
Abstract
Background:
The arthroscopic Broström technique with or without Gould modification has been used to treat patients with anterior talofibular ligament injury who failed nonoperative management and progressed to chronic lateral ankle instability. However, some patients develop limited range of motion over the ankle joint postoperatively.
Purpose/Hypothesis:
To compare the clinical outcomes and midterm functional performance of knot-tying techniques between using a knot pusher and a semiconstrained freehand tie during arthroscopic Broström-Gould procedure with inferior extensor retinaculum (IER) augmentation. It was hypothesized that the semiconstrained freehand tie would provide better plantarflexion of the ankle joint compared with the knot pusher.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 135 consecutive patients with mild-to-moderate lateral ankle instability (mean age, 42.7 years; range, 16-78 years) who underwent an arthroscopic Broström-Gould procedure from March 1, 2016, to April 30, 2022. The patients were divided into 2 groups according to the tying technique used in the Gould modification: surgical tie using a knot pusher (KP group; n = 30) or a semiconstrained freehand tie (FT group; n = 105). Radiographic parameters and ultrasound dynamic testing were examined during the preoperative assessment. Preoperative and 2-year postoperative assessments comprised American Orthopaedic Foot and Ankle Society Ankle-Hindfoot Scale, visual analog scale for pain, and 12-Item Short Form Survey (SF-12) scores.
Results:
The 2 groups had no differences in age, sex, or severity distribution in the preoperative assessment. American Orthopaedic Foot and Ankle Society Ankle-Hindfoot Scale, visual analog scale pain, and SF-12 scores were significantly better at the postoperative evaluation (all P < .05) in both groups. No significant difference was noted between groups in outcome scores. In the KP group, however, 7 out of 30 patients (23.3%) developed ankle stiffness with tightness when performing plantarflexion movement. No patients in the FT group reported similar symptoms.
Conclusion:
For mild-to-moderate chronic lateral ankle instability, we propose an arthroscopic Broström procedure with the addition of IER augmentation using a semiconstrained freehand tie to avoid overtightening the IER. This ensures favorable patient satisfaction and clinical outcomes without limitation of plantarflexion of the ankle joint and avoids the possible complication of stiffness with plantarflexion.
Keywords
Ankle sprains are a common injury, and 85% of ankle sprains are lateral ankle ligament injuries. Most patients with mild-to-moderate injury can recover adequately through conservative treatment. 24 However, 30% of patients who have not recovered after treatment may receive a diagnosis of chronic lateral ankle instability (CLAI). Surgical intervention is considered if conservative treatment is ineffective, and various procedures for addressing CLAI have been proposed.6,28
In the 1960s, Broström et al 4 proposed direct repair of the anterior talofibular ligament (ATFL) by conducting open surgery over the lateral ankle. This procedure was then modified by Gould et al,8,9 who performed inferior extensor retinaculum (IER) augmentation and used an open technique; this was termed the Broström-Gould procedure.8,9 The arthroscopically assisted technique was introduced to promote faster recovery, minimize surgical trauma, and decrease perioperative and postoperative complications.11,20 Arthroscopy is a feasible technique for visualizing and assessing the severity of a ligamentous injury and aids in the selection of a suitable surgical technique. In addition, concomitant intra-articular lesions can be examined and treated using arthroscopy. Chondral injuries of the talocrural joint have been observed in 77% of patients with CLAI. 15 Therefore, the arthroscopic Broström technique with or without the Gould modification has become the preferred treatment for lateral ankle ligament repair.
Studies have reported comparable radiographic parameter measurements and ankle stability when comparing open surgery with the arthroscopic Broström-Gould procedure. Therefore, arthroscopic techniques for lateral ankle ligament repair have become more popular due to the advantages of minimally invasive surgery. Nevertheless, some complications, such as the possibility of sural nerve injury and limited plantarflexion of the ankle joint, can occur in patients postoperatively. Stiffness in plantarflexion is particularly seen in patients who previously received IER augmentation for mechanical strength reinforcement. 10
Limitation of plantarflexion in the ankle can be attributed to overtightening the IER during knot tying. In the present study, we analyzed whether knot tying by using a knot pusher or a semiconstrained freehand tie during IER augmentation affects the clinical outcomes and midterm functional performance of patients after the arthroscopic Broström-Gould procedure. We hypothesized that IER augmentation using semiconstrained freehand tie provides better plantarflexion of the ankle joint and patient satisfaction than that achieved by using a knot pusher.
Methods
Patient Profiles
All experiments and surgical procedures were approved by the institutional review board of our hospital, and informed consent was obtained from all enrolled patients. In this retrospective study, we enrolled 135 consecutive patients with ATFL and/or calcaneofibular ligament (CFL) injury who underwent the arthroscopic Broström procedure with Gould modification between March 1, 2016, and April 30, 2022, and had follow-up data for at least 24 months. All patients were initially treated nonoperatively and given pain medication, an ankle brace, and subsequent physical therapy. Surgical intervention was suggested if symptoms remained for >6 months without improvement. The degree of severity of ligamentous injury was classified using the Ankle Sprain Grading Scale, 13 in which grade 1 injury indicates stretched ATFL and CFL with mild ankle swelling but stable ankle joint, and grade 2 injury may present marked ankle pain and bruise due to partial tear of the ATFL. Patients with grade 1 or 2 injury may be treated conservatively. However, surgical intervention is usually needed in patients with grade 3 injury due to marked ankle instability caused by both complete ATFL and CFL tear. The exclusion criteria for this study were poor skin condition, cellulitis, tarsal coalition, hindfoot varus deformity, and impeded lower-limb circulation.
Radiographic parameters, including talar tilting and anterior translation of the tibiotalar joint, were measured while the ankle was under stress. Dynamic ultrasound was performed to assess the injured ATFL and CFL (Figure 1). During the ultrasound, we carefully measured the gap between the ruptured end of the ATFL or CFL and the origin site on the fibular tip in neutral and plantar-inversion positions of the ankle joint, respectively, and, based on this gap, classified the ATFL injury into 1 of 3 grades (Table 1 and Figure 2). According to our ultrasound-based classification, for patients with grade 2 injury (ie, a gap of 5-15 mm), surgical intervention was performed on the basis of the tension and texture of the residual stump. 27 Magnetic resonance imaging (MRI) was used to assess the degree of ATFL and CFL tear and the quality of the remaining ligament (Figure 3).
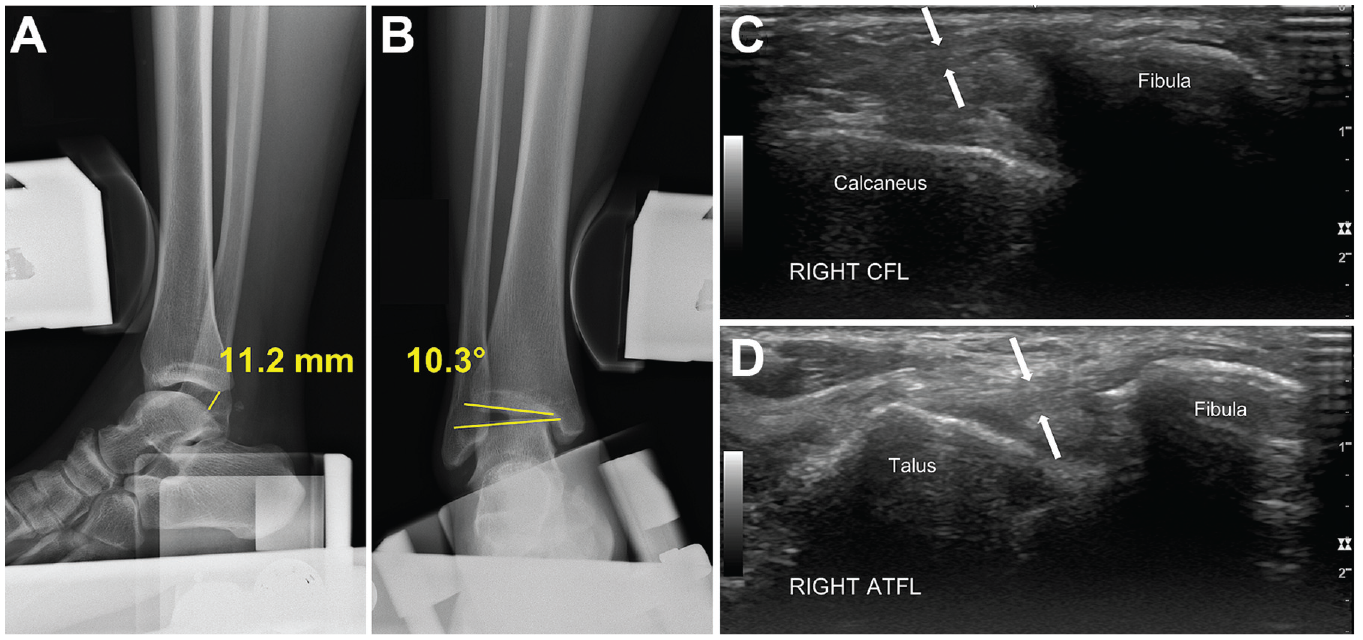
Preoperative radiographs and ultrasound images. (A, B) Significant anterior translation and talar tilting over tibiotalar joint under ankle stress views. (C, D) Ultrasound scans demonstrating the grading of injured CFL and ATFL under dynamic testing. ATFL, anterior talo-fibular ligament; CFL, calcaneofibular ligament.
Dynamic Ultrasonography Classification of Chronic Lateral Ankle Ligament Injury

Distance between the ruptured ATFL and the fibular origin site, observed through dynamic ultrasound examination. The gap was measured at the maximal plantarflexion-inversion positions of the ankle joint. ATFL, anterior talo-fibular ligament.
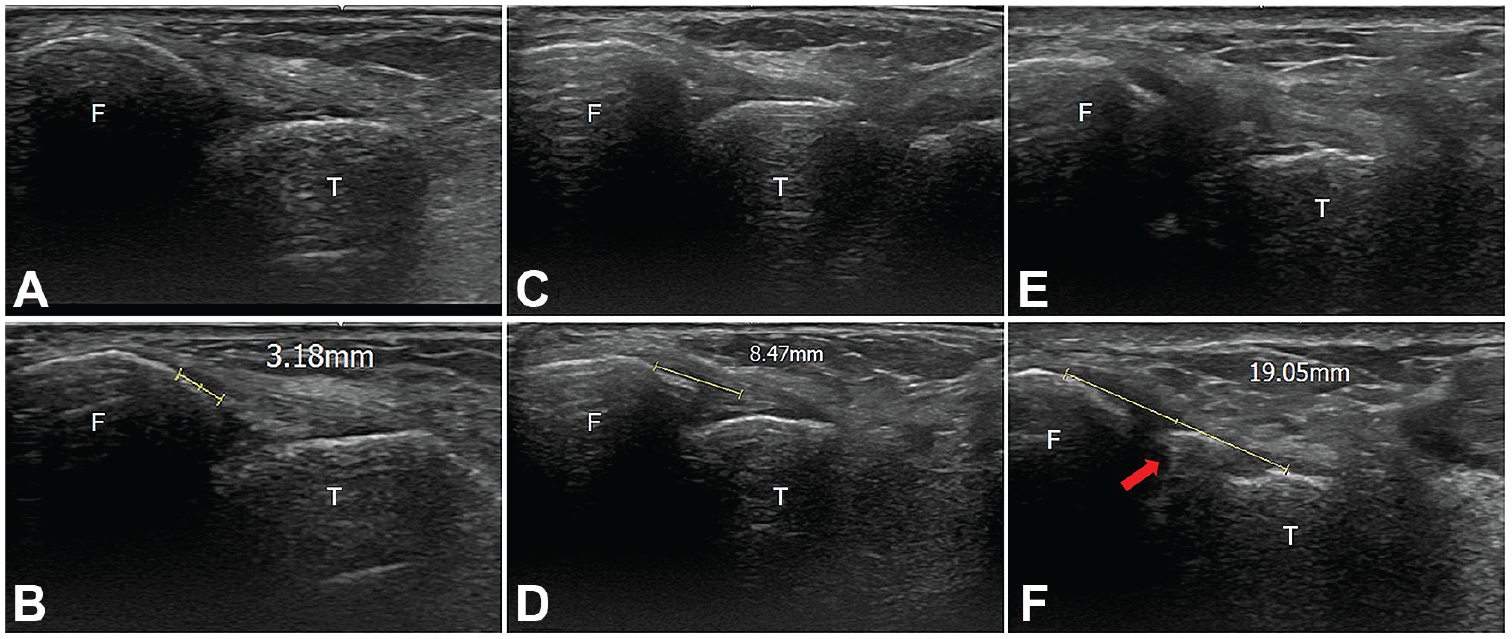
Grading of ATFL injury with ultrasound under dynamic examination with ankle in plantarflexion-inversion position. (A, B) A gap of <0.5 cm was considered to be easily reparable with arthroscopic repair (grade 1). (C, D) A gap of between 0.5 and 1.5 cm was regarded as reparable but ligament reconstruction should be seriously considered (grade 2). (E, F) A gap of >1.5 cm was considered irreparable, therefore requiring ligament reconstruction (grade 3). The red arrow indicates the avulsion of bony fragment from the fibular tip. ATFL, anterior talo-fibular ligament; F, fibula; T, talus.

Preoperative MRI images. (A) Axial view showing ATFL tear (arrowhead) near the insertion site of the fibula tip. (B) Coronal view showing hyperintensity near CFL with marked effusion (white arrow), indicating potential injury of the CFL (red arrow). ATFL, anterior talo-fibular ligament; CFL, calcaneofibular ligament; MRI, magnetic resonance imaging.
Study Groups
The patients enrolled in our study were divided into 2 groups. Initially, patients received IER augmentation with a surgical tie through a knot pusher (KP group; n = 30); however, after some patients developed ankle stiffness, we modified the tying technique to a semiconstrained freehand tie (FT group; n = 105). The degree of severity of ligamentous injury was classified using the Ankle Sprain Grading Scale, 13 and the arthroscopic classification was that used by Thès et al. 23
Surgical Technique and Postoperative Care Protocols
All surgical procedures were performed by a senior orthopaedic surgeon (C.-C.W.). Under spinal anesthesia or laryngeal mask anesthesia, the patient was placed on the operating table in the supine position. A pneumatic tourniquet was used for all patients. The surgical site was disinfected and draped in accordance with the standard protocol. After exsanguination, a percutaneous incision was made to create an anteromedial portal to facilitate the recording of the pathology (Figure 4A,B). A 21-gauge syringe needle was inserted from the anterolateral side of the ankle to the position of the accessory anterolateral portal, which was a working portal used to perform arthroscopic debridement on the inflamed tissue and the injured ligament by shaving (Stryker). A probe was inserted to test the integrity and tension of the remaining well-debrided ATFL or CFL. After the bone platform of the fibular tip had been prepared, two 3-mm biosuture anchors (Gryphon, Mitek, Depuy Synthes) were inserted into the fibula tip: one was inserted at the ATFL insertional site and the other 1 cm superiorly from the first suture anchor. The torn ATFL was captured with 1 limb of the suture anchor and pulled onto the original insertion site to achieve anatomic repair through the self-cinching surgical tie technique. 22

Arthroscopic repair of the AFTL. (A) The torn ATFL was partially detached from the fibular tip (arrowhead). (B) The torn ATFL was well prepared and reattached onto the fibular tip with biosuture anchors using the self-cinching tying technique. (C) IER augmentation completed using the semiconstrained freehand tie technique provides adequate tension and stability to protect the repaired ligament. The gap between the fibular tip and augmented IER was 5 mm. ATFL, anterior talo-fibular ligament; IER, inferior extensor retinaculum.
The Gould modification was performed percutaneously by introducing a Micro SutureLasso (Arthrex) to capture the IER with 3 limbs of No. 2-0 threads from the two 3-mm suture anchors using surgical knots. 1 In the KP group, all 3 limbs secured on the IER were tightened with a knot pusher until the IER was in contact with the fibular bone tip for the ankle in a neutral position. In the FT group, the tension of the IER was adjusted carefully under arthroscopic inspection with semiconstrained freehand tie. The distance between the fibular tip and IER was approximately 4 to 5 mm for the ankle in a neutral position (Figures 4C and 5). Finally, the global alignment was inspected arthroscopically, and 1 Mini-Hemovac (PAHSCO) was placed. The wound was closed in layers, and 1 short leg splint was applied to complete the procedure.
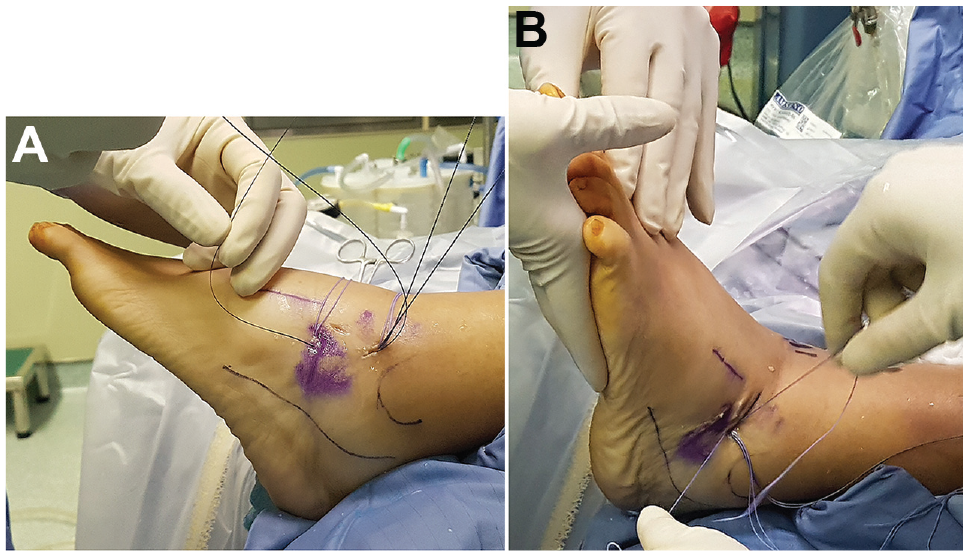
To reach adequate tension, the ankle joint was kept in 90° position when performing the Gould modification with the semiconstrained freehand tying technique. (A) The IER was captured with the remaining threads from 2 suture anchors percutaneously. (B) The ankle joint was kept in neutral position, and the tension of knot was adjusted by semiconstrained freehand tie.
Postoperatively, walking boots with partial weightbearing were worn by the patients for 6 weeks, and individualized rehabilitation was provided. Patients were encouraged to walk freely and perform plantarflexion and dorsiflexion motion. Ankle inversion was strictly prohibited for 3 weeks.
Surgical Outcomes and Radiographic Evaluations
Radiographic parameters for lateral ankle stability (talar tilting and anterior translation) were recorded preoperatively. Clinical outcomes, which were assessed using the visual analog scale (VAS) for pain, the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score, and the 12-Item Short Form Survey (SF-12), were evaluated preoperatively, postoperatively, and at final follow-up. Complications and limitation of ankle range of motion (ROM) were recorded using a goniometer in a standard fashion for all patients by 2 independent blinded examiners. The ankle sprain grade, arthroscopic grade, and radiographic parameters of the patients were recorded and measured by a single experienced orthopaedic surgeon (C.-C.W.) and a senior orthopaedic resident (T.-Y.L.).
Statistical Analysis
A paired t test was performed to evaluate preoperative radiographic parameters (eg, talar tilting and anterior translation) and clinical functional outcomes (VAS pain, AOFAS, and SF-12 scores) preoperatively, postoperatively, and at the final follow-up. Analyses between groups were conducted using Student t tests and chi-square tests. Statistical differences were defined by P < .05. All data were analyzed using SPSS Version 25 (IBM-SPSS).
Results
Patient Demographics
A total of 135 patients (42 men and 93 women) with a mean age of 42.7 years (range, 16-78 years) were enrolled in this study (Table 2). The KP group consisted of 30 patients (12 men and 18 women), whereas the FT group consisted of 105 patients (30 men and 75 women). No significant intergroup differences were observed between the groups regarding ankle instability in terms of ankle sprain grade (P = .549) or arthroscopic grade (P = .399). The mean follow-up duration was 31.6 ± 2.3 and 29.1 ± 2.8 months for the KP and FT groups, respectively (P = .152).
Patient Demographic and Perioperative Variables a

Data are reported as mean ± SD or n. BMI, body mass index.
Clinical Outcomes Assessment
The preoperative and postoperative ankle joint ROM values and outcome scores for the study groups are given in Table 3. In the preoperative assessment, both groups presented comparable ROM for plantarflexion and inversion of the ankle joint. Postoperatively, the freehand tie group had significantly greater plantarflexion ROM compared with the KP group (44.3°± 3.9° vs 40.5°± 2.8°, respectively; P = .042). There were no significant differences in preoperative outcome scores between the groups, indicating that the distribution of severity in both groups was similar. Postoperatively, the KP group had significant improvement in ankle joint plantarflexion compared with preoperatively (P = .042), and both groups saw significant improvements in VAS pain, AOFAS, and SF-12 scores (P = .019 to .049), with no significant between-group differences.
Comparison of Between-Group and Within-Group Differences in Preoperative and Postoperative Clinical Outcomes a
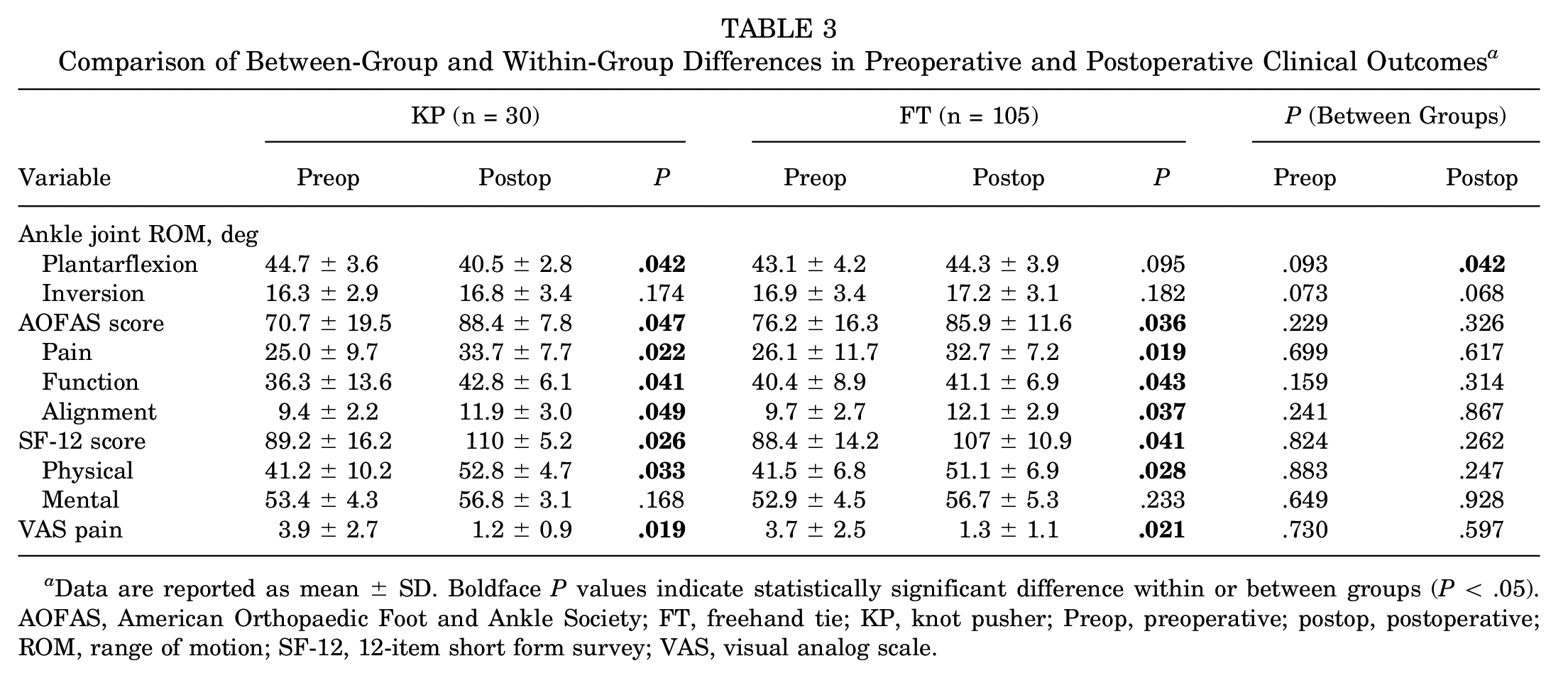
Data are reported as mean ± SD. Boldface P values indicate statistically significant difference within or between groups (P < .05). AOFAS, American Orthopaedic Foot and Ankle Society; FT, freehand tie; KP, knot pusher; Preop, preoperative; postop, postoperative; ROM, range of motion; SF-12, 12-item short form survey; VAS, visual analog scale.
Complications
The postoperative complications for both groups are listed in Table 4. Limited ROM of the ankle joint was observed during the follow-up in the KP group; 7 patients (23.3%) experienced mild stiffness when performing plantarflexion movements. However, no patients in the FT group had similar issues.
Postoperative Complications a

Data are reported as n (%). FT, freehand tie; KP, knot pusher.
Discussion
In the current study, we used ultrasound dynamic testing to determine surgical planning. The most important finding was that the 2-year-postoperative follow-up revealed comparable pain relief, clinical outcomes, and function performances in both groups. In addition, none of the patients who underwent IER augmentation using a semiconstrained freehand tie complained about ankle stiffness with tightness or limited ROM over the ankle joint. Thus, our study resulted in significant pain relief with improved patient satisfaction, and we made every effort to reach favorable clinical outcomes on the basis of well-developed surgical techniques. To the best of our knowledge, this study is the first case series to propose the concept of using a semiconstrained freehand tie to perform IER augmentation as a temporary biodegradable internal brace.
Several studies have demonstrated good clinical outcomes of arthroscopic-assisted ATFL repair. A prospective study conducted by Lopes et al 17 of 286 patients reported that arthroscopic treatment was a promising and reliable technique for lateral ankle ligament injury. Feng et al 5 reported favorable clinical outcomes after following up on 37 patients at 6, 12, 24, 36, and 48 months postoperatively. The author suggested that arthroscopic-assisted techniques enable more precise anatomic repair of the ATFL and are as effective as conventional surgical treatment in medium- and long-term follow-ups. Hagio et al 12 also reported positive functional outcomes, high patient satisfaction, and restored morphology of the ATFL after arthroscopic-assisted repair.
Further studies have compared the clinical outcomes between arthroscopic-assisted AFTL repair and an open technique. Matsui et al 19 retrospectively reviewed 37 patients, and the reported outcomes revealed equivalent clinical results at the 1-year follow-up in the 2 groups, but the arthroscopic group recovered from surgery more quickly. A systemic review conducted by Guelfi et al 10 of 721 patients from 19 studies (13 open and 6 arthroscopic) reported higher complication rates in the arthroscopic group, including superficial wound infection, delayed wound healing, and sensory disturbance over the lateral side of the ankle; however, these results did not affect the satisfaction rate (open, 91.7%; arthroscopic, 96.4%). Woo et al 25 reported better clinical outcomes in an arthroscopic group when performing a short-term follow-up and evaluating AOFAS, SF-36, and VAS pain scores. Moreover, less pain was reported during the perioperative period. A systemic review and meta-analysis performed by Zhi et al 30 divided 473 patients into open and arthroscopic groups. Comparable clinical outcomes were reported in the 2 groups, and arthroscopic techniques may alleviate more pain because the surgery was minimally invasive. Moreover, arthroscopic techniques did not result in higher rates of nerve injury or total complications. 30 Other studies have similarly concluded that arthroscopic-assisted surgery by performing the Broström technique not only yields higher patient satisfaction but also a lower complication rate.21,31
Although the arthroscopic Broström procedure is becoming a promising treatment for CLAI, the Gould modification has received criticism, and its use has depended on surgeon preference. Some other studies have compared the Broström technique with and without the Gould modification. In 2006, Aydogan et al 2 performed a cadaveric study with 10 specimens in each group to evaluate the biomechanical stability of Broström repair compared with the Broström-Gould modification. The results revealed that IER augmentation provided sufficient protection for primary ATFL repair. However, Behrens et al 3 reported no significant differences in the biomechanical stability of ankles regardless of whether the Gould modification was used. Similar results were obtained by Giza et al 7 by using 20 cadaveric feet to test the strength of a repair; the repair strength obtained through IER augmentation was not significantly higher. The results of these studies should be read with caution; no tissue-healing processes were implemented in the biomechanical studies involving cadaveric specimens. Moreover, the increase in inversion resistance did not fully indicate clinical benefit.
Some researchers have compared the Broström procedure with versus without IER augmentation in clinical application. Kocher et al 14 reported favorable clinical outcome scores and ankle stability with use of a modified Broström technique with IER augmentation for treating pediatric and adolescent patients with CLAI. Yoo et al 29 discovered that patients with internal bracing from IER augmentation could perform physical activity earlier. Similar conclusions were drawn by Martin et al, 18 who found that IER augmentation enabled patients to begin functional rehabilitation sooner after surgery. By contrast, Lee et al 16 conducted a retrospective review of 82 consecutive patients and compared additional IER augmentations. They suggested that additional IER augmentations did not guarantee better outcomes and that suture knots could result in pain, discomfort, and the sensation of a foreign body.
Of those patients treated with Gould procedure using a knot pusher, some experienced ankle stiffness when performing plantarflexion. This affects not only functional performance and gait pattern but also activity and quality of daily life. Although there is only 4° difference in plantarflexion with statistical significance, it remains clinically important in improving patient satisfaction. From a clinical point of view, this is very much in line with the purpose of the questionnaire design, and the same results are indeed observed in our study.
In this study, we introduced the concept of using a biodegradable internal brace with semiconstrained tension to provide additional support for repaired ligaments. This type of IER augmentation with freehand tying can provide temporary stability and protection for ATFL repair until the ligament tissue heals. All suture anchors and suture threads used were made from absorbable materials. Suture knots are partially absorbed within approximately 1 year, and anchors are absorbed within approximately 2 years. 26 Patients in neither group had a palpable suture knot after suture materials had degraded and did not report painful sensations or irritation related to a suture knot at the postoperative 1-year follow-up. However, ankle plantarflexion was significantly limited in patients who received IER augmentation with a knot pusher, which led to unsatisfactory results. Freehand tying prevented limitation of plantarflexion because the IER was not in contact with the fibular bone surface; a 4 to 5 mm gap existed between the IER and fibular bone. Therefore, the ankle had a dynamic space allowing motion during dorsiflexion and plantarflexion through a semiconstrained configuration. Moreover, after tissue healing, because the IER was not in contact with the fibular bone surface, the IER was not tethered by the periosteum. Consequently, IER movement was independent, which decreased the possibility of ankle plantarflexion limitation. Therefore, we suggest performing IER augmentation by using a freehand tying technique, which provides additional strength to support the repaired lateral ligament and prevents limitation of ankle plantarflexion and the long-term discomfort caused by suture knot irritation.
Limitations
This study has some limitations. First, this is a nonrandomized, retrospective, and single-center analysis. Second, the number of patients included in this study is limited; group 1 has only 30 patients. Third, all assessment scoring systems and radiographic parameters were assessed by a single orthopaedic physician. Fourth, the postoperative rehabilitation program arranged for patients depended on the patients’ functional demands, such as those of elite athletes. However, early rehabilitation for athletes was performed to prevent loss of muscle power, and the inversion position was strictly prohibited, which is the same procedure conducted during rehabilitation programs for patients with lesser demands. A prospective cohort study or randomized controlled trial should be performed as an evidence-based clinical evaluation with a long-term follow-up.
Conclusion
For mild-to-moderate CLAI, we propose an arthroscopic Broström procedure with the addition of IER augmentation using a semiconstrained freehand tie to avoid overtightening the IER. This ensures favorable patient satisfaction and clinical outcomes without limitation of plantarflexion of the ankle joint and avoids the possible complication of stiffness with plantarflexion.
Footnotes
Final revision submitted June 20, 2023; accepted June 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Buddhist Tzu Chi Medical Foundation (TCMF CP I10-01). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (ref No. 11-X-170).