynamic acetabular over coverage and recurrent impingement.11,29,34,45
Relative femoral and acetabular retroversion have not been thoroughly investigated for their association with cam morphology. The femoral version is an essential hip parameter utilized throughout managing femoroacetabular impingement (FAI), especially during preoperative planning. Patients with symptomatic FAI have abnormal femoral version rates of up to 52%, with 17% of these abnormalities being severe.4,24 In addition, the acetabular version is abnormal in 31% of patients with FAI. 4 However, the question remains whether these parameters are associated with the initial development of the cam deformity or just the presence of impingement symptoms.
This study aimed to investigate the association between femoral and acetabular versions with cam deformity in a randomly sampled and presumably largely asymptomatic population. Based on previous smaller studies, we hypothesized that relative femoral retroversion would be associated with cam deformity.
Methods
Institutional review board approval was not required for this study. We utilized cadaveric specimens from the Hamann-Todd Osteologic Collection at the Cleveland Museum of Natural History. The collection contains approximately 3000 complete, disarticulated human skeletons collected between 1912 and 1938 with associated demographic information—including age and ethnicity. We randomly selected 986 paired pelvises and femora for measurement. Any specimens with evidence of gross deformity or pathology—eg, slipped capital femoral epiphysis, posttraumatic changes, significant degenerative changes, or Legg-Calves-Perthes disease—were excluded from the study. There were 2 time points where the specimens could be excluded: during the initial data collection and imaging due to gross deformity or by additional review of images. All exclusions were made by the senior resident (R.T.Y.) or an orthopaedic resident (W.Z.M.) doing a full-year research fellowship focused on osteology. Each specimen was then assessed to determine the acetabular version, femoral version, alpha angle, and anterior offset. The measurements were obtained from digital images generated from specimens positioned by the methods below and analyzed using ImageJ software (US National Institutes of Health).
Measurements
The acetabular version was measured in a standardized fashion after reconstructing the pelvises using a previously published method.23,28,42 The 2 hemipelves and sacrum were reassembled and secured using rubber bands with a uniform 12-mm piece of foam used to represent the pubic symphysis (Figure 1). After reassembly, the pelvis was gently positioned with the pubic crest and anterior superior iliac spines in contact with the laboratory table to reestablish the anatomic frontal plane of the pelvis.1,28 The central acetabular version could then be directly measured with a goniometer (Prestige Medical) as the angle formed between the laboratory table (representing the horizontal plane) and a line connecting the mid aspects of the anterior and posterior acetabulum (Figure 1).
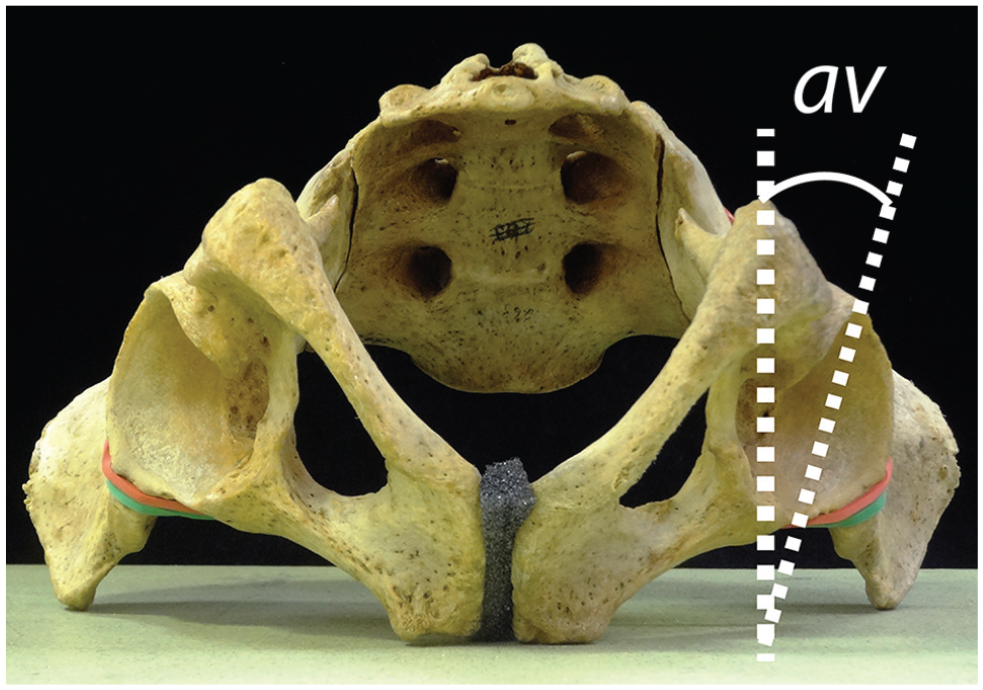
The central acetabular version (av) is defined as the complement of the angle formed between the laboratory table (representing the horizontal plane) and a line connecting the anterior and posterior ridges of the acetabulum.
Attention was then turned to the matching femora to measure the femoral version, alpha angle, and anterior offset. The femoral version was directly measured from specimens using the Kingsley-Olmsted method.21,26,44 Femora were positioned in a standardized anatomic position with the posterior femoral condyles and the greater trochanter resting on the table or elevated on blocks if there was femoral retroversion. The posterior aspects of the greater trochanter and posterior condyles defined the plane of the femur. A digital photograph of the femur was taken from a craniocaudal view, an oblique craniocaudal view angled perpendicular to the femoral neck. All images were processed, and angles were measured using Image J software.
The femoral version was measured as the angle formed between the plane of the femur (represented by the plane of the wood blocks) and the axis of the femoral neck (Figure 2A). The anterior offset and the alpha angle were measured based on modifications of the original methods described by Notzli et al.17,35,44 For anterior femoral offset, a line was drawn down the femoral neck axis, equidistant from the anterior and posterior borders of the femoral neck. Two lines were then drawn parallel to the femoral neck axis: the first line, tangential to the concavity of the anterior femoral neck, and the second, tangential to the convexity of the anterior femoral head. The anterior femoral offset was defined as the distance (in cm) of the perpendicular between these 2 lines (Figure 2B). A best-fit circle was placed over the femoral head to determine the alpha angle. The alpha angle was defined as the angle formed between the line representing the femoral neck axis and a line from the center of the best-fit circle on the femoral head to the point where the anterior cortical surface of the femoral head-neck junction first exits the best-fit circle (Figure 2C). For this study, specimens with an alpha angle >60° were considered to have a cam-type deformity.2,3

(A) Femoral version (fv) is defined as the angle formed between the plane of the full length of the femur (represented by the plane of the wood blocks) and the axis of the femoral neck. (B) The anterior femoral offset (afo) is determined based on 2 lines drawn parallel to the femoral neck axis: the first line, tangential to the concavity of the anterior femoral neck, and the second line, tangential to the convexity of the anterior femoral head. The anterior femoral offset (afo) is defined as the distance (in cm) of the perpendicular between these 2 lines.
Statistical Analysis
All statistical analyses were performed with SPSS (IBM). Interobserver agreement was determined for all variables measured in this study through the evaluation of 20 specimens by 2 authors (W.Z.M. and R.W.L.; an orthopaedic surgery resident and an attending physician); the specimens were remeasured by an additional author (R.T.Y., an orthopaedic surgery resident) to determine the intraclass correlation coefficient (ICC) for absolute agreement for each variable. Four weeks later, each of the 3 authors reevaluated the same 20 specimens to establish intrarater reliability (Table 1). The ICC values were interpreted as follows: <0.40 = poor; 0.40 to 0.59 = fair; 0.60 to 0.74 = good; and >0.74 = excellent.6,39
Intraclass Correlation Coefficients for Inter- and Intrarater Reliability (n = 20 Hips)

Two cohorts were created based on the presence of cam deformity (alpha angle >60°). Descriptive statistics were used to characterize the alpha angles, anterior offset, and femoral and acetabular versions of the hips with and without cam deformity. Femoral and acetabular versions were compared between these cohorts using the Student t test. Multiple regression analysis was also performed using age, femoral version, and acetabular version as independent variables with either alpha angle or anterior offset as the dependent variable. The level of significance for all tests was set at P < .05.
Results
The sample population comprised 685 of 986 (69.5%) White and 301 of 986 (30.5%) African American specimens. The 986 specimens demonstrated no evidence of gross deformity or pathology, including slipped capital femoral epiphysis, posttraumatic changes, significant degenerative changes, or Legg-Calves-Perthes disease. Specimens were predominantly men (840/986; 85.2%), with a mean age at death of 44.9 ± 15.2 years (range, 18-88 years).
The ICCs for each measurement demonstrated excellent agreement (Table 1). Regarding all specimens, the mean alpha angle and anterior offsets were 48.1°± 10.4° and 0.77 ± 0.17 cm, respectively. The mean femoral version was 10.4°± 9.6°, and the mean acetabular version was 18.1°± 6.3°, with a mean combined version of 28.5°± 11.5° (Table 2).
Measurements of Cadaveric Specimens (N = 986 Hips)

Using the definition of an alpha angle >60°, 149 of 986 (15.1%) specimens were found to have a cam deformity. There were no statistically significant differences between the cohorts with and without cam deformity with respect to the femoral version (10.8°± 10° vs 10.3°± 9.6°; P = .58), acetabular version (17.4°± 6° vs 18.2°± 6.3°; P = .14), or combined version (28.2°± 11.5° vs 28.5°± 11.5°; P = .95).
The results of the multiple regression analysis with the acetabular version, femoral version, and age as independent variables and the alpha angle or anterior offset as the dependent variable are depicted in Table 3. No statistically significant association was found between the femoral version, acetabular version, and alpha angle. Only increasing age demonstrated a significant association with increasing the alpha angle (P < .01). Multiple regression analysis showed a weak but significant association between increasing femoral and acetabular versions and decreased anterior offset (r = −0.283 and −0.083, respectively; P < .01).
Results of Regression Analyses of Femoral Version, Acetabular Version, and Age

Standardized (std) beta coefficients reflect how many SDs a dependent variable will change for every SD increase in the independent variable, allowing for a direct comparison of the relative effects of independent variables.
Unstandardized (unstd) beta coefficients reflect the mean change in the dependent variable with 1 unit of increase in the independent variable when other independent variables are controlled.
P < .01; P > .05 for the alpha angle vs the femoral and acetabular versions and for the anterior femoral offset vs age.
Discussion
The findings of our study demonstrate that acetabular and femoral retroversion are not associated with cam morphology in a large, asymptomatic population. Within the study, we found a 15.1% (149/986) prevalence of cam deformity. No statistically significant difference was observed between the 2 cohorts with and without cam deformity with respect to the mean femoral (10.8°± 10° vs 10.3°± 9.6°; P = .58) or acetabular version (17.4°± 6° vs 18.2°± 6.3°; P = .14). Multiple regression analysis further demonstrated that acetabular and femoral versions were not associated with the alpha angle. Notably, the use of multiple regression analysis allowed us to account for any linear effects of age, and thus, we evaluated the impact of femoral and acetabular versions on cam deformity parameters more objectively. The analysis did reveal a weak association between both increasing femoral and acetabular versions with decreased anterior offset (standardized β = −0.283; P < .01 and standardized β = −0.087; P < .01, respectively), which is opposite to the correlation noted in symptomatic populations.
As indicated by the lack of association within our study, idiopathic cam development is likely not driven by the presence of abnormal femoral or acetabular versions. Instead, growing evidence supports that idiopathic cam morphology develops during adolescence through the extension of the capital femoral epiphysis down the anterosuperior femoral neck and is associated with vigorous sporting activity.3,33,40,41 This cupping of the epiphysis around the femoral neck metaphysis is temporally associated with decreasing the relative size of the epiphyseal tubercle, a keystone like projection of the epiphysis in to the metaphysis, which provides intrinsic physeal stability.20,25,27,31,32,36,43 The additional stability provided by this cupping may be a physiologic adaptive response to resist physeal shear stress that would otherwise put the hip at risk for slipped capital femoral epiphysis.
Previous studies showing an association between cam deformity and relative femoral retroversion were performed mainly in smaller groups of symptomatic patients.8,17 Dall’Oca et al 8 reported on 21 patients with symptomatic FAI and found that those with cam impingement had relative femoral retroversion compared with norms in the published literature. Ito et al 17 investigated 24 patients with symptomatic FAI and reported relative femoral retroversion compared with 24 age-matched asymptomatic controls. Subsequent studies have highlighted that femoral retroversion is the main underlying factor for the decreased internal rotation observed in patients with FAI and cam-type deformities.5,22 There has also been controversy as to whether femoral retroversion is associated with poorer outcomes after arthroscopic femoral head-neck osteoplasty.9,16 However, there has been limited study of the association between femoral and acetabular versions with cam morphology in asymptomatic patients, possibly because of the challenges of imaging the distal femur to obtain femoral version measurements.
In a cadaveric study, Schaver et al 38 demonstrated that patients with cam deformities had more femoral anteversion and that the alpha angle was positively associated with increasing femoral anteversion. Their study had important methodological differences from the current paper. First, the femur was positioned resting on the proximal femoral shaft, rather than the greater trochanter as done in this study, which essentially extends the femoral neck and would be expected to decrease the version compared with our technique. Indeed, their mean version was 8.5° versus 10.4° in our study. Second, they measured the alpha angle on an axial view, where it is more difficult to visualize, while we utilized a view that more closely approximates the position used to clinically measure the alpha angle as originally described by Notzli et al. 22 Third, they did not account for demographic characteristics, while our study noted an association between the alpha angle and age and was able to adjust for it in the multiple regression analysis. Finally, only our study additionally accounts for the acetabular version, which allows for the consideration of the combined version of the femur and acetabulum.
In addition to the alpha angle, we also utilized another marker of cam deformity, decreased anterior femoral offset, 7 to investigate for possible associations with femoral or acetabular retroversion. Multiple regression analysis revealed a small but significant association between increases in femoral or acetabular versions and decreasing anterior offset (P < .01 for both). When beta coefficients were standardized, it was also revealed that the anterior offset had a much larger association with the femoral version than the acetabular version. This data suggested that increasing version is associated with cam deformity based on a decreased anterior offset and merits further clinical investigation. However, the more important finding is the absence of an association between retroversion and cam-type deformity.
We believe that the findings of no association between femoral and acetabular versions with cam morphology defined by the alpha angle contrast with the limited existing clinical literature because of our use of a random sample population, which is largely asymptomatic. Our data suggest that morphologic parameters for mechanical hip impingement, such as femoral and acetabular retroversion, do not increase the risk of cam morphology. Instead, we believe that relative femoral or acetabular retroversion increases the risk that existing cam morphology will become symptomatic by decreasing the range of motion before impingement (Figure 3).

The absence of association between cam deformity and relative femoral/acetabular retroversion in this largely asymptomatic sample population suggests that the development of idiopathic cam morphology is not significantly influenced by relative retroversion. Instead, we propose that relative retroversion increases the risk that idiopathic cam deformity becomes symptomatic, as patients are more likely to mechanically impinge. Please also note that relative retroversion may be a risk factor for symptomatic disease, but we do not consider it a requirement.
Limitations
There are limitations to our study, primarily stemming from the use of a historical cadaveric collection. Although this collection provided us a unique opportunity for direct measurement of femoral and acetabular versions that would otherwise be difficult to obtain, the lack of clinical data requires assumptions to be made about the prevalence of hip pain in this population. Although we cannot confirm the absence of hip pain in each of the specimens during life, the Hamann-Todd Collection essentially represents a random sample population from the Cleveland, Ohio, area during the early 20th century, and we believe that it is a reasonable assumption that most of the specimens came from asymptomatic patients, similar to any random sample population. Furthermore, the incidence of cam deformity of 15.2% in our study is consistent with previous studies of asymptomatic populations.13,15 However, given that this study population is from the 20th century, the applicability to cam development in more contemporary populations may be limited. The osteologic collection is limited to White and African American cadaveric specimens. Therefore, conclusions cannot be drawn regarding other racial groups. Disarticulated cadaveric specimens also present a risk for inaccuracy during the required reassembly of the pelvis to measure the acetabular version. To limit the risk of inaccuracy, we utilized a previously published, standardized technique for reassembly of the sacrum and hemipelvis,23,28,42 resulting in mean acetabular version measurements that were similar to the population norms of approximately 18 15° to 20° degrees.
Conclusion
In a large random sample population, cam morphology was not associated with femoral or acetabular retroversion. Combined with the existing literature, these findings suggest that retroversion is not associated with cam development. This study provides insight into the development of cam morphology, which may eventually aid in the evaluation and treatment of FAI. Further studies are needed to confirm these findings in a clinical setting. A more thorough understanding of the cause of cam deformity and the risk factors for symptomatic disease may improve the evaluation of patients with FAI and the selection of patients for intervention.
Footnotes
Acknowledgements
The authors thank Lyman Jellema, former collections manager at the Cleveland Museum of Natural History, for his assistance and expertise in navigating the Hamann Todd Osteological Collection.
Final revision submitted June 6, 2023; accepted July 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.T.Y. has received a grant from NuVasive; education payments from Medical Device Business Services; and hospitality from Alphatec Spine, Globus Medical, Medacta, and Medtronic. K.X. has received education payments from Fortis Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.