
Abstract
Background:
It is unknown whether the outcomes achieved in the early period after revision lateral meniscal allograft transplantation (RLMAT) are maintained through the midterm period.
Purpose:
To evaluate the midterm clinical and radiological results of patients who underwent RLMAT.
Study Design:
Case series; Level of evidence, 4.
Methods:
We reviewed the outcomes of 19 RLMATs in 18 patients with at least 5 years of follow-up data. The mean follow-up period was 6 ± 1.1 years (range, 5-8.5 years). Clinical outcomes were assessed using the modified Lysholm score, the International Knee Documentation Committee (IKDC) subjective score, and the Tegner activity level. Radiographic progression of arthritis was measured by the absolute and relative joint space widths on 45° of knee flexion posteroanterior radiographs preoperatively, 1 year postoperatively, and at the latest follow-up.Failure was defined as meniscocapsular separation, removal, or tear of more than half of the meniscal allograft on postoperative magnetic resonance imaging (MRI) or conversion to total knee arthroplasty. Of the 18 patients, 3 underwent ≥2 RLMATs. The survival rate was evaluated according to the number of revision surgeries.
Results:
For knees with an intact meniscus transplant at the final follow-up, the modified Lysholm and IKDC scores were significantly improved compared with preoperatively, but the Tegner activity level was unchanged. No significant differences were found in the absolute and relative joint space widths postoperatively. There were 6 failures within 3 years after RLMAT; the overall 5-year survival rate was 68.4% (13/19 knees). All failed knees showed bucket-handle tear patterns on MRI due to meniscocapsular healing failure. The survival rate decreased as the number of RLMATs increased—73.3% for a first RLMAT (n = 15 knees), 66.7% for a second RLMAT (n = 3 knees), and 0% for a third RLMAT (n = 1 knee). Midterm MRIs of 8 well-healed RLMATs showed evidence of meniscal degeneration; nonetheless, this did not affect clinical outcomes.
Conclusion:
The midterm results of RLMATs demonstrated a 5-year survival rate of 68.4% and positive clinical and radiological outcomes for failed MATs despite unimproved activity levels. Inadequate meniscocapsular healing was the leading cause of failure, and it needs to be carefully considered when performing RLMATs.
Meniscal allograft transplantation (MAT) has been documented to be an effective treatment for painful subtotal or total meniscectomized knees in relatively young and active symptomatic patients.8,19,22 However, the overall failure rate of primary MAT was 10% to 29% at the mid- to long-term follow-ups, commonly defined as removal of the allograft or conversion to knee arthroplasty.8,19,24 The failure risk factors include articular cartilage status, thenumber of additional procedures required at the timeof MAT, and the time from meniscectomy to MAT.16,18,19,20,22 Revision MAT (RMAT) may be considered a treatment option for the failed MAT in young patients if they had stable nonarthritic joints adequate for MAT surgery. However, the prognosis of RMAT may be inferior to that of primary MAT because of poor intra-articular conditions, including periarticular scar tissues after previous procedures and aggravated articular cartilage status. 12
There have only been short-term studies investigating the clinical and radiological outcomes after RMAT. Yanke et al 29 reported that the International Knee Documentation Committee (IKDC) score and the Knee injury and Osteoarthritis Outcome Score for pain, patient satisfaction, and symptoms improved at a minimum 2-year follow-up.Lee et al 12 reported that the early failure rate of RMAT was high at 33.3% (3/9) during the first year, although the 6 remaining patients without failure experienced clinical improvement after RMAT.
To our knowledge, the midterm outcomes of revision lateral meniscal allograft transplantation (RLMAT) are unknown for this rare operation. In this study, we aimed to evaluate the midterm clinical and radiological outcomes of patients who underwent RLMAT. It was hypothesized that if meniscocapsular healing was attained in the early remodeling period, the midterm clinical and radiological outcomes of nonfailed RLMAT would be well maintained.
Methods
Patient Selection for RLMAT
Our institutional review board approved the protocol for this retrospective study. We reviewed 19 consecutive operated knees of 18 patients who underwent RLMAT at our hospital between 2010 and 2016. Patients with at least 5 years of radiological or clinical evaluation data were included. All patients (N = 18) underwent RMAT in the lateral compartment.
Fifteen of the 19 knees underwent a first RLMAT; 7 of the previous failed MATs were performed at our hospital by the senior author (S.-I.B.), and the other 8 had been performed at other institutions. The remaining 4 knees had already undergone RLMAT at other hospitals; 3 of the 4 knees underwent a second RLMAT, and 1 knee underwent a third RLMAT because the second RLMAT failed. The characteristics of the included patients are summarized in Table 1. Among the 19 knees in the present study, 6 failed in the early remodeling period—within 3 years after surgery. Therefore, clinical and radiologic evaluations were performed for the remaining 13 knees; all 13 knees underwent clinical assessment with patient-reported outcome measures, 9 were evaluated radiologically on standing radiographs, and 8 allografts were evaluated using magnetic resonance imaging (MRI). Of the 13 patients without failure, 4 did not undergo radiographic and MRI evaluations because they did not visit the outpatient clinic during the midterm period after surgery, and 1 patient refused to undergo MRI because of its cost. The clinical assessments for these 4 patients were performed through telephone consultations.
Demographic, Structural, and Clinical Characteristics of the Patients Who Underwent RLMAT (N = 18) a
Data are reported as mean ± SD (range) or No. of patients. ACI, autologous chondrocyte implantation; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; ICRS, International Cartilage Repair Society; LMAT, lateral meniscal allograft transplantation; OCD, osteochondral defect; RLMAT, revision lateral meniscal allograft transplantation.
Alignment was measured as a hip-knee-ankle angle, with positive and negative values indicating valgus and varus alignment, respectively.
Surgical Indications and Contraindications
Patients’ clinical histories were evaluated by checking the copies of the patients’ medical records and detailed history taking. Careful patient selection was performed by assessing clinical histories, physical examination results, and imaging techniques—such as radiography and MRI—to ensure successful RLMAT surgery. Patients <50 years old and capable of self-ambulation and performing activities of daily living, with a history of a failed lateral MAT (LMAT), and wishing to undergo the “salvage procedure” for their persistent, localized pain were deemed eligible for RLMAT. The indications for RLMAT were not different from those for the primary LMAT. Patients were considered suitable for RLMAT if they had a well-aligned mechanical axis within 3° valgus on long-leg standing radiographs covering the hip to the ankle, 2-mm preserved joint space on a 45° of flexion weightbearing posteroanterior radiograph, and a stable ligament status evaluated both clinically and on preoperative MRI. The contraindication of RLMAT was the complete disappearance of the joint space, ligament deficiency, or an uncorrected mechanical axis deviation toward the affected compartment.
Surgical Technique and Rehabilitation
All the lateral menisci were transplanted with size-matched fresh-frozen allografts with a bone block connecting the anterior and posterior horns using the keyhole technique.10,11 During the surgical procedure, the failed meniscal transplant was removed using arthroscopic techniques, and the remaining capsular rim was trimmed with a motorized shaver to promote healing. If bony spurs were observed on the lateral tibial plateau due to progressed arthritic changes, they were removed. A keyhole tibial slot was then created beneath the lateral tibial eminence with guidance from a C-arm intensifier, and a meniscal allograft was introduced through a small incision in the front of the joint. Once the best position for the allograft was determined, a traditional inside-out meniscal repair was performed using several nonabsorbable polyester braided sutures placed vertically about 3 to 5 mm apart. As an example, the serial images of a patient are shown in Figure 1.
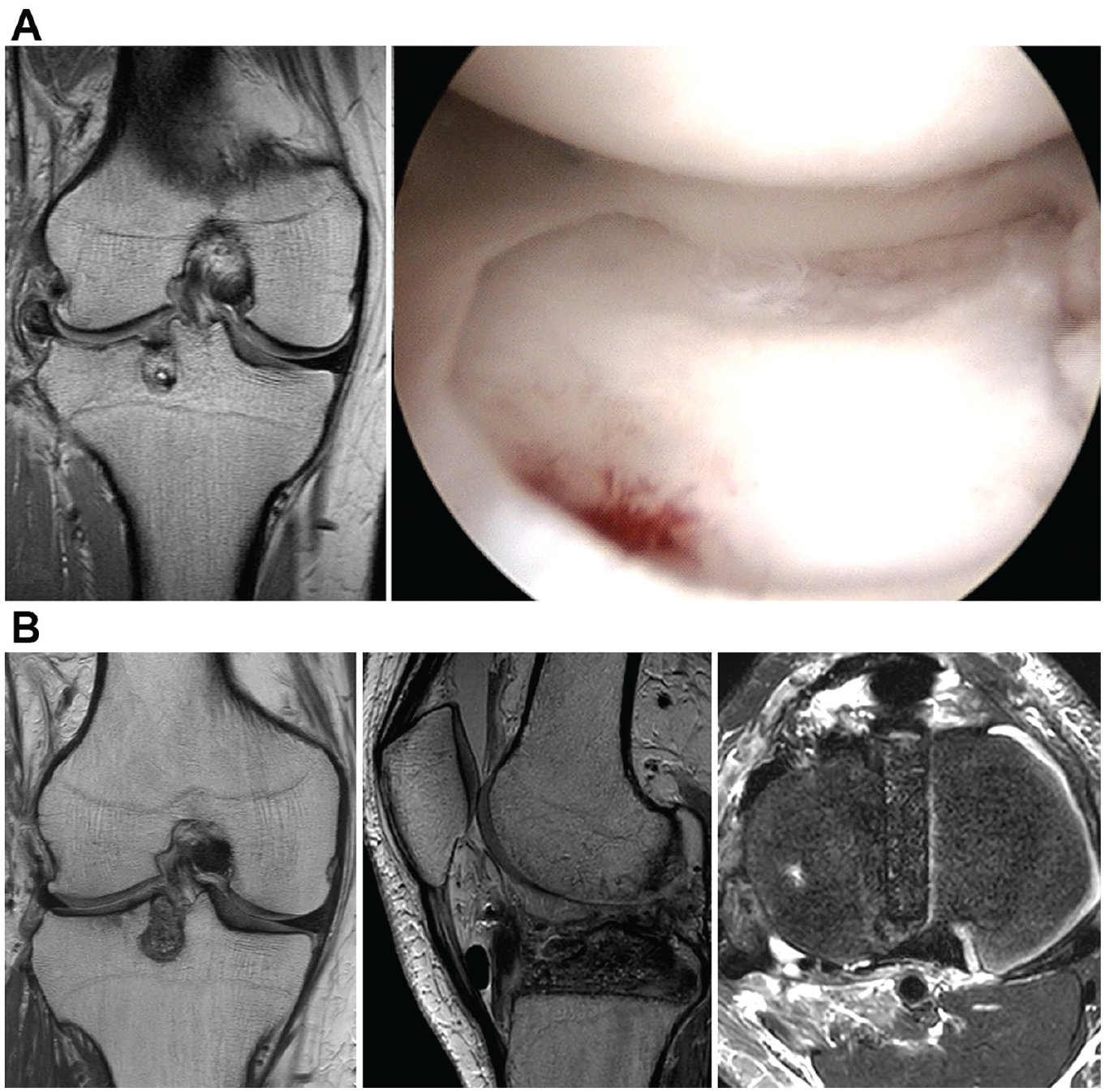
Serial MRI images of the affected side of the knee and arthroscopic examination at primary LMAT and RLMAT in a single patient. (A) Knee MRI and arthroscopic images after primary LMAT. The location of the tibial bone plug was quite lateral. Hence, severe graft extrusion was observed. (B) Knee MRI images before RMAT, graft extrusion, and midbody wearing out were observed, and the patient had severe pain at 9 years after the primary LMAT. Therefore, RLMAT was performed. Efforts were made to reduce graft extrusion by modifying the tibial bone plug through an angle and position different from those before RLMAT. LMAT, lateral meniscal allograft transplantation; MRI, magnetic resonance imaging; RMAT, revision meniscal allograft transplantation; RLMAT, revision lateral meniscal allograft transplantation.
At 1 to 2 days after surgery, the patients commenced continuous passive motion exercises. These range of motion exercises were performed to achieve full extension equal to that of the contralateral side within 1 week, 90° of flexion within 4 weeks, and 12° of flexion by 6 to 8 weeks. The patients were permitted only toe-touch weightbearing during the first 2 weeks after surgery, which was gradually increased to 50% weightbearing by the fourth week and to full-body weightbearing by the sixth week. The patients were advised to participate only in low-impact sports activities and light labor because of concerns regarding the deterioration of the meniscal transplants.
Clinical and Radiological Evaluations
Graft failure was defined as meniscocapsular separation, arthroscopic removal, or tear of more than half of the meniscal allograft confirmed on MRI or conversion to total knee arthroplasty. Clinical outcomes were assessed preoperatively, at 1 year postoperatively, and at the latest follow-up— minimum 5 years postoperatively—using the modified Lysholm score, the IKDC subjective score, and the Tegner activity level.2,6,23
The joint space width (JSW) values were compared on bilateral 45° of flexion weightbearing posteroanterior (Rosenberg) radiographs preoperatively, at 1 year postoperatively, and at the latest follow-up—minimum 5 years postoperatively. Images were acquired according to a standardized protocol to minimize the measurement error. The digital caliper in the picture archiving and communication system (PetaVision3D; Asan Medical Center) was used to measure the JSW values on radiographs. The absolute JSW value was measured at the center of the lateral compartment. In addition, to better standardize the findings between the patients, a relative JSW value was obtained by dividing the absolute JSW of the operated knee by the absolute JSW of the contralateral nonoperated knee.
All radiographic images were independently evaluated by 2 highly skilled orthopaedic surgeons (J.-H.S. and J.-S.C.). To increase data reliability, the data were measured every 2 weeks. Based on these data, the intra- and interobserver reliability of the JSW was evaluated using the intraclass correlation coefficient (ICC), with an ICC of 1 indicating perfect reliability and an ICC of 0 representing no agreement. The interobserver agreement was 0.897 on the absolute JSW and 0.879 on the relative JSW. The intraobserver agreement was 0.916 on the absolute JSW and 0.907 on the relative JSW.
Allograft status was evaluated on the MRI scans (Achieva 3T; Philips Healthcare) that were taken at 3, 6, and 12 months during the first postoperative year and then performed every 1 or 2 years if the patients agreed. MRI scans performed at 1 year postoperatively and at the latest follow-up after 4 years were used to evaluate changes in graft status. First, graft signal intensity was graded according to the method described by Stoller et al 26 : grade 0 (normal), grade 1 (globular increased signal intensity not adjacent to the articular surface), grade 2 (linear signal intensity within the meniscus), or grade 3 (increased signal intensity extended or communicated to the articular surface). Then, graft status was classified into 3 categories according to the integration and signal intensity of the meniscal transplants7,9,26: “satisfactory,” defined as complete healing with signal intensity grade ≤2 degeneration—with increased signal intensity due to linear intrasubstance that did not extend to the articular surface—of the graft; “fair,” defined as small, stable tears or insufficient healing without displacement; or “poor,” defined as gross tears or no meniscocapsular healing with or without displacement. Graft status was independently assessed by 2 orthopaedic surgeons (H.-K.C. and T.-H.K.). The Cohen kappa was used to assess the interrater reliability, and the results showed very good agreement (>0.80).
Statistical Analyses
All statistical analyses were performed using SPSS Version 21.0 (IBM Corp) with the statistical significance set at P < .05. The modified Lysholm and IKDC subjective scores were reported as means with standard deviations, and the Tegner activity levels were reported as medians with ranges. The Wilcoxon signed-rank test or Spearman rank correlation analysis (nonparametric paired test) was used to compare the changes in the clinical and radiological results between the 3 time points—preoperatively, 1 year postoperatively, and at the latest follow-up.The MRI grades at 1 year postoperatively and the latest follow-up were compared using the Spearman rank correlation analysis.
To determine the sample size required to detect differences in clinical scores (modified Lysholm score or IKDC subjective score) between preoperatively and latest follow-up of 1 sample group, α was set at .05, and power was set at 0.8. Using the mean and standard deviation of the pilot group preoperatively and at latest follow-up, the effect size was determined to be 0.8. A sample size of 12 knees was required to detect differences in the clinical scores of RLMAT at the 2 time points. The present study involved 13 knees that underwent RLMAT, and the power of the present study was 0.858 to reject the null hypothesis for clinical improvement, with a significance level of .05.
Results
Survival Rate After RLMAT
Across all 19 RLMATs included in the present study, 6 knees failed during the study period, and the overall survival rate at 5 years was 68.4% (13 of 19 knees). The survival rate decreased as the number of revisions increased: for a first RLMAT (n = 15 knees; 73.3%); a second RLMAT (n = 3 knees; 66.7%); and a third RLMAT (n = 1 knee; 0%) (Table 2). All 6 failed knees had bucket-handle tear patterns due to insufficient meniscocapsular healing within 3 years after surgery.
Rate and Possible Cause of Failure After RLMAT According to Number of Revisions a

ICRS, International Cartilage Repair Society; LMAT, lateral meniscal allograft transplantation; LTC, lateral tibial condyle; RLMAT, revision lateral meniscal allograft transplantation.
Poor host tissue quality: Tissue degenerated into hypovascular fibrotic tissue that causes healing failure of the meniscal allograft.
Severe arthrosis: ICRS ≥3 on both the femur and tibia sides during arthroscopy for failed revision allograft indicative of severe arthrosis.
Clinical and Radiological Results
The follow-up time for the clinical assessment of 13 patients without failure was 6 ± 1.1 years (range, 5-8.5 years). The modified Lysholm was significantly improved—from 56.7 ± 12.2 to 86.5 ± 10.2 (P = .003) at 1 year and 86.2 ± 5.9 (P = .001) at the latest follow-up—and IKDC subjective scores also improved—from 54.2 ± 10.5 to 66.2 ± 9.4 (P = .028) at 1 year and 69.6 ± 9.3 (P= .036) at the latest follow-up.These 2 clinical scores were maintained without significant changes during the midterm period (Figure 2). The Tegner activity level was not changed postoperatively.

A box plot showing the results of patients undergoing RLMAT from preoperatively to the 1-year and the final follow-up for (A) the Modified Lysholm score, (B) the IKDC subjective score, and (C) the Tegner activity level. *Statistically significant differences were seen in the follow-up modified Lysholm and IKDC subjective scores compared with preoperative scores (P < .05, Wilcoxon signed-rank test). The center line represents the median; the top and bottom of the box represent the first and third quartiles, respectively; the error bars represent 1.2 times the interquartile range; and the circles indicate outliers. IKDC, International Knee Documentation Committee; NS, nonsignificant; RLMAT, revision lateral meniscal allograft transplantation.
Midterm radiographic examination data were available in 9 of the 13 patients with an intact RLMAT at 5.8 ± 0.9 years (range, 5-7.5 years). When comparing the JSWs of the affected knees in the 45° of flexion posteroanterior standing view radiographs, no significant differences were found in the absolute and relative JSWs between all 3 time points (Figure 3). Also, 8 of the 13 patients with an intact RLMAT had MRI scans at the final follow-up.Three allografts showed meniscal degeneration during the midterm period at 5.2 ± 1.2 years (range, 4.1-7.5 years). However, the degenerative changes were not significant (Table 3).

A box plot showing the radiological results of RLMAT from preoperatively to 1-year postoperatively and the final follow-up for the 9 patients: (A) The absolute joint space width and (B) The relative joint space width. The center line represents the median; the top and bottom of the box represent the first and third quartiles, respectively; the error bars represent 1.2 times the interquartile range; the circles indicate outliers; and the asterisk indicates samples outside the normal distribution. NS, nonsignificant; RLMAT, revision lateral meniscal allograft transplantation.
MRI Changes of the Meniscal Allograft Status Between 1-Year Postoperatively and Latest Follow-up 4 Years After Surgery in 8 Patients a

MRI, magnetic resonance imaging.
Graft status was evaluated according to graft integration and the signal intensity of the meniscal transplants as described by Stoller et al. 26 Satisfactory = complete healing with signal intensity grade ≤2 degeneration of the graft; fair = small, stable tears or insufficient healing without displacement.
Discussion
The most important finding of the present study was that the subjective symptoms, as assessed by the Lysholm and IKDC subjective scores, could be improved after RLMAT in the patients who did not experience meniscocapsular healing failures. The clinical results of these well-healed RLMATs were sustained over the postoperative 5-year period. Insufficient meniscocapsular healing to host tissue in the early remodeling period was the main reason for refailure. Revision should be performed carefully, considering meniscocapsular healing problems.
The proven effect of primary MAT is improvement in patient-reported outcome measures in patients who had compartmental pain or effusion after subtotal or total meniscectomy.4,19,25,28 Vundelinckx et al27,28 reported that preoperative, postoperative midterm (7.5 years), and postoperative long-term (12.5 years) Lysholm scores were 39.6, 72.9, and 71.1, respectively, with continuously improving results after primary MAT. Lee et al 14 also reported that the long-term clinical outcomes remained improved, but a meaningful reduction of the JSW was observed in the long-term period. Unfortunately, the midterm (5- to 10-year) survival rate of primary MAT was 84% to 89.2%, but the long-term (>10 years) survival rates decreased3,8,15,19,25 from 45% to 73.5%. Therefore, revision should be considered in young patients if the primary MAT failed. However, to the best of our knowledge, there have been a few short-term studies after RLMAT for the failed primary LMAT,12,29 and the midterm clinical results have been lacking. In this present study for RLMATs, we observed that if meniscocapsular healing of the graft was achieved within the first 3 years, the subsequent prognosis was similar to that of the primary MAT, and the clinical and radiological results of the early period were well maintained in the midterm period without deterioration. Among the clinical parameters, the Tegner activity level did not improve after the operation; this was probably because we advised the patients to limit activity after surgery.
Early failure rates after RLMAT might be higher than after primary LMAT. One year after RMAT, graft failure was confirmed on MRI in 3 of 9 patients in a study by Lee et al. 12 Yanke et al 29 reported that after RMAT, 1 of the 8 patients underwent total knee arthroplasty at 34 months because of treatment failure. In the present study, graft failure occurred in 6 knees. It mostly occurred within 1 year, which is the healing period. The main failure mode was bucket-handle displacement with meniscocapsular healing problems due to poor host tissue quality. As the number of RLMATs increased, the survival rate decreased and failure occurred earlier. Therefore, if host tissue qualityis poor due to scaring by previous surgical tissue damage, augmentation for meniscocapsular healing—such as synovial abrasion, 17 fibrin clot, 5 and platelet-rich plasma 1 —should be considered. After RLMAT, clinicians should focus more on the graft healing to host tissue during rehabilitation, 13 and we recommend early MRI scans within 1 year to detect healing failures in such patients. 21 The MRI scans showed some degenerative signal changes in the meniscal allograft in 3 of 8 healed knees; therefore, longer-term observation is necessary for larger series.
Limitations
This study has several limitations. First, a small number of cases and some patients who did not undergo midterm radiographic and MRI examinations limited the generalization of radiological results and the survival rate after RLMATs. These were rarely indicated in clinical practice to collect enough sample size. Nonetheless, we found a statistically significant increase in clinical outcomes among patients who achieved meniscocapsular healing. Second, this was a retrospective study without a control group.Therefore, we could not determine the superiority of RLMAT over other treatments—such as osteotomy, arthroplasty, or conservative treatment. Third, only RLMATs were included. Thus, our results cannot be generalizable to medial RMATs.
Conclusion
The midterm results of RLMATs demonstrated a 5-year survival rate of 68.4% and provided clinical and radiological benefits for failed MATs despite unimproved activity levels. Inadequate meniscocapsular healing is the leading cause of failure, and it needs to be carefully considered when performing RLMATs.
Footnotes
Final revision submitted June 12, 2023; accepted June 21, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (ref No. 2020-1813).