
Abstract
Background:
Bone–patellar tendon–bone (BTB) anterior cruciate ligament reconstruction (ACLR) is one of the conventional techniques in the revision setting especially after a primary hamstring tendon graft. The use of the iliotibial band (ITB) augmented with allograft (AG) is an encouraging graft alternative for ACLR in terms of clinical and biomechanical data in the literature.
Purpose:
To compare the clinical outcomes of BTB graft with lateral extra-articular tenodesis, modified Lemaire (BTB-LET), and an ITB graft augmented with hamstring AG (ITB-AG) in the setting of revision ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Descriptive data and clinical outcomes were prospectively collected from patients who underwent revision ACLR with either the BTB-LET or ITB-AG technique between 2012 and 2020 and who had a minimum follow-up of 2 years. The clinical outcomes were assessed by the Lysholm, Tegner, Anterior Cruciate Ligament–Return to Sport after Injury, International Knee Documentation Committee subjective knee evaluation form, and Knee injury and Osteoarthritis Outcome Score. Return to sports, complications, and revisions were also analyzed.
Results:
A total of 167 patients were included, with 106 patients in the BTB-LET group and 61 patients in the ITB-AG group. There were no significant group differences in sociodemographic characteristics; however, the mean follow-up was significantly longer in the BTB-LET compared with the ITB-AG group (52.0 vs 38.8 months, respectively; P = .0001). There were no significant differences in postoperative outcome scores; however, patients in the ITB-AG group had a higher rate of return to competitive pivoting sports (32.8% vs 17.9%; P = .0288) and a higher overall rate of return to preinjury sport (63.9% vs 47.2%; P = .0365). Complications, including revisions for meniscal or chondral lesions and retears (8 [8.3%] in the BTB-LET group and 2 [4.0%] in the ITB-AG group), were not significantly different. All retears were due to sports-related accidents.
Conclusion:
In this study, ITB-AG was not different from BTB-LET in terms of functional outcomes scores but allowed better return to sport rate. Performing ITB-AG reconstruction in the setting of revision ACLR appears to be safe, effective, and associated with a satisfying return-to-sports rate.
Keywords
Graft choices in the revision setting of anterior cruciate ligament reconstruction (ACLR) remain challenging and depend on the initial failed graft. Worse clinical outcomes, despite all research improvements, have been demonstrated in comparison with outcomes after primary surgery.1,4,12,32,49 Poor patient-reported outcomes have been shown to be related to recurrent anterior knee instability and rotational instability.30,35 Hamstring tendon graft is still one of the most used grafts for primary ACLR worldwide. 47 Moreover, bone–patellar tendon–bone (BTB) ACLR is one of the conventional techniques in the revision setting, especially after a primary hamstring tendon graft. 45
When ACL rupture is combined with anterolateral structure injury, ACLR alone fails to restore knee kinematics.23,44 Anterolateral ligament reconstruction or lateral extra-articular tenodesis (LET) are often used for ACL revision surgery to control rotational instability and lower the rate of rerupture. 2 Studies have revealed that LET improves clinical and radiological outcomes particularly in the revision setting, which is the only setting to be considered a validated indication for LET.37,40,43,52 The control of rotatory instability reduces the rate of secondary meniscal injury and may slow the development of osteoarthritis.14,21,51
LET techniques started with Lemaire, as he used the iliotibial band (ITB) for isolated extra-articular reconstruction, 31 and later with MacIntosh for intra- and extra-articular reconstruction. 3 Several surgeons have modified the MacIntosh ITB technique because of lower biomechanical forces when used alone26,29 and have described intra-articular augmentation with both 15 or single 13 hamstring tendons, specifically the combined ITB and semitendinosus tendon technique described by Zarins and Rowe in 1986. 53 The use of the ITB in revision ACLR is of great advantage in terms of shortage of grafts and allows ACLR and LET to be achieved from a single harvest site while potentially preserving the knee's flexion and extension mechanisms. 19 Thus, reducing anterior knee pain associated with BTB techniques as well as a natural fixation to Gerdy tubercle.19,20
To the best of our knowledge, there are no studies evaluating the functional outcome of revision ACLR using the ITB augmented with allografts (AGs). Moreover, the comparison of revision ACLR with augmented ITB versus BTB revision ACLR associated with LET has never been examined before. Therefore, the primary target of this study was to compare the functional outcomes of revision ACLR surgeries using the 2 techniques. The secondary goals were to compare both groups’ return to sports, rate of complications, and rate and delay of re-rupture. Our hypothesis was that the functional outcome after revision using augmented ITB would not be different from that after revision with BTB autografts with LET.
Methods
Patient Population
Data were collected from the FAST (French prospective Anterior Cruciate Ligament Reconstruction) cohort, a study to examine patients who had undergone anterior and/or posterior cruciate ligament and/or multiligament reconstruction to determine the rate of reinjury and contralateral tear and functional outcomes at least 2 years after surgery (registered on ClinicalTrials.gov) between 2012 and 2020. The study protocol was approved by the local ethics committee, and all patients provided informed consent. All patients over 18 who underwent surgery operated by 6 senior surgeons (A.G., A.M., O.G., N.L., Y.B., A.H.) for a first revision ACLR after a primary reconstruction using a hamstring autograft, with or without a meniscal lesion, using an ITB graft augmented with AG (ITB-AG) or a BTB autograft associated with LET with an iliotibial band (BTB-LET), and who had ≥2 years of follow-up data were included. The choice of the revision technique was made according to the surgeon's preference and experience. Exclusion criteria were a history of primary reconstruction using a graft other than hamstring autograft, patients with inappropriate tunnel position or enlargement, other revision techniques, multiple revisions, refusal to participate in the study, another associated ligament reconstruction procedure (medial collateral ligament, lateral collateral ligament, posterior cruciate ligament), or associated osteotomy.
Initially included in the study were 143 patients who underwent BTB-LET and 74 patients who underwent ITB-AG. Of these patients, 37 (25.87%) in the BTB-LET group and 13 (17.57%) in the ITB-AG group were lost to follow-up; thus, the statistical analysis was carried out on 106 patients and 61 patients in the BTB-LET and ITB-AG groups, respectively (Figure 1).

Flowchart illustrating population selection. ACL, anterior cruciate ligament; AG, allograft; BTB, bone–patellar tendon–bone; FAST, French prospective Anterior Cruciate Ligament Reconstruction cohort; ITB, iliotibial band; LET, lateral extra-articular tenodesis.
Surgical Techniques
Revision ACLR Using BTB-LET
Revision ACLR using BTB-LET (Figure 2) was performed arthroscopically with grafts in a single bundle: harvesting of the central portion of the patellar tendon with patellar and tibial bone plugs being sized at a 9-mm width/20-mm length and 10-mm width/30-mm length, respectively. Intra-articular reconstruction is done by inside-out guidance on the femoral side through the standard anteromedial portal with size-to-size tunnel followed by the tibial tunnel. Femoral fixation is either by interference screw or Rigid fix system (Mitek), whereas tibial fixation is by interference screw (Softsilk; Smith & Nephew).

Illustration of revision anterior cruciate ligament reconstruction using bone–patellar tendon–bone graft with lateral extra-articular tenodesis.
For the LET, a strip of ITB of approximately 7 cm in length and 2 cm in width was harvested but remained attached to the Gerdy tubercle and then fixed on the lateral femoral condyle at an isometric point (Krakow point) through a transversely drilled tunnel using a bioabsorbable screw (BioSure; Smith & Nephew). The BTB-LET reconstruction is similar to the technique described by Rayes et al 42 using the BTB autograft and modified Lemaire LET.
Revision ACLR Using ITB-AG
After the preparation of the 7-mm tibial tunnel, an ITB of approximately 16 cm in length, 12 mm in width distally, and 35 mm proximally was harvested and kept pediculated to the Gerdy tubercle (Figure 3). The band was reinforced by a double-banded single AG of the semitendinous tendon. The assembly was tubularized and sutured by Vicryl sutures (Ethicon) leaving 2 tractor wires. No fixation was used in the femoral tunnel for the ITB-AG. The graft was then calibrated to ~7 mm for the tibial tunnel and ~9 mm for the femoral tunnel. Realization of a 9-mm outside-in femoral tunnel through an entry point just proximal and posterior to the lateral collateral ligament insertion and the exit point was controlled intra-articularly in the proper position. The graft was then passed in an antegrade manner toward the tibia where it was fixed by an interference screw at 30° of flexion and after cycling of the knee. The technique is similar to the technique described by Dos Santos et al, 13 with the difference being the ITB reinforcement by semitendinosus AG in our revision setting as compared with theirs by the gracilis tendon.

Illustration of revision anterior cruciate ligament reconstruction using iliotibial band graft augmented with hamstring allograft.
Postoperative Rehabilitation
The postoperative protocol was identical for the 2 groups. All patients were allowed weightbearing as tolerated in a protective articulated knee brace with unrestricted range of motion in addition to 2 crutches until they could ambulate using a normal gait. An exception was that the patients with a lateral meniscal injury who underwent partial lateral meniscectomy were allowed partial weightbearing for 4 to 6 weeks depending on the meniscal intervention performed. Physical therapy was started within days after the surgery to regain full knee extension. All patients were evaluated at 4 weeks postoperatively. Return-to-play criteria were determined by regular follow-up of the patients in terms of time factors; psychological readiness; and performance, functional, and strength tests (hop tests, dynamic valgus, and isokinetic tests). 28 Patients were allowed to return to nonpivoting sports at 4 months. Gradual return to pivoting sports was permitted at 6 months for noncontact sports and 9 months for contact sports.
Objective muscle strength criteria used to determine return to running were isolated strength evaluation of quadriceps (limb symmetry index >70%), quadriceps/body weight >1.45 N·m/kg, single-leg press >1.25 times body weight, seated calf raise >1.5 times body weight, and heel raise endurance >25 repetitions.8,39 Functional performance-based criteria included single-leg landing capacity. 22 Clinical evaluation included pain <2 of 10 on a numeric pain rating scale, absence of effusion or trace, knee flexion 95% limb symmetry index, and full knee extension. 41
Clinical Evaluation Protocol Before and After Revision ACLR
For both groups, preoperative evaluation consisted of recording patients’ sociodemographic characteristics, sport level (professional, competitive, regular leisure, occasional leisure, and sedentary) and sport type (contact pivoting, noncontact pivoting, nonpivoting, no sport) as well as the Lysholm, Tegner rating system, 7 Knee injury and Osteoarthritis Outcome Score (KOOS), 11 the ACL–Return to Sport after Injury (ACL-RSI), 5 and International Knee Documentation Committee (IKDC) subjective knee scores. 24 Postoperatively, patients completed the same functional outcome measures, and they rated their satisfaction (very satisfied, satisfied, somewhat satisfied, or not satisfied) and provided return-to-sport data: return to running, pivoting sport, competitive pivoting sport, and preinjury sport as well as any delays in returning to these sports. Patients received an email containing a link to a questionnaire with the electronic version of the outcome measures, which were then managed using Websurvey.fr software. The postoperative questionnaire was completed at 6 months and then at 1, 2, 4, 6, and 8 years after surgery.
Primary and Secondary Outcome Measures
The primary outcome measure for this study was the clinical outcomes as evaluated by the functional scores (IKDC, KOOS, Lysholm, Tegner, and ACL-RSI). The secondary outcome measures were return to sport, the complication rate, and the rate and delay of rerupture.
Statistical Analysis
For qualitative data, comparisons were made using the chi-square test or Fisher exact test, according to the expected values under the assumption of independence. Comparisons of quantitative data were made using the Student test or Mann-Whitney-Wilcoxon test (nonparametric test comparing ranks) depending on the distribution of the variable of interest. All comparisons were performed at the level of statistical significance set at P < .05.
All calculations were made with SAS for Windows (Version 9.4; SAS Institute).
Power analysis was conducted with the 2-sided Z test with pooled variance. The significance level of the test was .05. Group sample sizes of 61 in the ITB-AG group and 106 in the BTB-LET group achieved 80.02% power to detect a difference between the group proportions of 19%.
Results
Patient Characteristics
The preoperative data were demographically and anthropometrically similar in both the BTB-LET and ITB-AG groups. Surgical data were similar in both groups regarding time between injury and the revision surgery, meniscal lesions, and chondropathy (Table 1). All preoperative scores were similar between groups, with the exception of ACL-RSI (32.90 ± 27.27 in BTB-LET vs 40.89 ± 22.15 in ITB-AG; P = .0141) (Table 2).
Sociodemographic and Surgical Characteristics a

Data are reported as mean ± SD or n (%). BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; ITB-AG, iliotibial band graft augmented with hamstring allograft.
Student test.
Chi-square test.
Wilcoxon test.
Preoperative Data a

Data are reported as n (%) or mean ± SD. Boldface P value indicates statistically significant difference between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; IKDC, International Knee Documentation Committee; ITB-AG, iliotibial band graft augmented with hamstring allograft; KOOS, Knee injury and Osteoarthritis Outcome Score.
Contact pivoting sports: football, handball, basketball, rugby, hockey, judo, karate.
Noncontact pivoting sports: ski, tennis, squash, badminton, volleyball, roller skating, gymnastics.
Nonpivoting sports: running, biking, swimming, golf, hiking, horseback riding, climbing.
Chi-square test.
Fisher exact test.
Student test.
Wilcoxon test.
Functional Outcomes
After a mean follow-up of 52 months for the BTB-LET group and 38.8 months for the ITB-AG (P = .0001), there were no significant differences in the functional scores (IKDC subjective, KOOS, Lysholm, Tegner) and the psychological ACL-RSI score between the 2 groups. The loss of follow-up was significantly more in the BTB-LET group (25.87%) compared with 17.57% in the ITB-AG group. However, there was no statistical significance between both groups (P = .1684). In both groups, the level of satisfaction was also similar. Results are presented in Table 3.
Functional Results and Return to Sport a

Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; IKDC, International Knee Documentation Committee; ITB-AG, iliotibial band graft augmented with hamstring allograft; KOOS, Knee injury and Osteoarthritis Outcome Score. Nonpivoting sports: running, cycling, swimming, golf, hiking, riding, climbing. Noncontact pivoting sports: ski, tennis, squash, badminton, volley, roller skating, gymnastics. Contact pivoting sports: football, handball, basketball, rugby, hockey, judo, karate.
Wilcoxon test.
Student test.
Fisher exact test.
Chi-square test.
Return to Sport
At the final follow-up, the functional results in terms of delay to return to running and return to pivoting sports were similar in both groups. On the other hand, the ITB-AG group had a significantly higher rate of return to competitive pivoting sport (32.8%) compared with the BTB-LET group (17.9%) (P = .0288) after a mean of 14.2 and 14.6 months, respectively. The ITB-AG group also had a higher rate of return to the same preinjury sport (63.9%) versus the BTB-LET group (47.2%) (P = .0365), after a mean of 11.7 and 10.1 months, respectively.
The level of play as compared with the preoperative status at the final follow-up was the same or better in 23.6% of patients in the BTB-LET group and in 39.4% of the patients in the ITB-AG group (P = .2200; nonsignificant). In the BTB-LET group, 18.9% of the patients changed sports compared with 14.8% in the ITB-AG group (P = .2200; nonsignificant), and 21.7% discontinued playing sports in the BTB-LET group compared with 13.1% in the ITB-AG group (P = .2200; nonsignificant). Results are presented in Table 3. The demographics of the patients according to their level of play as competitive or not are illustrated in Table 4. The mean age at surgery was significantly younger in competitive patients (P = .0001).
Sociodemographic Characteristics of the Competitive and Noncompetitive Patients a

Boldface P value indicates statistically significant difference between groups (P < .05).
Student test.
Chi-square test.
Complications
There was no significant difference in the revision rate for meniscal or chondral surgery. At the final follow-up, 8 retears (8.3%) occurred in the BTB-LET group and 2 (4.0%) in the ITB-AG group (P = .4947; nonsignificant); all were traumatic lesions after sports accidents and confirmed by magnetic resonance imaging (MRI) (Table 5). One patient in the ITB-AG group underwent reoperation for wound complications. One patient in the BTB-LET group underwent reoperation for a cyclops lesion. None of the cases of postoperative hematoma or wound complications required surgical revision. Between surgery and final follow-up, 13 patients in the BTB-LET group and 8 patients in the ITB-AG group were evaluated for a contralateral ACL tear (P = .6889; nonsignificant).
Postreconstruction Complications a
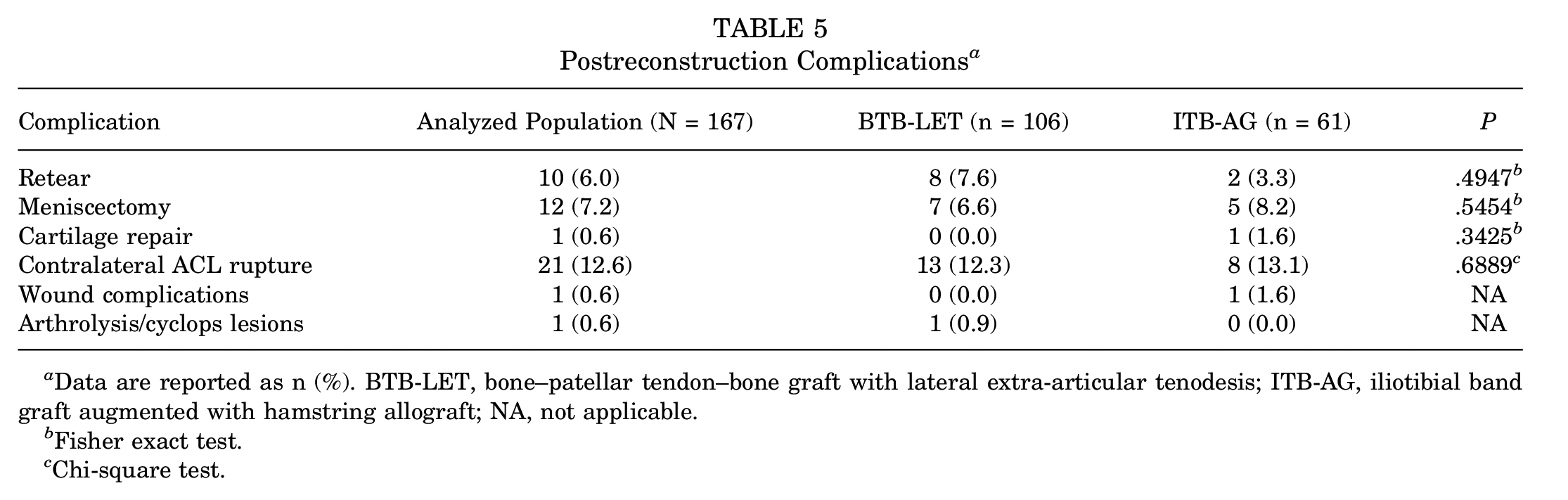
Data are reported as n (%). BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; ITB-AG, iliotibial band graft augmented with hamstring allograft; NA, not applicable.
Fisher exact test.
Chi-square test.
The characteristics of the patients with retears were not significantly different from the ones with intact grafts (Table 6). Furthermore, time to ligament failure was comparable in both groups; the retear-free event rates at 84 months postoperatively in the BTB-LET and ITB-AG groups were 87.6% and 82.4%, respectively (Table 7 and Figure 4).
Characteristics of Patients With Confirmed Retears

Student test.
Fisher exact test.
Time to Ligament Failure a
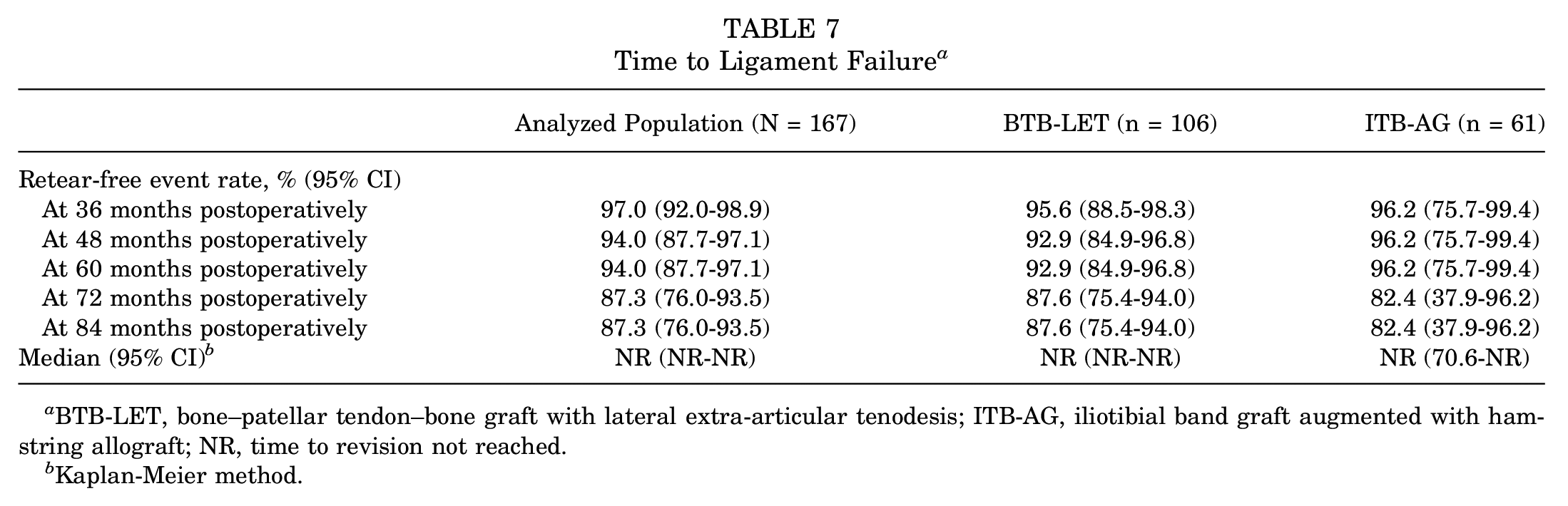
BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; ITB-AG, iliotibial band graft augmented with hamstring allograft; NR, time to revision not reached.
Kaplan-Meier method.
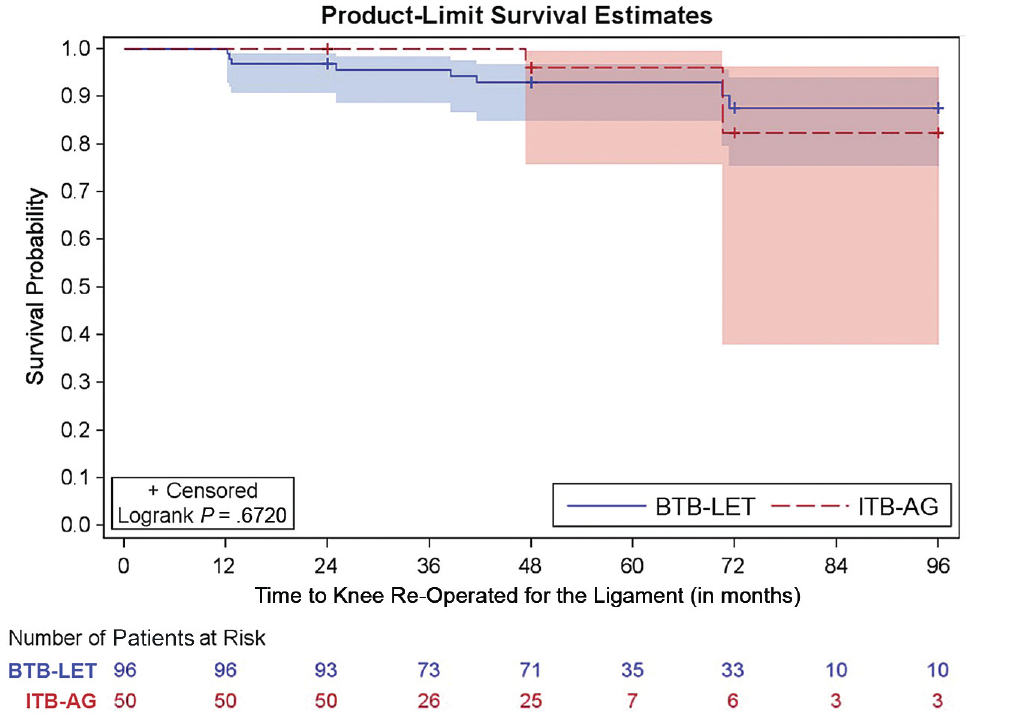
Survival probability according to revision anterior cruciate ligament reconstruction technique. Shaded areas indicate 95% CIs. BTB-LET, bone–patellar tendon–bone graft with lateral extra-articular tenodesis; ITB-AG, iliotibial band graft augmented with hamstring allograft.
Discussion
The main result of this study was that the functional outcomes after revision ACLR with the ITB-AG technique were not different from those with BTB-LET at minimum 2-year follow-up. There were no significant differences in the IKDC subjective score; the KOOS and its subcategories; and the Lysholm, Tegner, and ACL-RSI scores. Furthermore, a low rate of retear and time to retear were quite comparable in both groups. These results support previous studies of direct comparison concerning the use of fascia lata versus BTB autograft in terms of functional outcomes (Tegner score), and rate of graft failure. 46 In fact, this is the first study to date comparing clinical outcomes in the setting of revision for an AG reenforced ITB versus BTB in a population cohort.
The Multicenter ACL Revision Study large cohort of patients with revision ACL reconstruction at a minimum 6-year follow-up showed superiority of BTB autografts over BTB AGS in terms of sustainability and function whereas no significant difference in risk of graft rupture among BTB autograft and soft tissue AGs. 36 The authors of that study did not provide an explanation for these data, and a limitation of this study is that it is purely based on patient-reported outcome measures, without objective data. In a study published in 2003, Johnston et al 26 performed over-the-top, open ligament reconstruction with an ITB graft alone in the primary reconstruction setting. They reported a Lysholm score of 81 ± 17.3 at the final follow-up, compared to 81.49 ± 20.24(81.5 ± 20.2) in our series, and 54% of the patients did not return to the same level of sports as before the injury in both series.
Return to sports, mainly competitive pivoting sports and preinjury level, as secondary results in our study were better in the ITB-AG group. Return to sports is one of the main goals of ACL surgery. No significant studies are present in the literature that discuss return to sport after primary ACLR using fascia Lata. However, in the setting of revision, Mirouse et al 38 reported in their study that 12 of 30 sports players who underwent a revision surgery with ITB returned to their sport at the same level. 38 In their recent systemic review, Glogovac et al 17 also concluded that the rate of return to sport at preinjury level ranged from 13% to 69% and that athletes may have difficulty resuming their previous level of sport after revision ACLR but have a good chance of returning to a lower level of play. A 2015 meta-analysis showed that 51% of patients returned to competitive sport after revision ACLR, and our results are quite similar to those results. 18 Return to sport after a revision surgery is multifactorial. Psychological factors are of importance here and not to be ignored. 16 We assume that the morbidity regarding harvest site is one of the major factors for the low rate of RTS in the BTB-LET group. Rigidity of the fascia lata and initial traction resistance (3266 N) are important factors also, as reported by Chan et al, 9 who have conducted their studies on wider fascia lata grafts as compared with ours. Furthermore, the ITB-AG technique provides a continuous graft that is left attached to the Gerdy tubercle, and this technique provides anatomic attachment without the need to drill and weaken the proximal tibia. In addition, this attachement provides a vascular supply necessary for the ligamentization process of the graft. 10
In terms of complications, there was no significant difference in the rerupture rate and revision rate for either meniscal or chondral surgery. ITB-AG showed a good safety profile due to the significant low rate of complications. These results were also shown in a few previous studies9,25,32,37 that evaluated revision ACLR using the ITB and reported no specific postoperative complications except for hematomas, material protrusion, and muscular hernias, 38 which we did not encounter in our series. In the most recent systematic review, dated 2022, Lucena et al 33 reported that a comparison of 89 ITB versus 80 BTB autografts revealed no significant differences in graft failure, instrumented mean side-to-side knee laxity difference, or Tegner score. However, this analysis was from the results of primary setting of ACL Reconstruction. Time to ligament failure was comparable in both groups. There were no infections in either group, which is expected with the systematic use of vancomycin-soaked grafts. 6 The high rate found in the current study of contralateral ligament rupture, 14.7%, confirmed during regular patients’ follow-up and MRI after a trauma event, approaches the rates of recent literature. In their systemic review, Magnussen et al 34 mentioned that an overall risk of ACL injury in the contralateral limb was 12.5%. The background for these contralateral injuries may be multifactorial and beyond the scope of our study. 50
The use of ITB in revision ACLR was according to surgeon's preference. The discussion of the advantages of this technique can be summarized in the benefit of achieving the ACL revision and LET with a single continuous graft from a single harvest site while avoiding significant complications associated with harvesting of the patellar tendon—specifically, anterior knee pain or patellar fractures.19,20 It is worth mentioning that other surgeons use the quadriceps tendon with or without bone block in the revision settings to minimize this anterior knee pain, 49 but the discussion of this technique is outside the scope of our study. The attachment to the Gerdy tubercle provides vascularization essential to graft ligamentization. 10 On the other hand, the disadvantages of the ITB-AG technique, according to complications mentioned in the literature, are mainly hematoma, the 6-cm lateral incision, and nonsurgical muscle hernia at the harvest site13,27; however, thanks to the good closure layer by layer and tightly of the harvest site according to Jaecker et al 25 and Khiami et al, 29 we did not encounter hematomas or muscular hernias. The technique is relatively demanding, needs a learning curve, and requires relatively longer operative time. During the follow-up period of our patients, we did not encounter long-term consequences concerning this technique.
Limitations and Strengths
One of the limits to our study is that we did not report objective measurements of anteroposterior (Lachman test) or rotatory (pivot-shift test) instability. However, this was not the goal of our study, which was focused on the functional outcome reported by patients. Another drawback is that the difference between the preoperative psychological ACL-RSI score between the study groups could have influenced the results of this study. However, this difference was <13.4, the threshold of the minimal clinically important difference established by Webster and Feller. 48 In addition, a survival analysis was performed to report the time of incidence of the rerupture.
Another limit is the absence of comparative imaging. Indeed, 1 cadaveric study 25 showed a potential risk of tunnel convergence during ACLR associated with LET. This ITB technique eliminates the risk with a single femoral tunnel and a continuous intra- and extra-articular reconstruction. The follow-up period was also limited to 8 years, and postoperative long-term complications such as osteoarthritis could not be observed. Furthermore, the loss of follow-up was significantly more in the BTB-LET group (25.87%) compared with 17.57% in the ITB-AG group. However, there was no statistical significance between both groups (P = .1684). The difference in follow-up time with 52.0 months for the BTB-LET group and 38.8 months for the ITB-AG (P = .0001) is also considered a drawback to this study, and this can be explained with the relatively recent use of this technique compared with the more conventional BTB-LET technique.
Despite these limitations, the strength of our study is that it includes many patients and is monocentric, with regular follow-up of patients with patient-reported outcome measures. In addition, this is the first study evaluating a revision ACLR technique with an ITB augmented with AG and offers a comparison with conventional BTB-LET technique for the risk of retear over a relatively long period in terms of revision ACLR.
Conclusion
Revision ACLR with the ITB augmented in the intra-articular portion by AG provides the same functional results as BTB-LET and better results in terms of return to competitive pivoting sports.
Footnotes
Final revision submitted May 29, 2023; accepted June 7, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Comité de Protection des Personnes—Ile-de-France VI, Groupe Hospitalier Pitie-Salpetriere.