
Abstract
Background:
Anterior cruciate ligament (ACL) reinjury after ACL reconstruction (ACLR) can occur on the ipsilateral or contralateral side. Limited evidence exists regarding the difference between the incidence of reinjury to either knee, which is important in developing interventions to prevent ACL reinjury.
Purpose:
To compare the reinjury rate of the ACL on the ipsilateral side versus the contralateral side in athletes after ACLR and investigate the risk factors that may cause different reinjury rates between the sides.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies that involved ACL reinjury in athletes after ACLR were reviewed. Considering several risk factors, including age and sex, a comparison of ACL reinjury incidence on the ipsilateral and contralateral sides was performed using a meta-analysis.
Results:
Of the 17 selected studies, 3 were found to be at high risk of bias, and thus, 14 (n = 3424 participants) studies were included in the meta-analysis. In this athletic population, the contralateral ACL had a significantly higher rupture rate than the ipsilateral graft (risk ratio [RR], 1.41; P < .0001). Female athletes were found to have a greater risk of ACL reinjury on the contralateral versus the ipsilateral side (RR, 1.65; P = .0005), but different results were found in male athletes. (RR, 0.81; P = .21). There was no statistical difference in the incidence rate of ACL reinjury to either side in adolescent athletes (RR, 1.15; P = .28).
Conclusion:
The contralateral ACL was more vulnerable to reinjury than the ipsilateral side in athletes after ACLR. Female athletes were more likely to reinjure their contralateral native ACL, while the same trend was not found in their male counterparts. The reinjury rate was comparable in both knees in adolescent athletes.
Athletes represent one of the highest risk groups for anterior cruciate ligament (ACL) injuries.48,50,60,67 Anterior cruciate ligament reconstruction (ACLR) is commonly recommended for primary ACL rupture to regain stability and facilitate return to sport (RTS).18,32,48,69 However, athletes were also reported to be considerably more susceptible to ACL reinjury,40,53,54,74 including ipsilateral and contralateral side reinjuries. Patients with ACL reinjury have worse functional and radiological results than those with a primary ACL injury as well as heavier psychological and economic burdens.56,58,75 Therefore, ACL reinjury was considered one of the most devastating complications after ACLR. As a result, fewer athletes returned to their preinjury sport level after ACL reinjury.25,71
In terms of ACL reinjury, earlier studies paid more attention to the ipsilateral side after ACLR but ignored the contralateral side. Contralateral ACL reinjury was a double blow to patients physically and psychologically, the rate of which may be as high as the ipsilateral side.1,12,35,39,61,62,70,73,77 Thus, recently, ACL reinjury of the contralateral side has received extensive attention clinically. 42 The answer to the question, “Is the contralateral side exposed to a higher risk of ACL reinjury than the ipsilateral side?” may help develop RTS criteria and more targeted rehabilitation designed to prevent ACL reinjury. Increased knowledge regarding this question would also assist in counseling patients about the expected outcome after ACLR and RTS.
However, conflicting results were reported in previous studies regarding this question. Wright et al 77 showed that after a minimum 5-year follow-up, the reinjury rate of the contralateral side was approximately twice as high as the ipsilateral side (11.8% vs 5.8%), which was also supported by Paterno et al. 55 Conversely, some studies have found no significant differences in the ipsilateral and contralateral sides.3,33,52 In addition, few previous studies considered whether young age and sex play an equal role in ipsilateral and contralateral reinjury, which have been reported to be risk factors for overall ACL reinjury,8,9,42,45,72 especially in an athletic population.42,76
This systematic review aimed to (1) compare the ACL reinjury rate of the ipsilateral and contralateral sides in athletes after ACLR and (2) investigate whether young age and sex are factors of the differences observed between ipsilateral and contralateral ACL reinjury. The hypothesis was that the contralateral ACL would be at a higher risk of reinjury than the ipsilateral ACL in athletes after ACLR, regardless of sex, and that there would be no difference between the reinjury rate in adolescent athletes.
Methods
A meta-analysis was performed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 46 The protocol of this systematic review (ID: CRD42020215970) was registered on the PROSPERO database.
Literature Search and Selection
Two authors (H.G., H.H.) independently searched the PubMed and OVID databases using the following terms: “anterior cruciate ligament reconstruction,”“ACL reconstruction” OR “ACLR” combined with “reinjury,”“second injury,”“consequent injury,”“graft failure” OR “re-rupture” OR “retear.” Only studies in English were included. The publication date was not limited, and the references to included studies were reviewed for additional sources. Review articles, technique reports, and biomechanical and animal studies were excluded.
After removing duplicates, the same 2 reviewers independently screened the titles and/or abstracts of the studies. The full texts were obtained when the titles and abstracts provided vague or insufficient information. Any disagreement was resolved by consensus between the 2 reviewers while a senior professor specialized in sports medicine (S.C.) joined the discussion if necessary.
Specifically, the included articles needed to provide outcomes of interest—such as population characteristics, follow-up time, overall reinjury rates, contralateral reinjury rates, ipsilateral reinjury rates, and reinjury events in terms of sex (if reported). Studies that did not publish results of an athletic group and studies that involved the same cohort were excluded. Corresponding authors of articles were contacted for unpublished data as needed.
Study Quality Assessment
Two authors (H.G. and H.H.) independently assessed the risk of bias for each included study. A discussion was required when any disagreements occurred. Domain-based tools were used to assess the risk of bias, including the Cochrane Risk of Bias 2 tool 66 for randomized controlled trials (RCTs) and the Risk of Bias Assessment tool for Nonrandomized Studies 37 for observational studies. Specifically, an RCT was judged to be at high risk of bias if at least 1 domain had an increased risk of bias, and it was considered to have some concerns if ≥3 domains were considered to be at high risk of bias. 66 A non-RCT was judged to be at high risk of bias if at least 2 domains were rated as high risk or uncertain. 37
Data Extraction
The data were sorted and compiled within a collection form. Two authors (H.G. and H.H.) independently performed data extraction, and disagreements were discussed until a consensus was reached. The basic study data—including authors, study design, published year, patient characteristics, and follow-up period—were recorded. Relevant variables of interest were also extracted—including overall ACL reinjury and both the ipsilateral and contralateral ACL reinjury rates. Moreover, specific data—including patient age distribution, sex distribution, and follow-up times of patients with ACL reinjury—were discussed.
Statistical Analysis
Only small number of RCTs met the inclusion criteria; therefore, this study included nonrandomized prospective cohort studies and case series in the meta-analysis. Stata 15 and RevMan 5.3 were adopted for the PRISMA and meta-analysis. Heterogeneity was quantified by the I2 statistic; the random-effects model was used if heterogeneity was >50%. Otherwise, the fixed-effects model was used. The risk ratio (RR) and its 95% CI were calculated based on the extracted data. P < .05 was considered the threshold for statistical significance. The studies considered to be at high risk of bias were removed from the primary meta-analyses to reduce the compounding of bias. 10
A sensitivity analysis was performed to determine the robustness of our results. To investigate whether a short- or long-term follow-up time introduced bias into our study, eligible studies were evaluated by follow-up times >2 versus ≤2 years. Moreover, we conducted a sensitivity analysis of all studies—including those removed from the meta-analyses—to determine the influence of studies with a high risk of bias in our review.
Results
Literature Search and Selection
A total of 17 studies § with a total of 4059 participants met the study criteria and were included for evaluation. The literature search and selection of studies are presented in Figure 1.
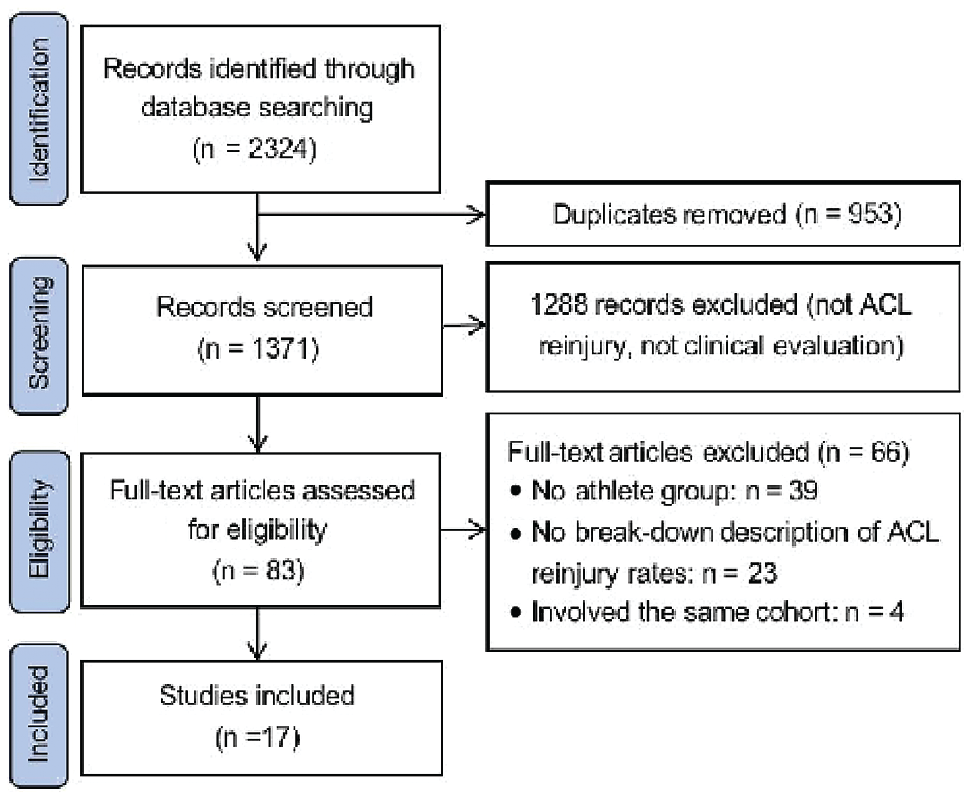
PRISMA flowchart of search results. ACL, anterior cruciate ligament; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
All 17 studies provided a clear population description of athletes and/or their activity level as well as the respective second injury rates of both ipsilateral and contralateral sides. The sample size of the included studies ranged from 39 to 1415, with a follow-up time ranging from 1 to 10 years. Approximately 80.2% of athletes (n = 3257; range, 37.2%-100%) in the included studies chose to RTS of any kind after ACLR. The median age at the time of surgery was 21.6 years. A total of 1087 patients from 5 studies11,14,24,35,62 were classified as adolescent athletes according to activity description. Ten studies ‖ described separate ACL reinjury events in male and female patients. The overall characteristics of the included studies are presented in Table 1.
Characteristics of the Included Studies a

contra/ipsi, contralateral/ipsilateral; RCT, randomized controlled trial; SNKLR, Swedish National Knee Ligament Registry.
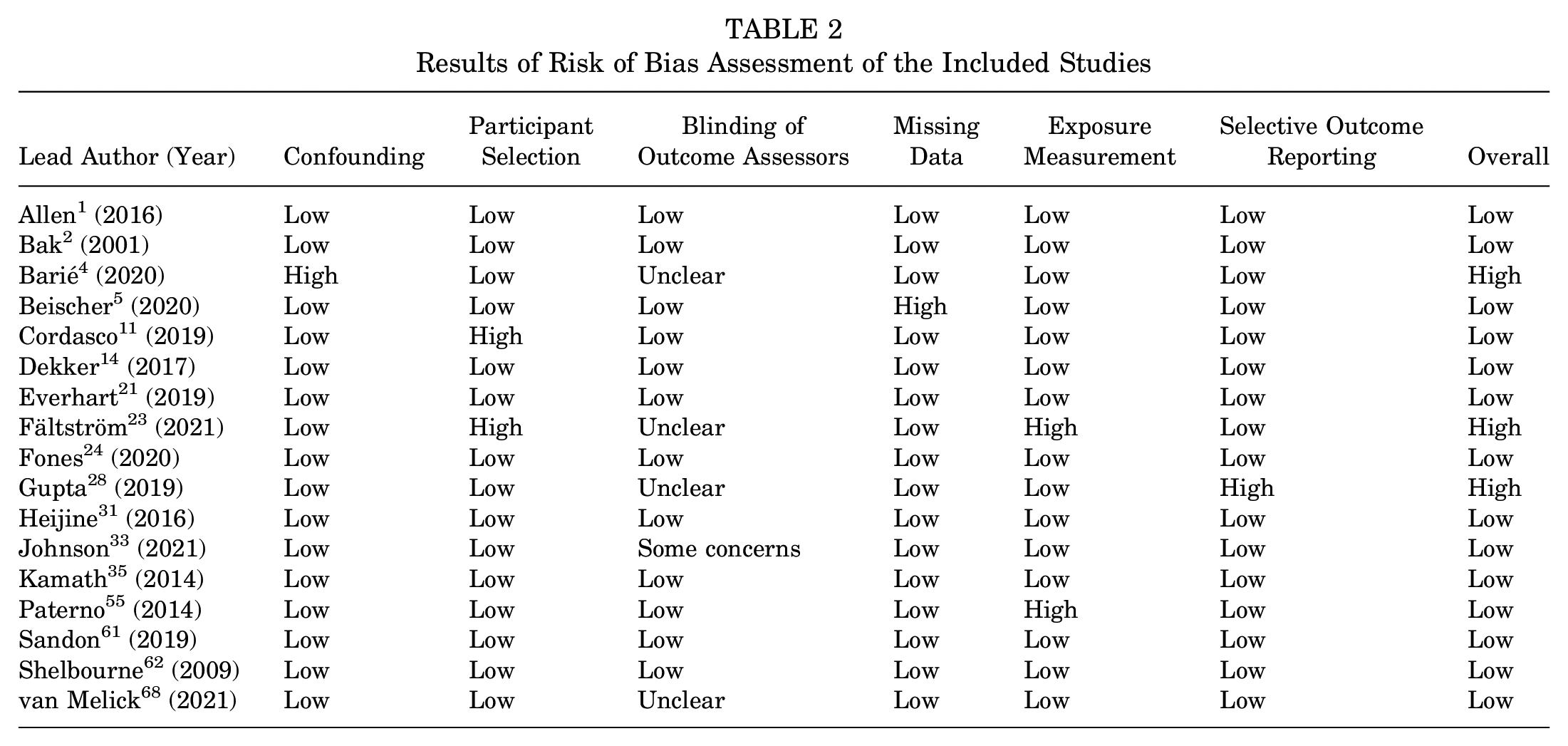
Of the included articles, 3 studies2,23,28 were at high risk of bias (Table 2). Thus, 14 studies ¶ (n = 3424 patients) were included in the meta-analyses.
Results of Risk of Bias Assessment of the Included Studies
Comparison of ACL Reinjury Rate to Either Knee
Overall, the pooled ACL reinjury rate across the 14 studies # was 14.8% (n = 504). The pooled contralateral and ipsilateral reinjury rates were 8.6% (n = 295) and 6.2% (n = 209), respectively. The reinjury rate of the contralateral side was 1.41 times higher than that of the ipsilateral side after ACLR (P < .0001) (Figure 2).
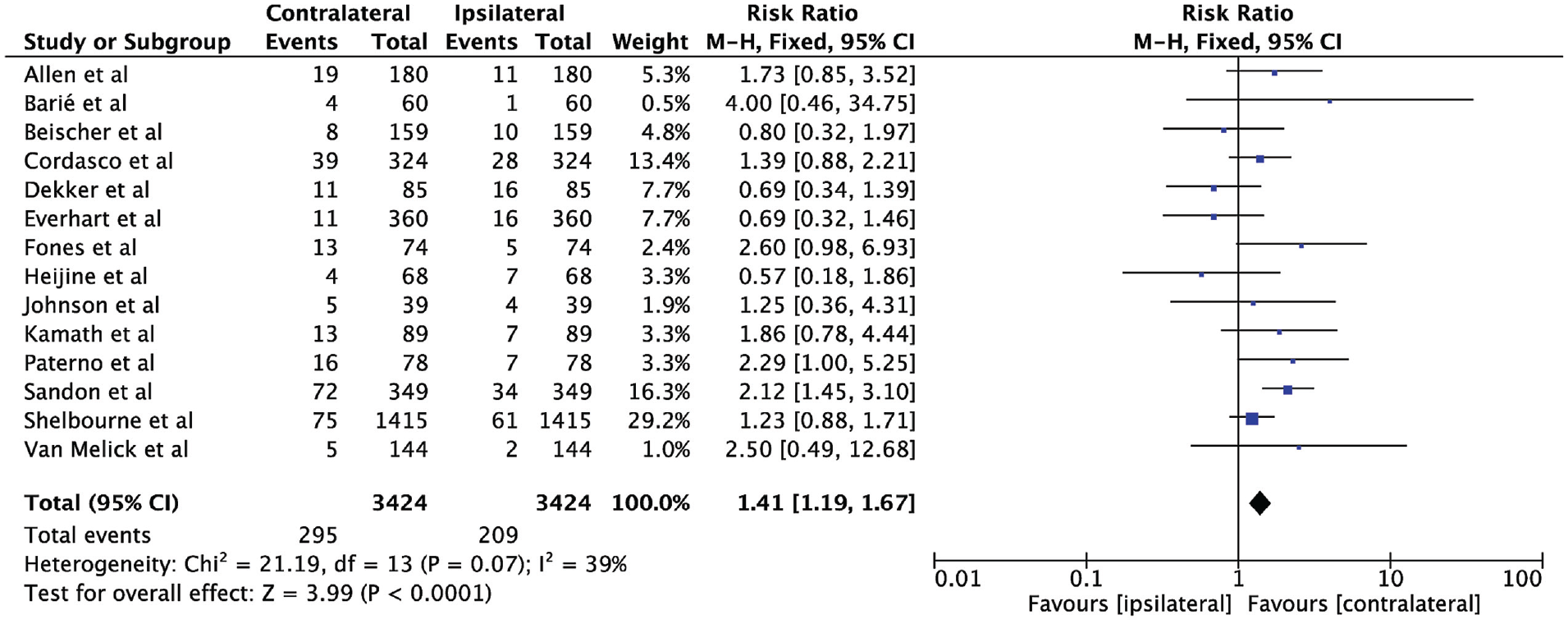
Contralateral versus ipsilateral reinjury rates for athletes from 14 studies. ** M-H, Mantel-Haenszel.
Effect of Younger Age on ACL Reinjury Rate to Either Knee
Figure 3 presents the results of 5 studies11,14,24,35,62 that separately reported ACL reinjury rates in an adolescent athletic cohort (n = 1046). Specifically, we included the precollegiate group reported by Kamath et al 35 in this subanalysis since all composing participants had undergone ACLR before college, although their mean age was not noted. The pooled ACL reinjury rate of this adolescent athletic cohort was 20.7% (n = 217). No statistical difference (RR, 1.15 [95% CI, 0.89-1.48]; P = .28) between the contralateral (n = 116 [11.1%]) and ipsilateral sides (n = 101 [9.6%]) was observed in this group.

Effect of Sex on ACL Reinjury Rate to Either Knee
The results of 8 studies §§ that provided both ipsilateral and contralateral data in different sexes are displayed in Figure 4. Of the male cohorts, ACL reinjury rates of the ipsilateral and contralateral sides were 5.6% (72/1297) and 4.4% (58/1297), respectively. No significant difference between the ipsilateral and contralateral sides (RR, 0.81 [95% CI, 0.58-1.13]; P = .21) was found in male athletes. On the other hand, female athletes had a significantly higher reinjury rate (119/1326 [9%]) on the contralateral side compared with that on the ipsilateral side (72/1326 [5.4%]; RR, 1.65 [95% CI, 1.25-2.19]; P = .0005).

Results of Sensitivity Analyses
Sensitivity analyses were performed comparing studies with long-term (>2 years; 11 studies ‖ ‖ ; n = 3163) versus short-term follow-ups (≤2 years; 3 studies33,55,68; n = 261). A statistically higher incidence of contralateral ACL injury was shown in both subgroups (>2 years: RR, 1.37 [95% CI, 1.15-1.63]; P = .0005 and ≤2 years: RR, 2 [95% CI, 10.06-3.76]; P = .03), indicating that the main results of this review were stable regardless of the follow-up time (Figure 5).

To determine the effect of observed bias on our study results, the 3 studies2,23,28 with a high risk of bias were added back to the analysis. Differences between the reinjury rate to either knee were still statistically significant. However, the pooled results were stable except for the female group, as only a nonsignificant trend of higher contralateral reinjury rate (RR, 1.34 [95% CI, 0.88-2.06]; P = .17) was shown when including the studies with a high risk of bias.
Discussion
In this review, we compared the ACL reinjury rate of the athletic population's contralateral and ipsilateral sides after primary ACLR. Overall, the pooled ACL reinjury rate of the contralateral side was 8.6%, which was 1.41 times higher than that of the ipsilateral side. Moreover, female athletes were at greater risk for contralateral ACL reinjuries, while the same trend was not found in male athletes. Furthermore, the reinjury rates of the 2 sides were statistically comparable in the adolescent athletic cohort.
As athletes are more likely to RTS after ACLR than previously thought,11,20,35 the need for high-level evidence to prevent further injury will increase in this parallel. However, many studies did not stratify a clear statement of athletic exposure or activity level for the included participants,7,30,47,72 especially in single-surgeon cohorts. The heterogeneity of the studied population would cast a shadow on the validity of applying results to athletes in the real world. Moreover, although a paucity of researchers considered athletic exposure as a potential risk factor for ACL reinjuries,59,72,74 few had noted whether contralateral reinjury rates were comparable with or greater than ipsilateral reinjury rates.
The present study found that ACL reinjury was more likely to occur in the contralateral knee in athletes with a history of ACLR. A previous meta-analysis by Wiggins et al 74 reported increased ACL reinjury rates of the contralateral side over the rates of ipsilateral graft rupture regardless of activity level. More recently, data from the Swedish National Knee Ligament Registry 61 demonstrated a 2-fold higher rate of consequent contralateral ACL injuries than that of the operated side in 349 soccer players who had ACLR and returned to play. Factors that might lead to a higher risk of contralateral ACL reinjury in athletes were still inconclusive. First, more mature surgical techniques and secure graft choices make it possible to reduce surgical failure and graft rupture.15,44,73 Moreover, the same exposure to risk factors such as bad exercise habits, and residual hormonal, anatomic, and biomechanical defects that led to the initial ACL injury are still present in the contralateral knee, causing a higher incidence of contralateral ACL rupture.38,51 It was also suggested that a change in the motor patterns may be contributing since it protected the reconstructed knee but simultaneously exerted more pressure on the contralateral limb.16,29,41,49 Further research is needed to examine how the kinematics of the contralateral extremity change from postoperative rehabilitation, from RTS to reinjury and how the postoperative rehabilitation strategy might be modified. In addition, we found an equal rate of reinjuries to either knee among adolescent athletes. Our finding was consistent with most results in the literature. Bickel et al 6 defined the insufficient size of adolescent ACL <7 mm and reported that grafts harvested in the adolescent population always had insufficient size. Therefore, immature hamstring tendon grafts with insufficient size for reconstruction may contribute to a higher risk of graft failure. 6 Thus, further research focused on the relationship between graft choice and reinjury rate in the adolescent population is needed. Furthermore, considering a higher baseline risk of contralateral ACL injuries among general athletes, these findings may be explained by increased risk factors of adolescents with previously operated knees. It was commonly recognized that young age is a very significant risk factor for ACL reinjury after ACLR.34,43 Young athletes had RTS rates ranging14,19,20,36,63 from 91% to 96%, which is considerably higher than those of adults, ranging20,22 from 60% to 75%. Moreover, the correlation between age and second injuries may be powered by higher activity levels of younger patients, 27 who reported to participate more in aggressive sports at every time point. 62 Biomechanical data also support this graft reinjury trend in adolescents regarding the deferred return of quadriceps and hamstring strength and neuromuscular control after ACLR.26,78 Moreover, skeletally immature patients can experience growth disturbance, including tibial recurvatum and distal femoral overgrowth on the ACL-reconstructed knee. 38 High sports demand but mismatching and undeveloped knee function put adolescent athletes at risk for reinjury of grafts, which could lead to an equal risk of reinjury to either knee.
The final aim of our study was to determine the sex-based effects on the difference between the reinjury rates of the contralateral and ipsilateral sides. This study demonstrated that female athletes were more susceptible to reinjury of the contralateral ACL than the previously operated knee, whereas the same trend was not found in male athletes. Therefore, the conclusion that ACL reinjury was more common on the contralateral than on the ipsilateral side may only apply to female athletes. Future studies should focus on the percentage of female athletes in the population to avoid any potential bias in the overall results when comparing reinjury rates. In a recent meta-analysis, Patel et al 52 reported a trend that more reinjuries occur in women's contralateral limbs rather than their ipsilateral limbs, although nonstatistically significant. Recently, several explanations have been suggested to put women at a higher risk of contralateral ACL reinjury. Wiggins et al 74 found that women may be particularly at risk for deficits in the uninvolved limb at the time of injury or develop compensation mechanisms in the rehabilitation, which could be explained by the functional unreadiness of the reconstructed knee. Pollard et al 57 noted that female soccer players had altered lower extremity coupling variability during side-step cutting after returning to play. They were also reported to exhibit increased knee abduction angles, and thus poorer frontal plane kinematics. 65 Moreover, women had smaller ACLs than men and a narrower mean cross-sectional area of the ACL.13,17,64 In the current studies23,62, most patients received a 10 mm-wide patellar tendon graft for ACLR regardless of sex. This means that female athletes are more likely to receive an ACL graft larger and wider than their primary ACL. Thus, high quality grafts tend to have better biomechanical properties, and the poor biomechanical properties of primary ACL may be one of the reasons for the higher contralateral ACL incidence. Our findings suggest that an improved rehabilitation program bridging general physical therapy and RTS should be developed for female athletes. More emphasis should be placed on regaining symmetrical function in this high-risk population to prevent reinjury after ACLR.
Risk of Bias Assessment
We identified 3 studies2,23,28 as having a high risk of bias and excluded them from our meta-analysis. A sensitivity analysis was performed by including all high-risk bias studies to demonstrate their influence on our pooled estimates of the difference between the ipsilateral and contralateral sides. The pooled results were stable except for the female subgroup, as a significantly higher rate of reinjury was no longer demonstrated in the contralateral side when including the studies with a high risk of bias.
Limitations
There are several limitations to this review. Several studies were removed because they lacked details regarding data on both ipsilateral and contralateral reinjuries, especially on sex-based information. This could result in a selection bias of misrepresentation of the reinjury rates. To ensure the homogeneity of the included studies, we conducted a strict inclusion criterion on the athletic population. In contrast, some potentially eligible studies may be excluded because of the absence of a depiction of population characteristics. Another limitation is that since not all studies conducted clinical assessments, there may be a chance for unidentified failures. Varied outcome measures, including surgery, may also underestimate the true incidence of ACL reinjury. We also acknowledge that in our review, graft choice, surgical techniques, and rehabilitation strategies, which could have an impact on the injuries that resulted from ACLR, were not consistent within the studies.
Conclusion
The contralateral ACL was more vulnerable to reinjury than the ipsilateral side in athletes after ACLR. Female athletes were more likely to reinjure their contralateral native ACL, while the same trend was not found in their male counterparts. In addition, the reinjury rate of either knee was comparable in adolescent athletes.
Footnotes
Final revision submitted June 1, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the National Key R&D Program of China (2021YFA1201303), the Clinical Research Plan of SHDC (SHDC2022CRT021), the National Natural Science Foundation of China (82172511, 81972121, 81972129, 82072521, and 82111530200), the Introduction Project of Clinical Medicine Expert Team for Suzhou (SZYJTD201714), the Shanghai Talent Development Funding Scheme (2020080), the Shanghai Sailing Program (21YF1404100, 22YF1405200, and 23YF1404300), the Shanghai Committee of Science and Technology (22DZ2204900 and 23ZR1445700), the Medical Engineering Joint Fund of Fudan University (YG2022-14), and the Science and Technology Innovation Project of General Administration of Sport of China (22KJCX010). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.