
Abstract
Background:
Osteochondral injuries (OCIs) are common in patients with acute lateral patellar dislocation, which can produce both short- and long-;term adverse effects. However, the pattern of these injuries warrants further analysis, especially in relation to patient age.
Purpose:
To determine the overall prevalence of concomitant OCIs as well as the prevalence differences based on location and age after acute lateral patellar dislocations.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A comprehensive search of PubMed, Embase, Web of Science, and Cochrane Library was completed from inception to July 20, 2022. All articles reporting the prevalence of OCI were included. The sample characteristics such as age, study design, magnetic resonance imaging diagnostic data, and the number of patients with OCI were extracted. The Methodological Index for Non-Randomized Studies (MINORS) was used for quality assessment. The overall and per-;site injury rates were calculated, and the prevalence was stratified by age-;group (≤16 and >16 years) and compared.
Results:
The systematic review included 39 studies involving 3354 patients. MINORS scores were 11.94 ± 1.98 and 16 ± 3.46 in the noncomparative and comparative studies, respectively. The overall prevalence of bone bruises and OCI was 89.6% (95% CI, 77.4%-97.7%) and 48.8% (95% CI, 39.0%-58.7%), respectively. In both overall and >16-year-old patients, the lateral femoral condyle (LFC) was the most common site of bone bruise (90.5% [95% CI, 84.0%-95.6%] and 91.5% [95% CI, 84.3%-96.9%], respectively); however, the medial patellar bruise was more common in patients ≤16 years (89.2% [95% CI, 82.9%-94.4%]). Among the pooled sites of OCI, the medial patella accounted for the largest proportion (36.9% [95% CI, 28.0%-46.3%]). OCIs were more common in patients >16 years (52.6% [95% CI, 39.4%-65.6%]) than in patients ≤16 years (46.6% [95% CI, 33.2%-60.3%]).
Conclusion:
Bone bruises on the LFC were most prevalent overall and in patients >16 years, whereas bone bruises on the medial patella were more prevalent in patients ≤16 years. OCIs were frequently seen in patients >16 years, with the most common site being the medial patella.
Acute lateral patellar dislocation is a common injury in young and active patients, especially in females, with an incidence of approximately 23 to 42 per 100,000 cases, accounting for 2% to 3% of knee injuries.12,18,21,30 The annual risk of patellar dislocation in the second and third decades of life is 29 and 9 per 100,000, respectively.15,46 Medial patellofemoral ligament (MPFL) injury and osteochondral injury (OCI) are common after patellar dislocation, and the presence of these defects has an impact on both short- and long-;term outcomes.8,11,13,20,26,33,56
The reported prevalence of these injuries varies widely, and it is also unclear whether there are age-;related differences. Recently, a systematic review reported the overall incidence of MPFL injuries as 94.7%, 24 yet detailed information on the prevalence and location of OCIs in relation to age is still lacking.
The purpose of this study was to systematically review the current literature to determine the prevalence of OCI after acute lateral patellar dislocation, the most common location, and whether there were age-;related differences in these injuries.
Methods
This systematic review and meta-;analysis were carried out following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 28 This research protocol was registered on PROSPERO (International Prospective Register of Systematic Reviews) (CRD42022298944).
Literature Search and Strategy
A comprehensive electronic search of PubMed, Embase, Web of Science, and the Cochrane Library was conducted from inception to July 20, 2022. The terms “patellar,”“dislocation,*”“instability,”“primary,”“acute,”“first,”“initial,”“bone bruise,*”“osteochondral,”“cartilage,*”“injury,”“lesion,*”“damage,*” and “fracture*” were combined using Boolean logic. A supplementary search of the reference lists of identified articles was also a strategy.
Eligibility Criteria
The inclusion criteria were studies written in English that evaluated patients with acute lateral patellar dislocation and reported the prevalence of OCI on magnetic resonance imaging (MRI). We excluded studies that had patients with congenital or recurrent patellar dislocations, those not reporting MRI findings duplicate studies or studies with data that could not be extracted, and animal studies and cadaveric studies.
Study Selection
All obtained articles were imported into Endnote (Clarivate Analytics) for de-;duplication and further management of the remaining articles. Two reviewers (Z.Y. and J.J.) independently identified the eligibility of studies based on the inclusion criteria. In the case of disagreement between the 2 reviewers, the consensus decision-;making process was enabled by the participation of the third reviewer (J.L.).
Quality Assessment and Level of Evidence
Quality assessment and grading of the level of evidence were performed independently by 2 reviewers (Z.Y. and J.J.). Methodological quality was assessed using the methodological index for nonrandomized studies (MINORS). 44 Any disagreements were resolved by consulting a third reviewer (Y.C.).
Data Collection
Relevant data were extracted independently by the 2 authors mentioned above, and a third author (B.G.) was consulted to resolve any discrepancies. The following data were entered into predesigned tables: first author, time of publication, country, study design, sample characteristics (age and sex), sample size, method of diagnosing the injury, number of patients with OCIs, and different injury sites. Although bone bruises are a mild type of OCI, given the characteristics of the raw data and the overall logic of the full text, bone bruises were finally analyzed separately in this study.
Statistical Analysis and Data Processing
The proportions of each injury type were pooled. In addition, the prevalence of each injury type was further analyzed by subgroups of sites and age. The age subgroups were divided into ≤16 years and >16 years groups according to the criteria of previous study. 24 Meta-analyses were performed with Stata software (Version 14.0; Stata). Event rates and relative 95% CIs were calculated.
Results
Search Results
The electronic search yielded a total of 498 publications, and an additional 10 publications were gained by manually searching the references of relevant articles. After removing duplicate publications (n = 151), the titles and abstracts were read according to the inclusion and exclusion criteria for further selection. The full text of the remaining 66 publications was examined carefully, and 39 studies met the inclusion scope (Figure 1).

Flowchart of the literature searching and screening process. OCI, osteochondral injury; MRI, magnetic resonance imaging.
Study Characteristics
Detailed information is shown in Appendix Table A1. A total of 3354 patients (mean age, 19.56 ± 4.28 years; 44.6% male) were included in the study. In all, 15 studies ‡ (n = 1080 knees) examined the incidence of bone bruises, and 38 studies § (n = 3329 knees) reported the prevalence of OCI. All were observational studies, with 9 cohort studies, ‖ 4 case-;control studies,6,13,19,42 and 26 case series. ¶ In addition, 11 studies # (28%) reported outcomes for patients with a mean age ≤16 years, and 28 studies** (72%) reported outcomes for patients with a mean age >16 years; age was not available for 2 studies (5%).19,28 Most of the included studies were of level 4 evidence (67%), followed by level 3 (18%) and level 2 (15%). MINORS scores were 11.94 ± 1.98 and 16 ± 3.46 in the noncomparative and comparative studies, respectively.
Prevalence of Bone Bruises After Acute Lateral Patellar Dislocation
The overall pooled prevalence of bone bruises was 89.6% (95% CI, 77.4%-97.7%) (Figure 2), and the prevalence in patients with a mean age ≤16 years versus those with a mean age >16 years was 82.6% (95% CI, 71.8%-91.3%), and 89.8% (95% CI, 74.0%-99.2%), respectively (Supplemental Figures S1-S2, available separately). The prevalence of bone bruises at various sites was analyzed in our study. Bone bruises were most frequently seen in the lateral femoral condyle (LFC) (90.5% [95% CI, 84.0%-95.6%]), followed by medial patella (59.7% [95% CI, 43.9%-74.7%]), lateral patella (17.4%), medial femoral condyle (7.5% [95% CI, 1.5%-16.7%]), lateral tibial plateau (2.5% [95% CI, 0.1%-6.8%]), and medial tibial plateau (2.4%) (Supplemental Figures S3-S6). Further age subgroup analysis revealed that the prevalence of medial patellar bruises in patients with a mean age ≤16 years and those with a mean age >16 years was 89.2% (95% CI, 82.9%-94.4%), 57.5 (95% CI, 41.0%-73.3%), respectively; and the prevalence of bruises in LFC in patients with mean age ≤16 years and those with mean age >16 years was 84.9% (95% CI, 77.8%-90.9%) and 91.5% (95% CI, 84.3%-96.9%), respectively (Supplemental Figures S7-S10).

Forest plot depicting the overall prevalence of bone bruises. ES, effect size.
Prevalence of OCI After Acute Lateral Patellar Dislocation
The overall pooled prevalence of OCI was 48.8% (95% CI, 39.0%-58.7%) (Figure 3). Additionally, the prevalence of OCI in patients with a mean age ≤16 years and in patients >16 years was 46.6% (95% CI, 33.2%-60.3%) and 52.6% (95% CI, 39.4%-65.6%), respectively (Supplemental Figures S11 and S12, available separately). In terms of specific injury sites, the prevalence of medial patella was the highest (36.9% [95% CI, 28.0%-46.3%]), followed by central patella (23.7% [95% CI, 5.3%-49.0%]), LFC (20.6% [95% CI, 13.1%-29.2%]), and lateral patella (12.6% [95% CI, 2.6%-27.3%]) (Supplemental Figures S13-S16). In studies with a mean patient age ≤16 years, the prevalence of OCI was 19.5% (95% CI, 8.3%-33.8%) at the LFC and 29.7% (95% CI, 24.9%-34.7%) at the medial patella (Supplemental Figures S17 and S18). In studies with a mean patient age >16 years, the prevalence of OCI was 22.4% (95% CI, 13.0%-33.3%) at the LFC and 40.8% (95% CI, 30.7%-51.4%) at the medial patella (Supplemental Figures S19 and S20).

Forest plot depicting the overall prevalence of osteochondral injuries. ES, effect size.
Discussion
The systematic review found that the overall prevalence of bone bruises and OCI was 89.6% and 48.8%, respectively. Bone bruises of the LFC were the most common overall (90.5%) and in patients >16 years (91.5%), while the medial patellar bruise was more common in those ≤16 years (89.2%). OCI occurred most frequently in the medial patella (36.9%) and was more prevalent in patients >16 years (52.6%).
In this study, the prevalence of bone bruises in the LFC and medial patella were as high as 90.5% and 59.7%, respectively, which may explain why they can be one of the relatively accepted diagnostic criteria for acute lateral patellar dislocation.2,45 Patients with a mean age ≤16 years had a high prevalence of medial patellar bruises, whereas those >16 years had a high prevalence of bone bruises at the LFC. Only 1 study investigated the prevalence of bone bruises in both children and adults with acute patellar dislocation and found that medial patellar bruise was common in both children (91%) and adults (93%); however, the sample size was small and may not be representative of all patients. 58 In terms of the clinical importance of bone bruises, Davies et al 10 found the initial size or persistence of the bone bruises to be uncorrelated with the presence/absence or type of associated injury. Boks et al 9 concluded that no statistically significant relationship was found between the existence of bone bruises and pain severity, and no clinical correlation was found. However, Paakkala et al 29 speculated that significant bone bruises may result in potential loss of cartilage nutrition and irreversible microstructural injuries, leading to osteochondral loss.
The present study also confirmed a relatively high prevalence of OCI after acute lateral patellar dislocation. The broad category of OCIs in this study included cartilage damages, fractures, or loose bodies, which may have contributed to its high prevalence. 8 We found that the sites prone to OCI are the medial patella, central patella, and LFC, which is in accordance with a previous study. 50 Based on the patellofemoral motion pattern during acute dislocation, the shearing mechanism can lead to lateral displacement of the patella, resulting in patellofemoral joint injuries. When the patella is repositioned, the concave structure of the trochlear groove protects its articular surface from damage during patellar resetting, whereas the convex shape of the patella puts its articular cartilage at risk of injury during repositioning.34,47,56 Therefore, the patella is at dual risk of shear or impaction injury during dislocation and repositioning, whereas the femoral articular surface is only at-;risk during dislocation, which might explain the higher prevalence of patellar injury.
Notably, our further subgroup analysis of patients ≤16 years revealed that OCIs were more likely to appear at the medial patella compared with the LFC, which may be related to the later ossification process of the medial patella than the distal femur. 59 In children and adolescents, external forces could easily affect this chondro-;osseous boundary, leading to avulsion fractures of the patellar boundary, which further enriches the theoretical basis for the above findings. 14
However, OCI of the medial patella and LFC was more likely to occur in patients >16 years compared with those ≤16 years. The reasons for this phenomenon are likely multifaceted, which may be closely related to the anatomy of the patellofemoral joint and the MPFL and the vastus medialis oblique muscle. The anatomy of the patellofemoral joint in adolescents is not fully developed and perfect, and the MPFL and the internal oblique femoral muscle are not fully fused.55,58,59
Consequently, the patellofemoral joint in adolescents is relatively less stable, less force is required for acute dislocation, and collision and compression between the patella and LFC would be relatively less. In addition, Tompkins et al 48 explained that the more remarkable plasticity of tissue in skeletally immature patients is also one of the reasons for fewer OCIs.
It has also been suggested that the prevalence of OCI is associated with specific anatomic factors. For example, patellar dislocation in patients with a normal femoral trochlea, resulting in a higher prevalence of OCI due to its greater outward traction and retraction forces.49,60 The prevalence of OCI in the medial patella and LFC may be higher in complete MPFL injuries compared with partial MPFL injuries.55,56 Moreover, Zheng et al 58 also found a higher prevalence of patellofemoral injuries in men, especially in the patella, presumably related to greater compression and impact intensity of the patellofemoral joint in men. Comparing the prevalence and location of OCIs between male and female patients could be a focus of future research to further investigate whether sex-;specific injury patterns exist in patellar dislocation.
The results of this study should be interpreted in view of several limitations. First, the lack of uniformity in the definitions and diagnostic criteria for OCI in some of the original studies, as well as the imprecise description of isolated fractures, may interfere with the prevalence statistics. Second, the study did not include those data confirmed by other methods (sonography or surgery), so the results only apply to cases confirmed by MRI. Third, study quality was not an exclusion criterion, such that large heterogeneity may have contributed to differences in prevalence estimates. For example, some studies reported only crude prevalence, while others reported only sites or age-;adjusted prevalence. Future studies should validate our results in larger-;scale investigations.
Conclusion
Bone bruises on the LFC were most prevalent overall and in patients >16 years, whereas bone bruise on the medial patella was more prevalent in patients ≤16 years. Additionally, OCIs were frequently seen in patients >16 years, with the most common site being the medial patella.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231220904 – Supplemental material for Prevalence and Site of Concomitant Osteochondral Injuries in Patients With Acute Lateral Patellar Dislocation: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231220904 for Prevalence and Site of Concomitant Osteochondral Injuries in Patients With Acute Lateral Patellar Dislocation: A Systematic Review and Meta-analysis by Zhi Yi, Jin Jiang, Jinmin Liu, Ming Ma, Yi Chen, Fei Teng, Ao Yang, Zhongcheng Liu, Bin Geng, Yayi Xia and Meng Wu in Orthopaedic Journal of Sports Medicine
Footnotes
Appendix
Characteristics of the Included Studies a
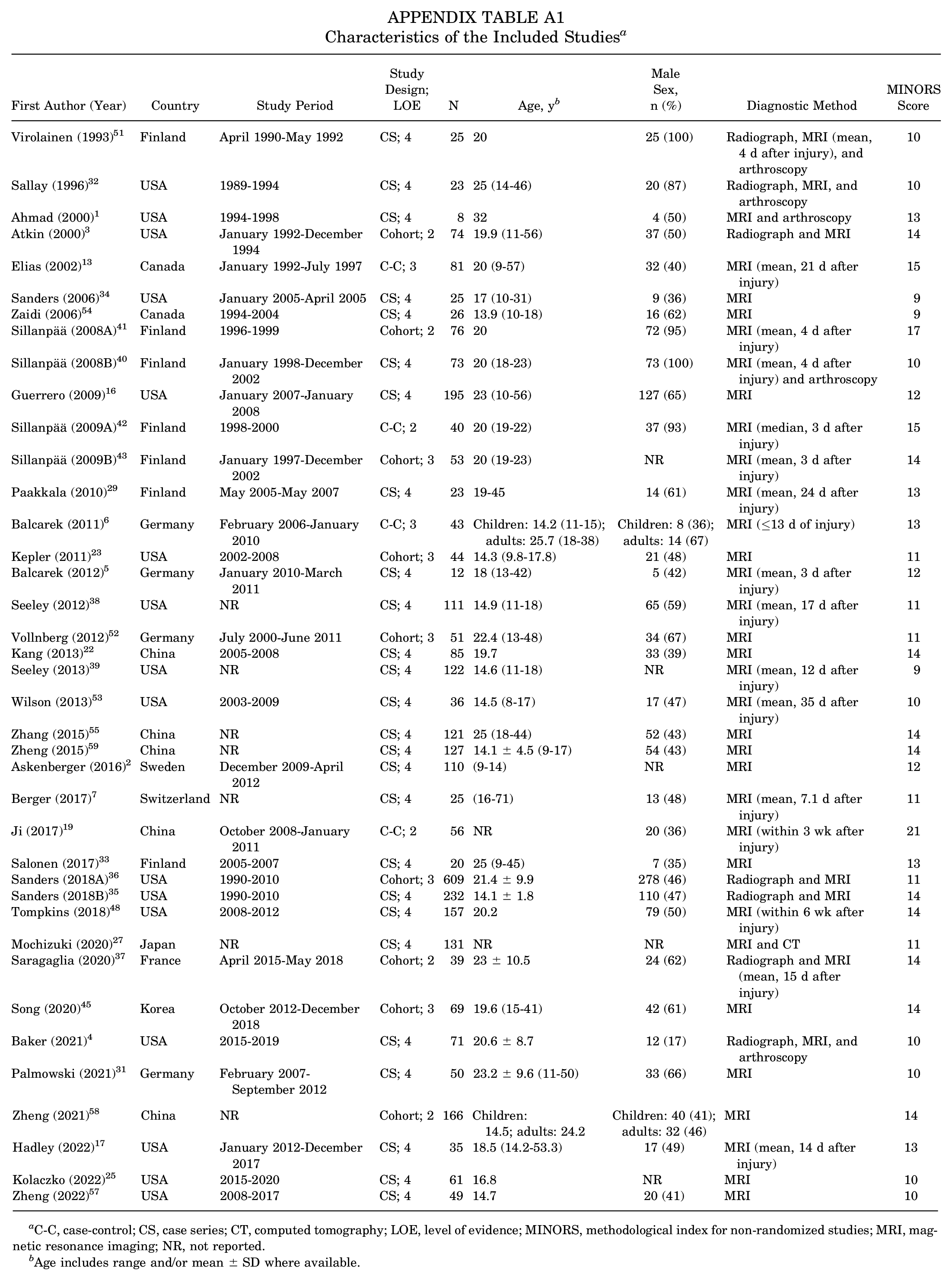
| First Author (Year) | Country | Study Period | Study Design; LOE | N | Age, y b | Male Sex, n (%) | Diagnostic Method | MINORS Score |
|---|---|---|---|---|---|---|---|---|
| Virolainen (1993) 51 | Finland | April 1990-May 1992 | CS; 4 | 25 | 20 | 25 (100) | Radiograph, MRI (mean, 4 d after injury), and arthroscopy | 10 |
| Sallay (1996) 32 | USA | 1989-1994 | CS; 4 | 23 | 25 (14-46) | 20 (87) | Radiograph, MRI, and arthroscopy | 10 |
| Ahmad (2000) 1 | USA | 1994-1998 | CS; 4 | 8 | 32 | 4 (50) | MRI and arthroscopy | 13 |
| Atkin (2000) 3 | USA | January 1992-December 1994 | Cohort; 2 | 74 | 19.9 (11-56) | 37 (50) | Radiograph and MRI | 14 |
| Elias (2002) 13 | Canada | January 1992-July 1997 | C-C; 3 | 81 | 20 (9-57) | 32 (40) | MRI (mean, 21 d after injury) | 15 |
| Sanders (2006) 34 | USA | January 2005-April 2005 | CS; 4 | 25 | 17 (10-31) | 9 (36) | MRI | 9 |
| Zaidi (2006) 54 | Canada | 1994-2004 | CS; 4 | 26 | 13.9 (10-18) | 16 (62) | MRI | 9 |
| Sillanpää (2008A) 41 | Finland | 1996-1999 | Cohort; 2 | 76 | 20 | 72 (95) | MRI (mean, 4 d after injury) | 17 |
| Sillanpää (2008B) 40 | Finland | January 1998-December 2002 | CS; 4 | 73 | 20 (18-23) | 73 (100) | MRI (mean, 4 d after injury) and arthroscopy | 10 |
| Guerrero (2009) 16 | USA | January 2007-January 2008 | CS; 4 | 195 | 23 (10-56) | 127 (65) | MRI | 12 |
| Sillanpää (2009A) 42 | Finland | 1998-2000 | C-C; 2 | 40 | 20 (19-22) | 37 (93) | MRI (median, 3 d after injury) | 15 |
| Sillanpää (2009B) 43 | Finland | January 1997-December 2002 | Cohort; 3 | 53 | 20 (19-23) | NR | MRI (mean, 3 d after injury) | 14 |
| Paakkala (2010) 29 | Finland | May 2005-May 2007 | CS; 4 | 23 | 19-45 | 14 (61) | MRI (mean, 24 d after injury) | 13 |
| Balcarek (2011) 6 | Germany | February 2006-January 2010 | C-C; 3 | 43 | Children: 14.2 (11-15); adults: 25.7 (18-38) | Children: 8 (36); adults: 14 (67) | MRI (≤13 d of injury) | 13 |
| Kepler (2011) 23 | USA | 2002-2008 | Cohort; 3 | 44 | 14.3 (9.8-17.8) | 21 (48) | MRI | 11 |
| Balcarek (2012) 5 | Germany | January 2010-March 2011 | CS; 4 | 12 | 18 (13-42) | 5 (42) | MRI (mean, 3 d after injury) | 12 |
| Seeley (2012) 38 | USA | NR | CS; 4 | 111 | 14.9 (11-18) | 65 (59) | MRI (mean, 17 d after injury) | 11 |
| Vollnberg (2012) 52 | Germany | July 2000-June 2011 | Cohort; 3 | 51 | 22.4 (13-48) | 34 (67) | MRI | 11 |
| Kang (2013) 22 | China | 2005-2008 | CS; 4 | 85 | 19.7 | 33 (39) | MRI | 14 |
| Seeley (2013) 39 | USA | NR | CS; 4 | 122 | 14.6 (11-18) | NR | MRI (mean, 12 d after injury) | 9 |
| Wilson (2013) 53 | USA | 2003-2009 | CS; 4 | 36 | 14.5 (8-17) | 17 (47) | MRI (mean, 35 d after injury) | 10 |
| Zhang (2015) 55 | China | NR | CS; 4 | 121 | 25 (18-44) | 52 (43) | MRI | 14 |
| Zheng (2015) 59 | China | NR | CS; 4 | 127 | 14.1 ± 4.5 (9-17) | 54 (43) | MRI | 14 |
| Askenberger (2016) 2 | Sweden | December 2009-April 2012 | CS; 4 | 110 | (9-14) | NR | MRI | 12 |
| Berger (2017) 7 | Switzerland | NR | CS; 4 | 25 | (16-71) | 13 (48) | MRI (mean, 7.1 d after injury) | 11 |
| Ji (2017) 19 | China | October 2008-January 2011 | C-C; 2 | 56 | NR | 20 (36) | MRI (within 3 wk after injury) | 21 |
| Salonen (2017) 33 | Finland | 2005-2007 | CS; 4 | 20 | 25 (9-45) | 7 (35) | MRI | 13 |
| Sanders (2018A) 36 | USA | 1990-2010 | Cohort; 3 | 609 | 21.4 ± 9.9 | 278 (46) | Radiograph and MRI | 11 |
| Sanders (2018B) 35 | USA | 1990-2010 | CS; 4 | 232 | 14.1 ± 1.8 | 110 (47) | Radiograph and MRI | 14 |
| Tompkins (2018) 48 | USA | 2008-2012 | CS; 4 | 157 | 20.2 | 79 (50) | MRI (within 6 wk after injury) | 14 |
| Mochizuki (2020) 27 | Japan | NR | CS; 4 | 131 | NR | NR | MRI and CT | 11 |
| Saragaglia (2020) 37 | France | April 2015-May 2018 | Cohort; 2 | 39 | 23 ± 10.5 | 24 (62) | Radiograph and MRI (mean, 15 d after injury) | 14 |
| Song (2020) 45 | Korea | October 2012-December 2018 | Cohort; 3 | 69 | 19.6 (15-41) | 42 (61) | MRI | 14 |
| Baker (2021) 4 | USA | 2015-2019 | CS; 4 | 71 | 20.6 ± 8.7 | 12 (17) | Radiograph, MRI, and arthroscopy | 10 |
| Palmowski (2021) 31 | Germany | February 2007-September 2012 | CS; 4 | 50 | 23.2 ± 9.6 (11-50) | 33 (66) | MRI | 10 |
| Zheng (2021) 58 | China | NR | Cohort; 2 | 166 | Children: 14.5; adults: 24.2 | Children: 40 (41); adults: 32 (46) | MRI | 14 |
| Hadley (2022) 17 | USA | January 2012-December 2017 | CS; 4 | 35 | 18.5 (14.2-53.3) | 17 (49) | MRI (mean, 14 d after injury) | 13 |
| Kolaczko (2022) 25 | USA | 2015-2020 | CS; 4 | 61 | 16.8 | NR | MRI | 10 |
| Zheng (2022) 57 | USA | 2008-2017 | CS; 4 | 49 | 14.7 | 20 (41) | MRI | 10 |
C-C, case-control; CS, case series; CT, computed tomography; LOE, level of evidence; MINORS, methodological index for non-;randomized studies; MRI, magnetic resonance imaging; NR, not reported.
Age includes range and/or mean ± SD where available.
Final revision submitted June 20, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the National Natural Science Foundation of China (81874017, 81960403, and 82060405); Lanzhou Science and Technology Plan Program (2021-RC-102); Natural Science Foundation of Gansu Province (22JR5RA943, 22JR5RA956); and the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2020-BJ03, CY2021-MS-B02, and CY2021-MS-A07). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.