
Abstract
Background:
Glenolabral articular disruption (GLAD) lesions may occur in adolescents with anterior shoulder instability, resulting in articular cartilage loss and reduced functional glenoid surface area.
Purpose/Hypothesis:
To compare failure rates and patient-reported outcomes (PROs) between adolescents with versus without GLAD lesions who were treated for anterior shoulder instability with arthroscopic stabilization. It was hypothesized that the comparison would yield no significant differences.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients aged ≤18 years who were treated for anterior shoulder instability with arthroscopic stabilization between 2010 and 2021 were retrospectively identified. Those patients with a GLAD lesion identified at the time of surgery were compared with patients with >2 years of retrospective follow-up who were matched to the no-GLAD cohort according to pathology and management. Demographic and patient characteristics including recurrent instability, complications, and reoperations were recorded. All patients in the GLAD cohort were contacted to obtain PRO data, including the Single Assessment Numeric Evaluation; the shortened version of the Disabilities of the Arm, Shoulder, and Hand questionnaire; and the Pediatric Adolescent Shoulder Survey. Patients were also asked about recurrent instability and additional shoulder problems.
Results:
Of 35 included patients (mean age, 15.4 ± 1.6 years; 80% male), 15 patients (43%) with GLAD lesions and 26 patients without GLAD lesions were identified. Both cohorts had similar patient characteristics, number of anchors, and anchor constructs; the mean follow-up period was significantly different (GLAD vs no-GLAD, 6.9 ± 3.3 vs 3.4 ± 1.2 years, respectively; P < .001). Seven of 15 GLAD patients (46.7%) underwent loose body removal; 4 of 15 GLAD patients (26.6%) and 9 of 26 no-GLAD patients (34.6%) had recurrent subjective instability (P = .7). No significant group differences were found in PRO scores, reoperation rates (15% no-GLAD vs 20% GLAD), or percentage of patients with recurrent instability between cohorts (P > .05).
Conclusion:
Adolescent patients with and without GLAD lesions treated arthroscopically for anterior shoulder instability had similar PROs and failure rates at intermediate duration of follow-up. GLAD lesions may be managed in a similar surgical manner as isolated Bankart tears in teenagers, with expectations of similar outcomes.
Anterior shoulder instability in adolescents has an extremely high risk of recurrence. With a recurrence rate as high as 95% with nonoperative treatment,4,10,13,14 many adolescents and young adults require arthroscopic stabilization. Although most of these patients achieve good postoperative outcomes and high rates of return to sport,1,7 the frequency of recurrent instability remains significant. Therefore, there has been recent interest in understanding and attempting to mitigate this risk. In 2019, Kramer et al 8 reported that 25% of their adolescent cohort experienced recurrent instability after arthroscopic stabilization. In 2021, Cheng et al 2 identified 4 risk factors for recurrent instability after arthroscopy: glenoid bone loss, decreased glenoid retroversion, skeletal immaturity, and >1 presurgical instability event.
Whether additional glenoid pathology influences outcomes to the same degree is unclear. Glenolabral articular disruption (GLAD) lesions, although fairly uncommon, can occur in addition to the more predictable Bankart lesion.11,18 It has been suggested that loss of articular cartilage adjacent the labrum, which characterizes a GLAD lesion, may be associated with inferior outcomes or higher risk of recurrent instability. Pogorzelski et al 12 showed that of the 10 patients in their cohort for whom arthroscopic Bankart repair failed, 30% had GLAD lesions. In contrast, Elrick et al 6 compared a cohort of patients with GLAD lesions to those without such lesions in an adult population and found no significant difference in postoperative patient-reported outcomes (PROs), satisfaction, or rate of recurrent instability. In 2020, Davey et al 3 published a study comparing outcomes after arthroscopic Bankart repair in adult patients with and without GLAD lesions and reported no difference in outcome between the groups.
With few studies in the literature so far, the true clinical impact of a GLAD lesion remains unclear. In addition, none of the aforementioned studies specifically evaluated adolescent patients. Therefore, the purpose of this study was to compare PROs of adolescent patients with and without GLAD lesions who were treated for anterior shoulder instability with arthroscopic stabilization. Considering the findings in adult patients, we hypothesized there would be no significant difference in outcomes between the cohorts.
Methods
Patient Selection
After obtaining approval for the study protocol from our institutional review board, we used Current Procedural Terminology code 29806 to retrospectively identify adolescent patients aged ≤18 years who were treated for anterior shoulder instability with arthroscopic stabilization between 2010 and 2021. We excluded patients with more extensive anterior tears (anterior and posterior, multidirectional, and concurrent superior tears) and isolated posterior labral repairs, identifying patients with isolated Bankart repair and capsulorrhaphy. We further excluded patients with previous ipsilateral shoulder surgery and underlying syndromes affecting the musculoskeletal system. Only those patients with >2 years of follow-up data in their charts were included.
Injuries were confirmed by clinical and radiographic evidence of anterior shoulder instability (history of dislocation or subluxation, positive anterior apprehension test, and anterior labral tear seen on magnetic resonance imaging [MRI]). GLAD lesions were defined as an avulsion of anterior inferior glenohumeral cartilage associated with an anterior inferior labral tear or Bankart tear and were confirmed via arthroscopic imaging at the time of this study (Figure 1).
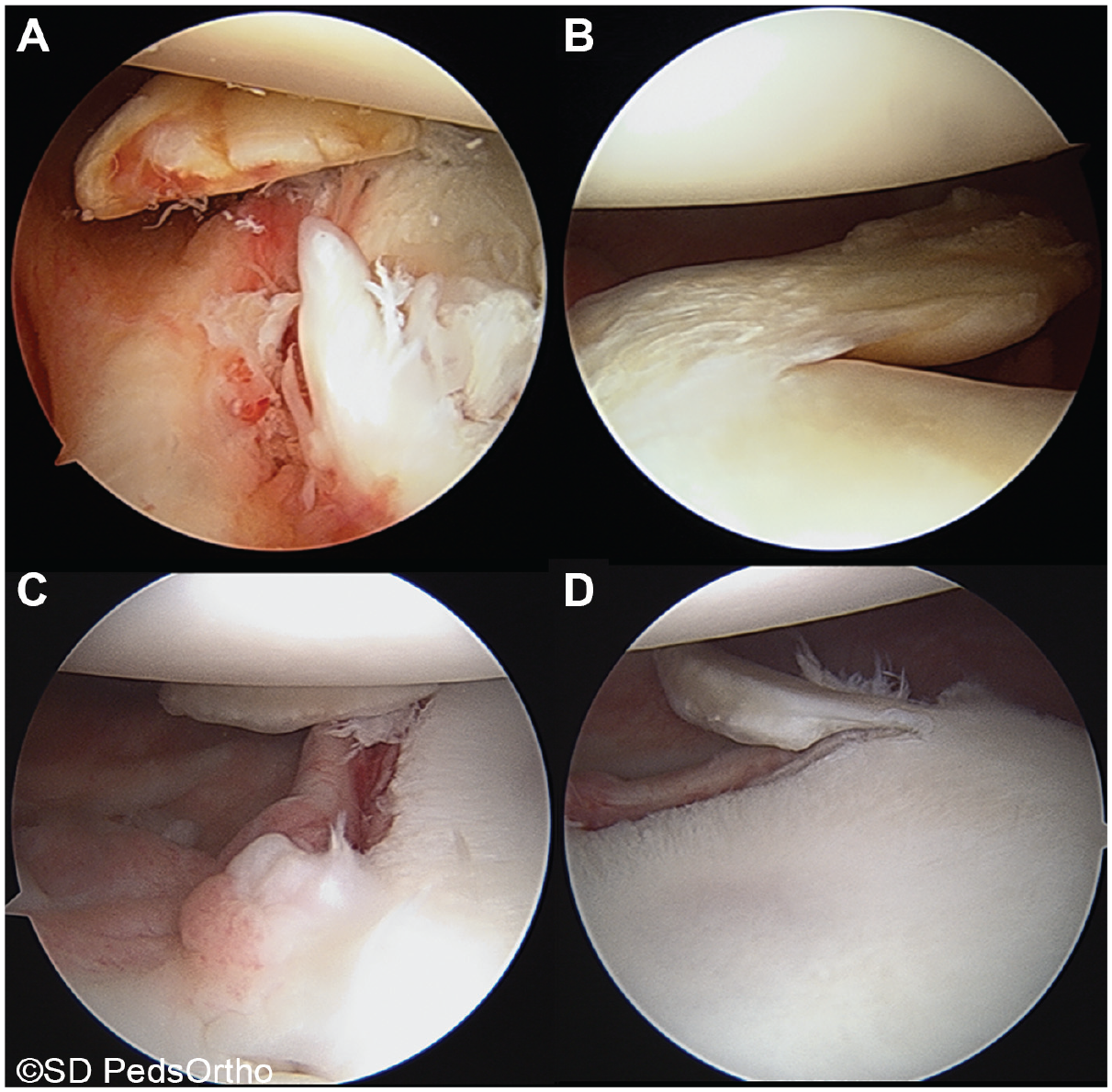
(A and B) Images of a 15-year-old girl with large anteroinferior glenolabral articular disruption (GLAD) lesion before repair. (A) Arthroscopic view from the anterosuperior portal demonstrating the avulsed articular cartilage and surrounding damage. (B) View from the posterior portal demonstrating the avulsed articular cartilage hinged off the articular surface and sitting inferiorly. (C and D) Images of a 17-year-old boy with a small anteroinferior GLAD lesion, (C) viewed from above and (D) viewed from posterior.
After identifying the patients with GLAD lesions (and the different pathologic characteristics), we created the no-GLAD cohort by further application of exclusion criteria to match the GLAD cohort according to number of anchors used and location of tear.
Surgical Technique
Indications for surgery were based on a discussion between the patient and treating surgeon; specific indications included pain, apprehension, functional limitation after an episode of anterior shoulder instability (including dislocation requiring formal reduction, dislocation reportedly self-reduced, or self-reported subluxation) despite nonoperative treatment, an unacceptably high risk of recurrent instability based on patient characteristics and activity level, or MRI evidence of the GLAD lesion after a first-time dislocation. All procedures were performed by 2 fellowship-trained surgeons (A.T.P. and E.W.E.).
All patients underwent shoulder arthroscopy in the lateral decubitus position under general anesthesia. A standard posterior, anterosuperior, and anterior (adjacent to the subscapularis tendon) portal was used for diagnostic arthroscopy and working portals, but a percutaneous anteroinferior transscapularis insertion was used for implants. The labrum was mobilized, and the anterior glenoid rim was prepared using a rasp and a shaver. The capsulolabral tissues were attached to the glenoid rim with suture anchors (Arthrex Biocomposite Suturetak, Arthrex Fibertak, or Smith & Nephew Bioraptor). In the no-GLAD cohort, repairs were performed to the edge of the glenoid, but in the GLAD cohort, repairs were performed to the margin of the articular cartilage loss, on the face of the glenoid (Figure 2). Unstable cartilage fragments were always removed, and the juxtaposed labrum and/or articular surface was debrided to maximize the stability of the labral repair. Any additional pathology such as posterior labral tearing or loose bodies were addressed at the time of surgery.
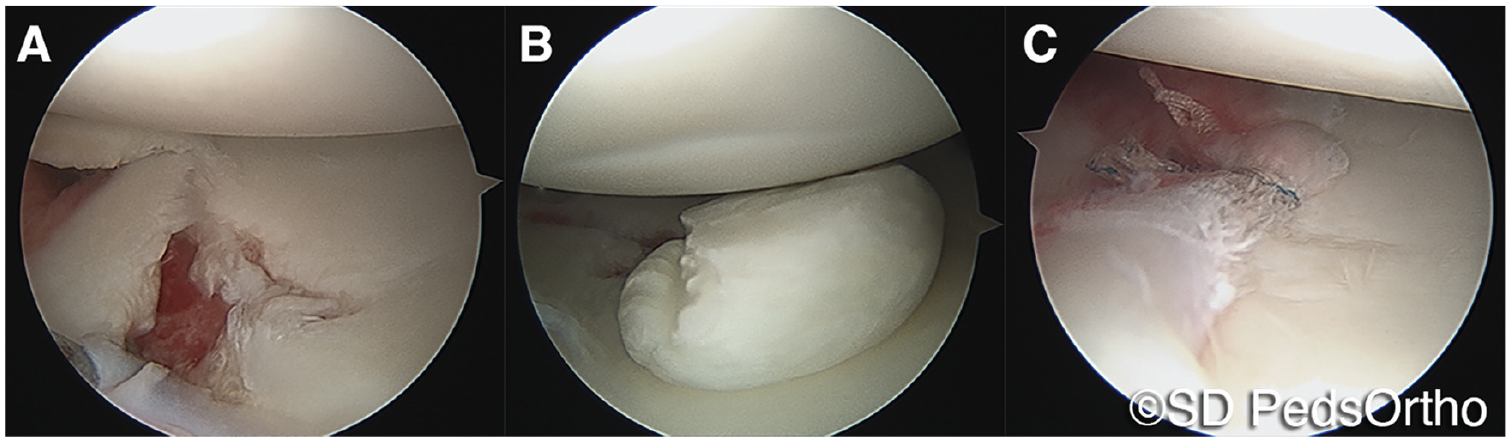
An arthroscopic images of a 16-year-old girl with a large glenolabral articular disruption lesion. (A) Anterosuperior viewing portal demonstrating a grade 4 chondral defect. (B) Posterior view of the same patient demonstrating the size of the cartilage fragment, with injury to the humeral head. (C) Image after en face repair of the labrum to repair the cartilage defect.
Postoperatively, patients were immobilized in a shoulder immobilizer full-time for 2 weeks and then transitioned to a sling (wherein the immobilizer strap around the waist is removed) with part-time wear for an additional 4 weeks. Active and active-assisted range of motion exercises began 2 weeks postoperatively with formal physical therapy, with advancement to strength training after 6 to 8 weeks postoperatively, based on physical therapy protocols. Patients were allowed to return to contact sports after 6 months but only after graduation from physical therapy with range of motion and strength restored to at least 90% of the contralateral shoulder.
Patient-Reported Outcomes
Medical records were reviewed for patient, injury, and surgical characteristics, including age, sex, injury mechanism, number and type of anchors used for repair, and any additional operative procedures. All patients in the GLAD cohort were contacted to obtain PRO scores for the Single Assessment Numeric Evaluation (SANE), 17 the shortened version of the Disabilities of the Arm, Shoulder and Hand questionnaire (QuickDASH), 9 and the Pediatric Adolescent Shoulder Survey. 5 These patients were also asked whether they had experienced recurrent instability (subjective subluxation or dislocation) or had undergone any additional procedures for their shoulder. The PRO data for patients in the no-GLAD cohort were obtained from the medical records, as patients in this group were not contacted, per the study design.
MRI scans were evaluated for all included patients to measure pertinent morphologic features, particularly the size of the GLAD lesion. Glenoid bone loss was measured using the best-fit circle method. 16 However, rather than measuring the space of missing bone within the circle, we measured the total width of the glenoid, and the width of the missing cartilage at the anteroinferior glenoid was then measured in that same horizontal plane. The measurements were made at the largest dimension of the articular surface (and therefore the greatest dimension of articular injury). This injury width was then divided by the total width to determine the size of the cartilage injury. Hill-Sachs lesions were also assessed and measured.
Statistical Analysis
Descriptive statistics were calculated for all variables of interest. The GLAD and no-GLAD groups were compared using the nonparametric Mann-Whitney U test for continuous or interval-dependent variables and the Fisher exact test or chi-square test for categorical variables. Alpha was set at P < .05 to declare significance, and SPSS Version 28 (IBM) was used for analyses.
Results
A total of 35 patients with GLAD lesions were treated arthroscopically for anterior shoulder stabilization during the study period. In this cohort, 18 patients (51.4%) also underwent loose body removal at the time of surgery. The mechanism of initial injury was football in 15 patients (42.9%) and a different contact sport (wrestling, hockey, soccer, water polo, volleyball) in 8 patients (22.9%); 13 patients (37.1%) had surgery after 1 reported episode of instability. The GLAD lesion was identified on preoperative MRI scans in 16 patients (45.7%). Of the 35 patients, 15 (43%) could be contacted for PROs and were included in the final comparison. The mean age for this refined cohort was 15.4 ± 2 years, and 80% were male.
To identify the no-GLAD cohort, we reviewed 685 patient charts to yield a cohort of 129 patients with a minimum 2-year outcome data. After we applied further criteria (such as age, anchor number, location of tear), the no-GLAD cohort consisted of 26 patients. Both cohorts had similar baseline characteristics (Table 1). The GLAD cohort had significantly longer follow-up (6.9 ± 3 years) than the no-GLAD cohort (3.4 ± 1 years; P < .001).
Comparison of Baseline Characteristics Between Study Cohorts a

Data are reported as mean ± SD or n (%). Boldface P value indicates statistically significant difference between groups (P < .05). GLAD, glenolabral articular disruption.
The MRI assessment of lesion size demonstrated that the mean size of the GLAD lesions was 4.8 ± 1.5 mm (range, 2.7-8.8 mm) in the largest dimension. They accounted for a mean 17.7% ± 5% (range, 7.6%-26.3%) of the total glenoid articular surface but with no substantial loss of bone noted either by MRI or via arthroscopy. No off-track Hill-Sachs lesions were noted in the GLAD cohort.
No significant difference was found in any of the PRO measures at minimum 2-year follow-up (Table 2). No differences in pain scores, Pediatric Adolescent Shoulder Survey scores, or QuickDASH scores could be discerned between the 2 cohorts.
Comparison of Patient-Reported Outcome Scores Between Study Cohorts a

Data are reported as mean ± SD. GLAD, glenolabral articular disruption; QuickDASH, shortened version of the Disabilities of the Arm, Shoulder and Hand questionnaire; SANE, Single Assessment Numeric Evaluation.
No significant group difference in reoperations was noted at a mean of 20 months after the index procedure (20% in the GLAD cohort compared with 15.4% in the no-GLAD cohort; P = .7). Further, no difference was found in the percentage of patients who experienced recurrent instability (26.7% vs 34.6%, respectively; P = .6) (Table 3). Regarding revisions, 3 patients in the GLAD group underwent revision surgery. One patient experienced a reinjury 1 year postoperatively while playing football and was treated with revision shoulder arthroscopy with Bankart repair, followed by a second reinjury 3 years postoperatively treated with shoulder arthroscopy with posterior labral repair. Another patient experienced shoulder reinjury during shotput 1 year postoperatively and underwent revision shoulder arthroscopy with Bankart repair. The third patient sustained a new posterior labral tear playing water polo and was also found to have posterior arthrofibrosis from the previous surgery; the patient underwent shoulder arthroscopy for lysis of adhesions and posterior labral repair. In the no-GLAD group, 7 patients experienced recurrent instability requiring revision shoulder arthroscopy with revision Bankart repair.
Reoperations and Recurrent Instability a

Data are reported as n (%). GLAD, glenolabral articular disruption.
Discussion
Adolescents undergoing shoulder arthroscopy for anterior instability with concomitant GLAD lesions appear to achieve similar PROs to those teenagers undergoing anterior Bankart repairs without a GLAD lesion at intermediate duration of assessment. Moreover, the reoperation and recurrent instability rates were not significantly different between the 2 cohorts, suggesting that presence of a GLAD lesion may not be a risk factor for inferior outcomes or recurrent instability after arthroscopic shoulder stabilization. Both cohorts experienced reoperation and recurrent instability rates that are higher than ideal.
The high failure rate (defined as recurrent instability) in both cohorts of adolescent patients in our study (~27% and ~35% for the GLAD and no-GLAD groups, respectively) is a reflection of the previously published literature in this age group. Kramer et al 8 found recurrent instability after arthroscopic stabilization in 25% of their adolescent cohort at a mean of just under 3 years of follow-up. Their study reported on 36 adolescents with a mean age of 16 years, similar to our study, which reports on a total of 41 patients with a mean age of 15 years in the GLAD cohort and 16 years in the no-GLAD cohort. An older study that evaluated both arthroscopic and open stabilization surgeries in this same age group (mean age, 16-17 years) found survivorship curves related to recurrent instability of 86% at 2 years and only 49% at 5 years (or the equivalent of 24% failure and 51% failure, respectively). 15 Therefore, the comparison in outcomes in the current study and previous studies on GLAD lesions needs to be viewed within this lens—that adolescents have a higher failure rate than do adults.
In 2018, Pogorzelski et al 12 raised concerns that the articular cartilage damage associated with GLAD lesions may predispose patients to inferior outcomes. It is well established that glenoid pathology affects postoperative outcomes for patients with shoulder instability. Cheng et al 2 showed that in adolescents, increased glenoid bone loss and decreased glenoid retroversion are risk factors for recurrent instability after arthroscopic stabilization. However, how a GLAD lesion affects the geometry of the glenoid and whether it affects shoulder stability are not well understood. It has been proposed that a GLAD lesion may affect the glenoid version (leading to more anteversion) or that it may indicate a higher energy injury to the capsulolabral complex. 12 Additionally, loss of glenoid cartilage surface area associated with GLAD lesions may predispose patients to further instability. Given articular cartilage involvement, there is theoretical concern that GLAD lesions could contribute to the development of osteoarthritis (although this has not yet been explored in the literature). These hypotheses have certainly sparked clinical interest. However, recent research investigating whether outcomes are inferior in patients with GLAD lesions is predominantly in the adult literature.
In a case series of anterior shoulder instability, Pogorzelski et al 12 showed that the presence of a GLAD lesion was associated with a higher risk of failure (defined as revision surgery or redislocation). However, this has not been shown in subsequent comparative studies in the adult population or our current study of adolescent patients. Davey et al 3 published a retrospective cohort study in 2020 evaluating outcomes after anterior shoulder stabilization in patients with and without GLAD lesions. Their GLAD lesion group was also small (22 patients). The study used different PROs (Rowe score, Shoulder Instability–Return to Sport after Injury), and the patients were older (mean age, 26 years), but Davey et al found no significant difference in outcomes between the groups. Additionally, their revision rates of 13.6% in the GLAD group and 4.5% in the no-GLAD group were not statistically different, although their findings of lower revision rates and recurrent instability are consistent with lower failure rates in the adult patient with anterior instability. Elrick et al 6 also found no difference in outcomes or satisfaction in their comparative study of adult patients (mean age, 29 years) with and without GLAD lesions (27 patients per group). Our study of a purely adolescent cohort had findings similar to those of Davey et al and Elrick et al, but our intermediate-term outcomes still reflect the higher failure rates of this surgery in this active age-group.
Combining the findings of the current study with others presently available in the literature, it appears that patients with GLAD lesions, including adolescents, can expect similar outcomes after arthroscopic stabilization. However, it is also important to examine ways in which these patients might be unique. Within our cohort of patients with GLAD lesions, only 47% of lesions were recognized on preoperative MRI scans. This emphasizes that surgeons need to be able to recognize the lesions intraoperatively and be prepared to adjust stabilization constructs as needed, even if they were not expecting a GLAD lesion based on imaging. Additionally, nearly half (46%) of the patients with GLAD lesions also had loose body removal at the time of surgery. This illustrates the importance of carefully looking for loose bodies once a GLAD lesion is recognized during arthroscopy.
One of the important factors to consider regarding this injury pattern is that the GLAD lesion is not the same as the loss of anterior osseous glenoid; rather, the GLAD lesion entails the loss of articular cartilage. To that end, even though our cohort had relatively high glenoid loss (17% by MRI measurement and as high as a quarter of the glenoid surface in 1 patient), this was not loss of the underlying bone stock. Therefore, the GLAD lesion does not seem to contribute to further worsening of the failure rate (which is already high in this young population).
Limitations
This study had several limitations, including a small sample size and a high rate of loss to follow-up (only 15/35 patients in the GLAD lesion group could be reached to obtain outcomes). The cohort sizes were not large enough for propensity matching, and therefore, the length of follow-up differed between the groups. However, given that the duration of outcome assessment was longer in the GLAD cohort, it can be presumed that the failure rate of these patients would not exceed that of the no-GLAD cohort if the latter group were followed for an equally long duration of time. Additionally, although outcomes were collected prospectively, this study was otherwise a retrospective examination of the patients’ clinical and surgical history. The GLAD cohort patients were contacted at the time of the study, whereas the no-GLAD cohort was made up of patients who already had >2 years of clinical follow-up available. A post hoc power analysis was performed to detect a 10% difference in failure (based on the Davey et al 3 study, which demonstrated no difference in outcomes for adult patients, with about 9% revision surgery difference between the GLAD and no-GLAD cohorts). Our study would need 692 adolescent patients (346 in each cohort) to detect a difference with 80% power at an alpha of <.05. This suggests that the lack of significance between our 2 cohorts is not a spurious finding due to small sample size but rather a result of the small effect size of the difference observed. Finally, the size of the GLAD lesion was not routinely reported in these patients’ operative notes, and therefore, we were not able to determine whether lesion size affects outcomes.
Conclusion
Adolescent patients with and without GLAD lesions treated arthroscopically for anterior shoulder instability had similar PROs and failure rates at intermediate duration of follow-up. GLAD lesions may be managed in a similar surgical manner as isolated Bankart tears in teenagers, with expectations of similar outcomes. The continued high failure rate in this youthful population suggests that improvement in management is needed and should be sought.
Footnotes
Final revision submitted June 20, 2023; accepted June 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.T.P. has received education payments from ImpactOrtho and SportsTek Medical and consulting fees from OrthoPediatrics. E.W.E. has received nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of California, San Diego (170519X).