
Abstract
Background:
One proposed mechanism of rotator cuff disease is scapular motion impairments contributing to rotator cuff compression and subsequent degeneration.
Purpose:
To model the effects of scapular angular deviations on rotator cuff tendon proximity for subacromial and internal mechanical impingement risk during scapular plane abduction.
Study Design:
Descriptive laboratory study.
Methods:
Three-dimensional bone models were reconstructed from computed tomography scans obtained from 10 asymptomatic subjects and 9 symptomatic subjects with a clinical presentation of impingement syndrome. Models were rotated to average scapular orientations from a healthy dataset at higher (120°) and lower (subject-specific) humeral elevation angles to investigate internal and subacromial impingement risks, respectively. Incremental deviations in scapular upward/downward rotation, internal/external rotation, and anterior/posterior tilt were imposed on the models to simulate scapular movement impairments. The minimum distance between the rotator cuff insertions and potential impinging structures (eg, glenoid, acromion) was calculated. Two-way mixed-model analyses of variance assessed for effects of scapular deviation and group.
Results:
At 120° of humerothoracic elevation, minimum distances from the supraspinatus and infraspinatus insertions to the glenoid increased with ≥5° changes in upward rotation (1.6-9.8 mm, P < .001) or external rotation (0.9-5.0 mm, P≤ .048), or with ≥10° changes in anterior tilt (1.1-3.2 mm, P < .001). At lower angles, ≥20° changes in most scapular orientations significantly increased the distance between the supraspinatus and infraspinatus insertions and the acromion or coracoacromial ligament.
Conclusion:
A reduction in scapular upward rotation decreases the distance between the rotator cuff tendon insertions and glenoid at 120° humerothoracic elevation. Interpretation is complicated for lower angles because the humeral elevation angle was defined by the minimum distance.
Clinical Relevance:
These results may assist clinical decision making regarding the effects of scapular movement deviations in patients with rotator cuff pathology and scapular dyskinesia and may help inform the selection of clinical interventions.
The shoulder is the second most frequently reported site of musculoskeletal pain, with a point prevalence of 20.9%. 31 Pathology associated with the rotator cuff tendons is a common source of shoulder pain 38 and likely results from a number of different mechanisms.15,35 One theory is that the rotator cuff undergoes repetitive microtrauma due to deformation by the surrounding anatomy during shoulder motion. For example, it has long been believed that the supraspinatus insertion site (or footprint) contacts the coracoacromial arch (mechanical subacromial impingement) during shoulder motion. Although this phenomenon was originally thought to occur between 70° and 120° humerothoracic elevation, an abundance of data now suggest that the rotator cuff tendon or footprint is closest to the acromion between 30° and 70° humerothoracic elevation and begins to move away from (or clears) the acromial undersurface by 90°.1,2,7-9,16,17 Furthermore, if the arm continues to elevate, the undersurface of the rotator cuff tendon approaches, and may contact, the superior glenoid rim. This distinct mechanism, internal impingement, was identified originally in overhead athletes during combined shoulder abduction and external rotation,4,39 but it has been observed recently above 90° humeral elevation even without extreme axial rotation,18,34 suggesting it may not be exclusive to overhead athletes.
Clinicians have long theorized that scapular movement deviations may predispose a person to these mechanical impingement mechanisms by increasing the magnitude and frequency of compression. 23 For example, persons with shoulder pain have been found to exhibit decreased scapular posterior tilting,6,20,24 decreased scapular upward rotation,6,12,20 and increased scapular internal rotation. 40 However, it remains unclear the extent to which altered scapular kinematics influences rotator cuff impingement risk.
One approach to investigate this question is to systematically impose changes in scapular orientation and measure the effects on the proximity between the rotator cuff tendon insertions and the coracoacromial arch (subacromial) and glenoid (internal). This approach has been used with a small subject sample in a magnetic resonance imaging (MRI) study, 37 with human cadaveric specimens,10,28 and with 3-dimensional (3-D) computer modeling. 3 It is important to note, however, that, in all of these past studies, measurements of subacromial and glenoid proximities were made without consideration of the specific rotator cuff tendon insertions. Thus, it remains unclear the extent to which changes in scapular orientation directly affect the proximity between the rotator cuff tendon insertions and potential impinging structures.
The purpose of this study was to model the effects of scapular angular deviations on the proximity of rotator cuff tendon insertions to the coracoacromial arch and glenoid during humeral elevation in the scapular plane. It was hypothesized that the minimum distance between the supraspinatus tendon insertion and the acromion (subacromial) would decrease with scapular downward rotation, internal rotation, and anterior tilt when assessed at lower angles of humeral elevation. It was further hypothesized that the minimum distance between the supraspinatus tendon insertion, and the glenoid (internal) would decrease with scapular downward rotation when assessed at 120° of humeral elevation.
Methods
Participants
Study participants were recruited as part of a larger investigation of shoulder kinematics and measures of mechanical rotator cuff impingement. The study cohort was enrolled between 2007 and 2010 and consisted of 10 asymptomatic participants (4 women; age, 28 ± 6 years; height, 173.0 ± 8.3 cm; weight, 78.4 ± 14.1 kg) and 9 participants with signs and symptoms consistent with the broad clinical diagnosis of impingement syndrome (4 women; age, 34 ± 13 years; height, 171.6 ± 11.4 cm; weight, 79.8 ± 6.2 kg).27,30 All participants underwent motion analysis using bone-fixed electromagnetic sensors as part of the larger investigation. 22 Consequently, the nondominant side was tested in the majority (80%) of the asymptomatic cohort due to the invasive nature of the procedures. In the symptomatic cohort, however, the symptomatic (ie, tested) side corresponded with the dominant side in 88.9% of the participants. The study protocol was approved by our institutional review board, and informed consent was obtained from all participants before data collection.
Procedure
Computed tomography (CT) scans were acquired of each subject’s shoulder from which 3D subject-specific bone models were created using Mimics software (Materialise). The coracoacromial ligament is not visible on CT imaging and was therefore represented by creating a 3D plane based on anatomic descriptions (Figure 1). 5 The rotator cuff tendon footprints (ie, insertions) were identified on the humeral model such that the supraspinatus and infraspinatus tendon insertions were defined by the superior and middle facets of the greater tuberosity, respectively, and the subscapularis tendon insertion was defined by the lesser tuberosity (Figure 1). Although recent evidence suggests the individual rotator cuff tendon insertion locations are more complex, 29 we chose to use these simplified definitions as they could be implemented readily on the CT-derived bone models where the bony facets are well visualized, but tendon insertion patterns cannot be appreciated.

Modeling subacromial and internal impingement risk. (A) Superior and posterior views of the humerus positioned at 120° humerothoracic elevation (77° glenohumeral elevation) to assess internal impingement risk. (B) Superior and posterior views of rotator cuff tendon insertions (shaded) of subscapularis, supraspinatus, and infraspinatus on the humeral head when the humerus is positioned at a subject-specific lower angle to assess subacromial impingement risk. The acromion and coracoacromial ligament plane are represented semitransparent to facilitate visualization of the rotator cuff tendon insertions.
Coordinate systems were established for the humerus and scapula using published recommendations.21,41 The humeral head was centered on the glenoid and translated laterally 2 mm to account for the estimated cartilage thickness of the humeral head not visible in the CT image but known to affect glenohumeral position. MATLAB software (MathWorks) was used to position each subject’s humerus relative to the scapula based on average data in asymptomatic subjects during scapular plane abduction (Figure 1). 22 Instead of imposing subject-specific kinematic data on the bone models, kinematic data were averaged across the sample before modeling. This was done because differences between participants in glenohumeral kinematics would likely impact compression risk, thereby confounding the effect of the imposed scapular deviations, which was the primary effect of interest. Compression risk was then assessed for each subject during the simulated scapular plane abduction by calculating the minimum distances between each tendon insertion (supraspinatus, infraspinatus, and subscapularis) and potential impinging structures (glenoid, acromion, and coracoacromial ligament).
Once the baseline minimum distance measures were established, scapulothoracic angular deviations were imposed on the models by rotating the scapula ±5°, ±10°, ±20°, and ±30° about each of the 3 scapular anatomic axes. Positive angles represent deviations of upward rotation, internal rotation, and anterior tilt, while negative angles depict deviations of downward rotation, external rotation, and posterior tilt. Compression risk was then recalculated for each subject in each of the imposed scapular deviations as described previously.
The effect of the scapular deviations on compression risk (ie, minimum distance) was assessed at 2 angles of humeral elevation. The first angle (120° humerothoracic elevation) was used to investigate the proximity between the rotator cuff tendon insertion and glenoid (internal compression risk) (Figure 1A). The second angle of humeral elevation was used to investigate the proximity between the rotator cuff tendon insertion and acromion or coracoacromial ligament (subacromial compression risk) and was selected for each subject as the angle at which the distance from the supraspinatus tendon insertion to the acromion was minimized during the simulated scapular plane abduction (Figure 1B). This angle ranged from 50° to 95° humerothoracic elevation across all participants.
Statistical Analysis
Before analysis, data normality was assessed using skewness and kurtosis. Two-factor mixed-model analyses of variance (ANOVAs) were then run to compare the effect of each scapular deviation on compression risk (ie, minimum distance) with a within-subject factor of deviation magnitude (levels: 0°, ±5°, ±10°, ±20°, and ±30°) and a between-subject factor of group (levels: symptomatic, asymptomatic). Analyses were run for each tendon insertion (supraspinatus, infraspinatus, subscapularis) and impinging structure (glenoid, acromion, coracoacromial ligament). Main effects were interpreted only in the absence of a significant interaction. Pairwise follow-ups compared each scapular deviation with the baseline condition (ie, 0° deviation) and utilized Tukey-Kramer adjustments. All statistical analyses were performed using SAS 9.4 (SAS Institute) with statistical significance defined as P < .05.
Results
There were no consistent differences between symptomatic and asymptomatic subjects for any analysis (group × angle interaction: P≥ .080; group main effect: P≥ .214). However, there were significant effects of scapular deviations (ie, angle main effect) for all conditions, as described in detail below.
Proximity to Glenoid
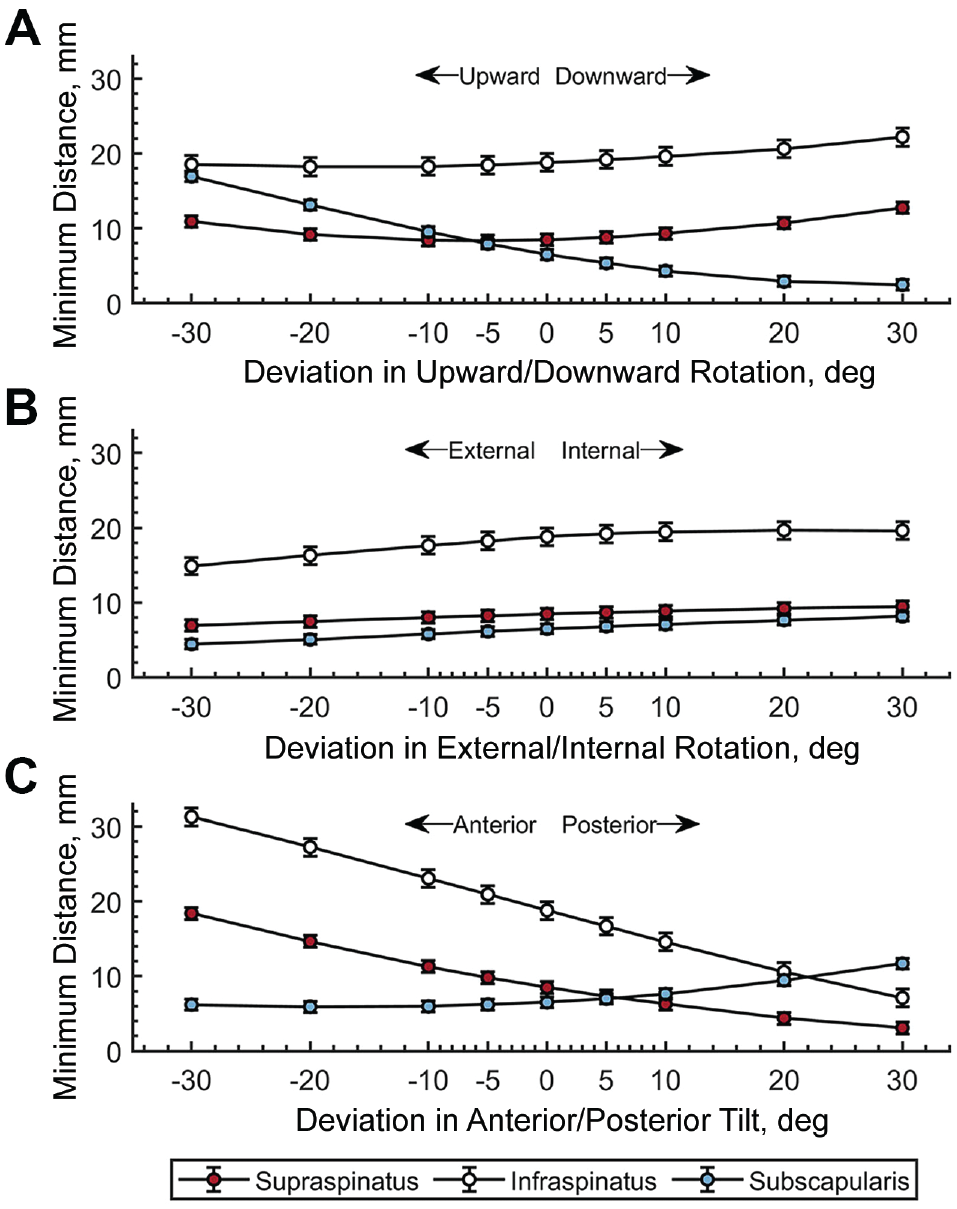
For the supraspinatus, the average (±SE) minimum distance to the glenoid at 120° humerothoracic elevation was 8.6 ± 0.6 mm before imposing any changes in scapular orientation. All scapular deviations consistently and significantly affected the minimum distance (main effect, P < .001) (Figure 2). The minimum distance significantly increased with a ≥5° change in upward rotation (1.6-9.8 mm, P < .001) or external rotation (0.9-5.0 mm, P≤ .048), or with a ≥10° change in anterior tilt (1.1-3.2 mm, P≤ .001). Furthermore, the minimum distance significantly decreased with a ≥5° change in downward rotation (1.5-6.5 mm, P≤ .001) or internal rotation (1.0-5.4 mm, P≤ .030) or with a ≥10° change in posterior tilt (1.1-2.8 mm, P < .001).

Impact of scapular deviations on the distance between the glenoid and supraspinatus, infraspinatus, and subscapularis tendon insertions. (A) Upward/downward rotation, (B) external/internal rotation, and (C) anterior/posterior tilt. Values are shown as mean, with error bars representing standard error.
For the infraspinatus, the average (±SE) minimum distance to the glenoid was 10.9 ± 0.6 mm before imposing any changes in scapular orientation. All scapular deviations affected the minimum distance consistently and significantly (main effect, P < .001) (Figure 2). The minimum distance to the glenoid significantly increased with a ≥5° change in external rotation (1.6-9.9 mm, P < .001) or with a ≥10° change in upward rotation (2.2-7.1 mm, P < .001) or anterior tilt (0.9-2.3 mm, P≤ .002). Furthermore, the minimum distance significantly decreased with a ≥5° change in internal rotation (1.6-7.6 mm, P < .001) or with a ≥10° change in downward rotation (1.9-3.9 mm, P < .001) or posterior tilt (1.1-3.3 mm, P < .001).
For the subscapularis, the average (±SE) minimum distance to the glenoid was 15.6 ± 1.0 mm before imposing any changes in scapular orientation. All scapular deviations consistently and significantly affected the minimum distance (main effect, P < .001) (Figure 2). The minimum distance to the glenoid significantly increased with a >5° change in upward rotation (2.0-11.5 mm, P < .001) or with a ≥20° change in internal rotation (2.4-3.6 mm, P < .001) or posterior tilt (1.4-2.8 mm, P < .001) or with a 30° change in anterior tilt (1.4 mm, P≤ .001). Furthermore, the minimum distance significantly decreased with a ≥5° change in downward rotation (2.0-10.9 mm, P < .001) or a ≥10° change in external rotation (1.3-4.2 mm, P≤ .041).
Proximity to the Acromion
For the supraspinatus, the average (±SE) minimum distance to the acromion was 2.1 ± 0.4 mm before imposing any changes in scapular orientation. All scapular deviations consistently and significantly affected the minimum distance (main effect, P < .001) (Figure 3). The minimum distance significantly increased with a ≥20° change in upward rotation (2.2-4.0 mm, P < .001), downward rotation (1.5-3.0 mm, P≤ .001), internal rotation (0.6-1.2 mm, P < .001), external rotation (0.4-0.9 mm, P≤ .003), or anterior tilt (1.7-3.2 mm, P≤ .001) or with a 30° change in posterior tilt (1.2 mm, P < .001).

Impact of scapular deviations on the distance between the acromion and supraspinatus, infraspinatus, and subscapularis tendon insertions. (A) Upward/downward rotation, (B) external/internal rotation, and (C) anterior/posterior tilt. Values are shown as mean, with error bars representing standard error.
For the infraspinatus, the average (±SE) minimum distance to the acromion was 3.5 ± 0.5 mm before imposing any changes in scapular orientation. All scapular deviations affected the minimum distance consistently and significantly (main effect, P < .001) (Figure 3). The minimum distance significantly increased with a ≥10° change in anterior tilt (1.3-6.3 mm, P≤ .012); with a ≥20° change in upward rotation (1.6-3.1 mm, P < .001), downward rotation (1.1-2.2 mm, P≤ .001), or internal rotation (0.9-1.8 mm, P < .001) or with a 30° change in external rotation (0.8 mm, P < .001).
For the subscapularis, the average (±SE) minimum distance to the acromion was 10.9 ± 1.0 mm before imposing any changes in scapular orientation. All scapular deviations consistently and significantly affected the minimum distance (main effect, P < .001) (Figure 3). The minimum distance to the acromion significantly increased with a ≥10° change in upward rotation (2.1-8.3 mm, P < .001), internal rotation (1.0-3.0 mm, P≤ .003), or posterior tilt (3.2-10.6 mm, P < .001). Furthermore, the minimum distance significantly decreased with a ≥10° change in internal rotation (1.0-2.9 mm, P≤ .003) or anterior tilt (2.5-5.3 mm, P < .001) or with a 20° change in downward rotation (1.5 mm, P = .016).
Proximity to the Coracoacromial Ligament
For the supraspinatus, the average (±SE) minimum distance to the coracoacromial ligament was 8.4 ± 0.8 mm before imposing any changes in scapular orientation. All scapular deviations affected the minimum distance consistently and significantly (main effect, P < .001) (Figure 4). The minimum distance increased significantly with a ≥5° change in anterior tilt (1.3-9.9 mm, P < .001), with a ≥20° change in downward rotation (2.2-4.3 mm, P < .001) or internal rotation (0.7-1.0 mm, P≤ .007), or with a 30° change in upward rotation (2.4 mm, P < .001). Furthermore, the minimum distance decreased significantly with a ≥10° change in posterior tilt (2.2-5.4 mm, P < .001) or with a ≥20° change in external rotation (1.0-1.5 mm, P < .001).
Impact of scapular deviations on the distance between the coracoacromial ligament and supraspinatus, infraspinatus, and subscapularis tendon insertions. (A) Upward/downward rotation, (B) external/internal rotation, and (C) anterior/posterior tilt. Values are shown as mean, with error bars representing standard error.
For the infraspinatus, the average (±SE) minimum distance to the coracoacromial ligament was 18.8 ± 1.2 mm before imposing any changes in scapular orientation. All scapular deviations affected the minimum distance consistently and significantly (main effect, P < .001) (Figure 4). The minimum distance significantly increased with a ≥5° change in anterior tilt (2.1-12.5 mm, P < .001) or with a ≥20° change in downward rotation (1.8-3.4 mm, P < .001). Furthermore, the minimum distance significantly decreased with a ≥5° change in posterior tilt (2.1-11.7 mm, P < .001) or with a ≥10° change in external rotation (1.2-3.9 mm, P≤ .008).
For the subscapularis, the average (±SE) minimum distance to the coracoacromial ligament was 6.5 ± 0.6 mm before imposing any changes in scapular orientation. All scapular deviations consistently and significantly affected the minimum distance (main effect, P < .001) (Figure 4). The minimum distance to the coracoacromial ligament significantly increased with a ≥5° change in upward rotation (1.4-10.5 mm, P≤ .044), or with a >20° change in internal rotation (1.2-1.7 mm, P < .001) or posterior tilt (2.9-5.2 mm, P < .001). Furthermore, the minimum distance significantly decreased with a ≥10° change in downward rotation (2.2-4.0 mm, P < .001) or external rotation (0.7-2.1 mm, P ≤ .020). However, the minimum distance did not fall below the 5 mm threshold for impingement risk in any condition except the ≥10° change in downward rotation.
Discussion
The primary results of this study suggest that scapular angular deviations can substantially change the minimum distance between the rotator cuff tendon insertion and potential impinging structures (ie, glenoid, acromion, coracoacromial ligament). Specifically, at 120° humerothoracic elevation, minimum distances from the supraspinatus and infraspinatus insertions to the glenoid increased with ≥5° changes in upward rotation (1.6-9.8 mm, P < .001) or external rotation (0.9-5.0 mm, P≤ .048), or with ≥10° changes in anterior tilt (1.1-3.2 mm, P < .001). At lower angles, ≥20° changes in most scapular orientations significantly increased the distance between the supraspinatus and infraspinatus insertions and the acromion or coracoacromial ligament.
Although clinical theory often states that scapular upward rotation, external rotation, and posterior tilt help protect rotator cuff insertions,14,19,23,26,35 the results of this study suggest that this theory is an oversimplification. The patterns of effect demonstrated were deviation-, magnitude-, tendon-, and mechanism- (ie, subacromial, internal) specific. Ultimately, understanding the effects of scapular motion deviations on the rotator cuff mechanical impingement risk allows clinicians to identify positions of potential injury and interpret scapular movement impairments observed during a clinical examination.
From the perspective of internal impingement, the effect of scapular movement deviations on the minimum distance is generally linear, meaning that increasing the deviation in one direction (eg, upward rotation) increases the minimum distance while increasing the deviation in the opposite direction (eg, downward rotation) decreases the minimum distance. In this way, upward rotation, external rotation, and anterior tilt increase the minimum distance between the glenoid and supraspinatus and infraspinatus insertions, while downward rotation, internal rotation, and posterior tilt decrease the minimum distance (Figure 2). For the supraspinatus, upward rotation is the primary scapular deviation that increases the minimum distance with a change as small as 5° increases the minimum distance by an average of 1.6 mm. For the infraspinatus, however, scapular external rotation is the primary scapular deviation that increases the minimum distance with a change as small as 5° increases the minimum distance by a similar amount. These findings make sense mechanically given the location of the tendon insertions and the movement of the glenoid as a result of the scapular deviation. For example, with the humerus rotated to 120° humerothoracic elevation (Figure 1A), the supraspinatus insertion, located on the anterosuperior aspect of the greater tuberosity, lies in the plane of scapular motion for upward/downward rotation, whereas the infraspinatus, located on the posterosuperior aspect of the greater tuberosity, lies in the plane of scapular motion for internal/external rotation. Thus, upward rotation and external rotation logically move the tendon insertions further away from the glenoid, while downward rotation and internal rotation do the opposite.
Despite vastly different methodologies, these results are generally in line with previous work by Mihata et al, 28 who investigated internal impingement in human cadavers during the late cocking phase of throwing at 90° humeral elevation. To do this, the researchers altered the scapula’s orientation by 10° about each axis while assessing internal impingement by projecting points along the rotator cuff insertion onto the glenoid and calculating an area of overlap. The authors reported that increasing either scapular upward rotation or external rotation significantly decreased the area of overlap. Taken together, the results of both studies suggest that impairments in scapular upward rotation or external rotation (ie, decreased internal rotation) may be an important kinematic consideration when internal impingement is suspected as the source of a patient’s symptoms. This may be especially pertinent as contact between the glenoid and rotator cuff insertions has been reported to occur in most subjects even during functional reaching or scapular plane abduction.18,34 Therefore, internal impingement may be an overlooked mechanism of shoulder pain and rotator cuff pathology outside of overhead athletes.
To investigate subacromial impingement risk, we investigated the proximity of rotator cuff tendon insertions to the acromion and coracoacromial ligament at lower angles of humerothoracic elevation given the findings of previous studies that reported the rotator cuff insertions generally clear the coracoacromial arch by 90° humerothoracic elevation.8,13,16,17 Further, we chose to investigate proximities at a humeral elevation angle that is individualized for each subject based on when the supraspinatus tendon was closest to the acromion instead of a standardized angle as was done for assessing internal impingement risk (ie, 120°). This decision had distinct consequences that need to be considered when interpreting the results of the study. Specifically, because the minimum distance was already minimized by design, the minimum distance between the acromion and supraspinatus and infraspinatus insertions typically increased following any deviation in scapular orientation (Figure 3). This phenomenon impedes the ability to interpret directly the impact of scapular motion deviations on compression risk against the acromion as any change in scapular orientation is perceived to have a positive impact on impingement risk. Therefore, results regarding tendon compression risk against the acromion should be interpreted with caution.
Although the results regarding tendon compression risk against the coracoacromial ligament with changes in scapular/upward downward rotation follow a similar pattern to that of the acromion (ie, increasing minimum distance regardless of change), a directionality appears to emerge for internal/external rotation and anterior/posterior tilt. Specifically, scapular anterior/posterior tilt appears to have the largest effect on the minimum distance as a change as little as 5° in either direction significantly impacts the minimum distance to the supraspinatus and infraspinatus insertions (Figure 4). Interestingly, however, anterior tilt appears to increase the distance between the coracoacromial ligament and tendon insertions, which is antithetical to previous research and commonly held clinical theory.19,23,24,26,37 Only the subscapularis tendon followed a pattern where increased anterior tilt reduced the minimum distance. The extent to which changes in scapular impairments impact shoulder symptoms and rotator cuff pathology remains unclear given the lack of longitudinal studies. Even so, the results of the current study suggest that scapular movement may be important as it alters the distance between the rotator cuff tendon insertions and potential impinging structures.
The question of whether scapular movement impairments (eg, dyskinesia) is potentially pathological is a question of much debate in research and clinical practice,11,25,32 and deserves consideration in the context of the current study. We posit that this debate persists, in part, because the consequences of the movement impairments are not well understood. For example, if it is known that the movement impairments do not significantly alter mechanisms of tendon injury (eg, subacromial, internal impingement), instability (eg, joint congruency), and muscle function (eg, lines of action, moment arms), the conclusion that dyskinesia may represent normal between-person variability of movement may be supported. However, this conclusion cannot be made based on the current state of the literature, and the current study aims to provide important context relative to mechanisms of tendon injury. More research is needed to investigate the consequences of these scapular movement alterations on important factors such as tissue stress and symptom provocation to establish the clinical implications of our findings. Although preliminary, the results of the current study may be useful to clinicians as they perform and interpret the results of scapular modification testing,33,36 if they suspect subacromial or internal impingement may be a factor in their patient’s shoulder condition.
Limitations
There are limitations to consider when interpreting the results of this study. In particular, we used previously acquired average motion data using bone-fixed sensors to initially position the scapula and humerus. Although the previous data were collected in vivo and are not subject to skin motion artifact, 22 the modeling in this study did not allow for the natural motion of each individual subject to be investigated. This was intentional, as differences between participants would likely impact compression risk, thereby confounding the effect of the imposed scapular deviations, which was the primary effect of interest. Future work will build upon the result of the current study by combining subject-specific anatomic models and kinematics to investigate the effect of scapular motion deviations on tendon compression risk in vivo.
In addition, the use of CT-derived 3D bone models does not allow for consideration of soft tissue data. Instead, the tendon insertion sites were identified based on the bony insertion, and subject-specific variation in tendon thickness and soft tissue insertion areas could not be accounted for. Similarly, the coracoacromial ligament was modeled based on accepted anatomic information rather than reconstructed from imaging. 5 Another limitation of this study is the manner in which the scapular deviations were imposed. Although scapular deviations can be observed simultaneously about multiple axes (eg, downward rotation and anterior tilt), deviations were imposed about each scapular anatomic axis individually to first understand the “simple” effects before proceeding to more complex multiaxial deviations in future work. Finally, this study measured only the minimum distance between surfaces and could not account for the location of the minimum distance of specific soft tissue deformations that may contribute to pathology. Despite these limitations, this investigation provides unique data that allow improved interpretation of the potential effects of scapular dyskinesia on risk of injury to the rotator cuff tendon insertions.
Conclusion
Scapulothoracic deviations affect mechanical impingement risk, especially for the supraspinatus and infraspinatus. Scapular downward rotation decreases the distance between the rotator cuff tendon insertions and the glenoid at higher angles of elevation. For lower angles, interpretation was complicated because the humeral elevation angle was defined by the minimum distance. These results may assist clinical decision making regarding the effects of scapular movement deviations in patients with rotator cuff pathology and scapular dyskinesis and may help inform the selection of clinical interventions.
Footnotes
Acknowledgements
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the US National Institutes of Health.
Final revision submitted May 20, 2023; accepted July 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: research support was received from the Foundation for Physical Therapy, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (award Nos. K01-HD042491 and R03-HD053399), and the National Institute of Arthritis and Musculoskeletal and Skin Diseases (award No. T32AR050938). J.P.B. has received education payments from Gemini Medical and consulting fees from Zimmer Biomet Holdings. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Minnesota (reference no. 991M24181).