
Abstract
Background:
This study sought to evaluate the effect of atelocollagen insertion into the bone–tendon interface of the repaired tendon after arthroscopic rotator cuff repair for high-grade partial articular supraspinatus tendon avulsion (PASTA) lesions.
Purpose:
To compare clinical and radiological outcomes of atelocollagen-inserted rotator cuff repair and atelocollagen-noninserted rotator cuff repair in the high-grade PASTA lesions.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The data from 301 consecutive patients who underwent arthroscopic rotator cuff repair of PASTA lesions between January 2017 and June 2020 were retrospectively reviewed. Patients with minimum 2-year follow-up data were included and divided into 2 groups: those treated with transtendon suture-bridge repair without additional augmentation (group 1) and those with atelocollagen-inserted transtendon suture-bridge repair (group 2). Patients in group 2 were matched 1:1 to patients in group 1 using propensity score matching (n = 68 per group); and pain visual analog scale, American Shoulder and Elbow Surgeons, University of California, Los Angeles, Korean Shoulder Scoring System, Simple Shoulder Test, and range of motion scores were compared between these groups. Also, repaired tendon integrity and thickness were compared immediately, 6 months, and 1 year after surgery on magnetic resonance imaging (MRI) using the vertical distance from the midpoint footprint of the greater tuberosity.
Results:
In most comparisons, there were no significant differences in outcome measures and range of motion between groups. However, less residual discomfort at the final follow-up was also documented in group 2 (P = .043). Also, the difference in forward flexion was 3.7° at 1 year and 5.4° at final follow-up, and the difference in abduction was 2.2° at final follow-up, which were all significantly greater in the experimental group. Group 2 showed significant greater tendon thickness of the repaired tendon immediately, 6 months, and 1 year after surgery on MRI (P≤ .001).
Conclusion:
Addition of atelocollagen did not improve outcome scores. However, there was slightly greater flexion and abduction at final follow-up. Also, there was less residual discomfort at final follow-up.
Partial-thickness rotator cuff tears (PTRCTs) are a common cause of shoulder pain and limitation of daily activities. Articular-side PTRCT occurs approximately 2 to 3 times more often than bursal-side PTRCT. Partial articular supraspinatus tendon avulsion (PASTA) lesions are a type of articular-side PTRCT and are a common pathology in the aging population. Partial tears of <50% of the rotator cuff thickness are usually treated nonoperatively. 16 Conversely, when the tear is ≥50%, surgical intervention focusing on repair has been successful. 27 PTRCTs have been considered a point on the rotator cuff disease continuum that includes overuse of an essentially normal tendon, tendinitis, tendon fibrosis, partial-thickness tendon tears, and complete tendon tears. 8 Although the natural history of PASTA lesions remains unclear, this variety of tendon disruption is generally associated with pain and disability, and it has been shown that 53% of PASTA lesions tend to grow over time.16,34
Because not all PASTA lesions are symptomatic, their exact diagnosis can be difficult, and diagnosis of PASTA lesions often relies on magnetic resonance imaging (MRI). 4 However, discrepancies between the clinical examination and the details of MRI scans are sometimes present. Although the lesions may be similar, the degree of inflammation may vary, clinical differences in pain or range of motion (ROM) may occur. Sometimes, PASTA lesions combined with stiffness cause severe shoulder pain. Initially, many conservative treatments, including trigger-point dry needling or acupuncture needling, physical therapy, and medication are used.23,32 However, when these treatment modalities fail, arthroscopic repair of PASTA lesions could be performed. Arthroscopic transtendon repair of PASTA lesions has shown good clinical outcomes.9,19,26,28 Compared with the normal tendon thickness, high-grade PASTA lesions showed high-grade articular-side tears (Ellman grade 3) compatible with a thin rotator cuff thickness. Also, even though a repair was performed, residual shoulder discomfort often persisted. 1 High-grade PASTA lesions with chronic shoulder pain are interesting considering the tendency of tendon thickness to affect surgical selection: take down and rotator cuff repair versus transtendon repair. These PASTA lesions often showed a poor tendon quality with insufficient or thin tendons. For these reasons, an attempt was made to insert atelocollagen between the repaired tendon and greater tuberosity bone after transtendon suture bridge repair in PASTA lesions in this study.
Collagen is a key structural protein found in the extracellular matrices of many connective tissues in mammals, making up about 30% of the whole-body protein content. The substance of a human rotator cuff tendon is composed of a tenocyte and an extracellular matrix composed of type 1 collagen. 5 Among them, collagen functions to transfer force and disperse energy transferred to the tendon, and it supports the connective tissue. 25 Atelocollagen is a highly purified collagen treated with proteolytic enzymes (pepsin) to remove the terminal telopeptides, minimizing the immune response, 7 resulting in low immunogenicity. 20 This has many advantages in terms of biocompatibility and optimizing the collagen-cell interaction to enhance efficacy and reduce side effects.20,24 A variety of studies have considered various human tissue treatments, such as cartilage regeneration,17,18,30 tendon regeneration,13-15 head and neck soft tissue reconstruction,3,10,11 and periodontal management.22,33 Particularly in the clinical application to the shoulder, gel- or patch-type atelocollagen became available in Korea after Korean Food & Drug Administration approval in 2015. Since 2019, our institute has been performing ultrasonography-guided atelocollagen injection in outpatient clinics or arthroscopic injection to the repaired rotator cuff for PTRCT. This atelocollagen (Coltrix TendoRegen; Ubiosis) is a commercial product; it is contained in a sterilized syringe and can be used immediately for surgery.
The purpose of this study was to evaluate the effect of collagen scaffolds as an augment to arthroscopic rotator cuff repair for high-grade PASTA lesions. Clinical outcomes and radiologic outcomes, including tendon integrity and thickness, were compared. The study hypothesis was that atelocollagen augmentation into the bone-tendon interface after arthroscopic rotator cuff repair would increase repaired tendon thickness and improve clinical scores and residual discomfort.
Methods
Study Patients
This study was designed as a nonconcurrent, matched, cohort study. The study protocol received institutional review board approval, and the requirement for participant informed consent was waived owing to the retrospective nature of the study. The data of 301 consecutive patients who underwent arthroscopic rotator cuff repair of high-grade PASTA lesions between January 2017 and June 2020 as performed by a single surgeon (J.-H.J.) were retrospectively reviewed. High-grade PASTA lesions were confirmed by MRI and arthroscopic evaluation. Through arthroscopic examination, the tear size of the PASTA lesions, focusing on the anteroposterior length and width of torn supraspinatus tendon was evaluated. All patients showed Ellman grade 3 articular-side partial-thickness tears (ie, high-grade PASTA lesions). Lesions >6 mm in depth were defined as Ellman grade 3 (>50% thickness). 6
The indication for arthroscopic rotator cuff repair was high-grade PASTA lesions diagnosed by MRI. High-grade PASTA lesions that did not respond to nonoperative treatment for >6 months were targeted for surgical treatment. The initial patients in this study underwent arthroscopic rotator cuff repair alone. When atelocollagen became available in 2019 in our institute, it was used to augment the arthroscopic rotator cuff repair in subsequent patients. Patients with ≥2 years of follow-up were included, while those who met any of the following conditions were excluded: (1) combined full-thickness subscapularis tendon tear, (2) glenohumeral osteoarthritis, (3) superior labrum anterior to posterior (SLAP) repair, (4) follow-up loss, and (5) previous shoulder surgery.
An a priori power analysis was performed to determine the appropriate sample size, which was estimated by utilizing an effect size of 0.5, an acceptable alpha error of .05, and a beta error of 0.2 to ensure a power of 80%. Calculations indicated that it would be necessary to include ≥64 patients to compare means between the groups using the independent-samples Student t test.
The 301 patients were classified into the following 2 groups based on atelocollagen insertion in patients who underwent arthroscopic rotator cuff repair of high-grade PASTA lesions: group 1 (226 patients treated with arthroscopic repair without atelocollagen augmentation) and group 2 (75 patients treated with arthroscopic repair with atelocollagen augmentation).26,28 The group 2 patients were then matched to group 1 patients in a 1:1 format using propensity score matching, with sex, age, body mass index, trauma history, and tear size (anteroposterior and lateral) as matching characteristics (68 patients per group) (Figures 1 and 2).

Classification of patients into study groups. AP, anteroposterior; BMI, body mass index; OA, osteoarthritis; PASTA, partial articular supraspinatus tendon avulsion; SLAP, superior labrum anterior to posterior; SSC, subscapularis.

Evaluation of patient data using propensity score matching. AP, anteroposterior; BMI, body mass index.
Surgical Technique
After administration of general anesthesia combined with an interscalene block, the patient was positioned in the lateral decubitus position. An arthroscope was inserted through the posterior portal, and the complete glenohumeral joint examination was performed. The biceps tendon pathology or labral pathologies were evaluated completely. Soft tissue tenodesis was performed in cases with biceps tendon partial tears, and cases with SLAP lesions were excluded. Subacromial decompression was routinely performed and distal clavicular excision was not performed. Almost all PASTA lesions were located on the anterior aspect of the supraspinatus tendon. Arthroscopic findings confirmed Ellman grade 3 PASTA tear.
The tear was debrided, and repair was performed in situ with a 4.5-mm double-loaded suture anchor (Healicoil PK; Smith & Nephew) using the suture-bridge technique. For the prevention of tendon damage through the anchor insertion during conventional transtendon repair, the preference was to conduct anchor insertion through the anterosuperior portal just above the biceps tendon. Once rotator cuff repair was complete, CO2 gas was inflated into the subacromial space using the CO2 infusion pump after stopping saline insertion. Finally, a spinal needle was inserted into the bone-tendon interface of the repaired tendon (arrow in Figure 3F) and then 1 mL porcine type 1 atelocollagen gel at a concentration of 3 mg/mL was injected through the in situ spinal needle into the bone-tendon interface.

Arthroscopic findings of the atelocollagen insertion. (A) In the glenohumeral joint, high-grade partial articular supraspinatus tendon avulsion lesion (arrow) extended posteriorly. (B) Four strands of the inserted anchor were passed through torn rotator cuff tendon margin (transtendon repair). (C) In the subacromial space, transtendon suture bridge repair (arrow) was done. Partial fraying of bursal-side rotator cuff was present. (D) Complete restoration of articular-side tear (arrow) was shown in the glenohumeral joint. (E) Once rotator cuff repair was complete, we inflated CO2 gas into the subacromial space through the CO2 infusion pump. (F) Atelocollagen was injected through the in situ spinal needle into the bone-tendon interface of the repaired tendon (arrow).
Postoperatively, an ultra-sling orthosis (shoulder abduction brace; Seoul-Brace) was applied for 6 weeks with an abduction pillow for rehabilitation. On the second postoperative day, pendulum and passive ROM exercises were initiated. Active-assisted ROM and muscle-strengthening exercises were allowed 6 weeks after surgery. Daily activities and light exercise were permitted 12 weeks postoperatively.
Clinical and Imaging Outcomes
Clinical assessment findings included the visual analog scale (VAS) for pain, shoulder index of the American Shoulder and Elbow Surgeons (ASES) shoulder score; the University of California, Los Angeles; the Korean Shoulder Scoring System, and the Simple Shoulder Test. At the final follow-up, residual discomfort was also evaluated. 1 Shoulder ROM was measured by a single blinded examiner (H.Y.) in the neutral position using a goniometer in both groups preoperatively and at every follow-up visit. Postoperatively, tendon integrity (Sugaya classification) and repaired tendon thickness were measured in both groups and compared immediately, 6 months, and 1 year after surgery, respectively. Two examiners (H.Y. and S.O.) independently evaluated the MRI; both were blinded to the procedure and not involved in the surgery. Through T2-weighted fat-suppression MRI via oblique coronal MRI, changes in the tendon thickness were assessed. The tendon thickness as the vertical distance from midpoint footprint around the greater tuberosity was measured. The measuring point of tendon thickness was located 1.2 cm behind the bicipital groove.
Statistical Analysis
The Kolmogorov-Smirnov test was used to confirm a normal distribution for all data. Data related to ROM and functional scores were compared between the study groups with the independent-samples Student t test. Separately, the Pearson chi-square test was used to compare differences in categorical demographic variables between the groups.
Reproducibility was assessed based on the intraclass correlation coefficient. Intraobserver reliability was assessed using the values measured by each examiner at 1-week intervals, and interrater reliability was measured by comparing the means of the 2 observers. Reliability measurements were reviewed, and the results indicated substantial to almost perfect agreement (intraclass correlation coefficients ranging from 0.62 to 0.97). Statistical analysis was performed using SPSS 25 software (SPSS Inc), and the alpha level was set at .05.
Results
Patient Characteristics
Group 1 contained 29 men and 39 women, while group 2 was composed of 27 men and 41 women. The mean age at the time of surgery was 61.9 years in group 1 and 61.4 years in group 2, and there were no significant differences in the operated arm, body mass index, trauma history, tear size of PASTA lesions, and biceps tendon tear between them (Table 1).
Patient Characteristics a

Data are shown as mean ± SD or No. of patients. Boldface P value indicates statistically significant difference between groups (P < .05). AP, anteroposterior; SSP, supraspinatus muscle.
Functional and Radiological Outcomes
At minimum 2-year follow-up, the mean VAS pain and outcome scores had improved over time in both groups, with no significant difference between the groups at any time point (P < .05 for all) (Figure 4). Even though there was no difference in VAS pain scores between the 2 groups at the final follow-up, there was a significant difference in residual discomfort between the groups (P = .043) (Table 2 and Figure 4).

Functional scores (visual analog scale [VAS] for pain; American Shoulder and Elbow Surgeons [ASES]; the University of California, Los Angeles [UCLA], rating scale; Korean Shoulder Scoring System [KSS]; and Simple Shoulder Test [SST] score) improved after surgery in both groups, with no significant group differences at any time point.
Clinical and Radiological Outcomes a
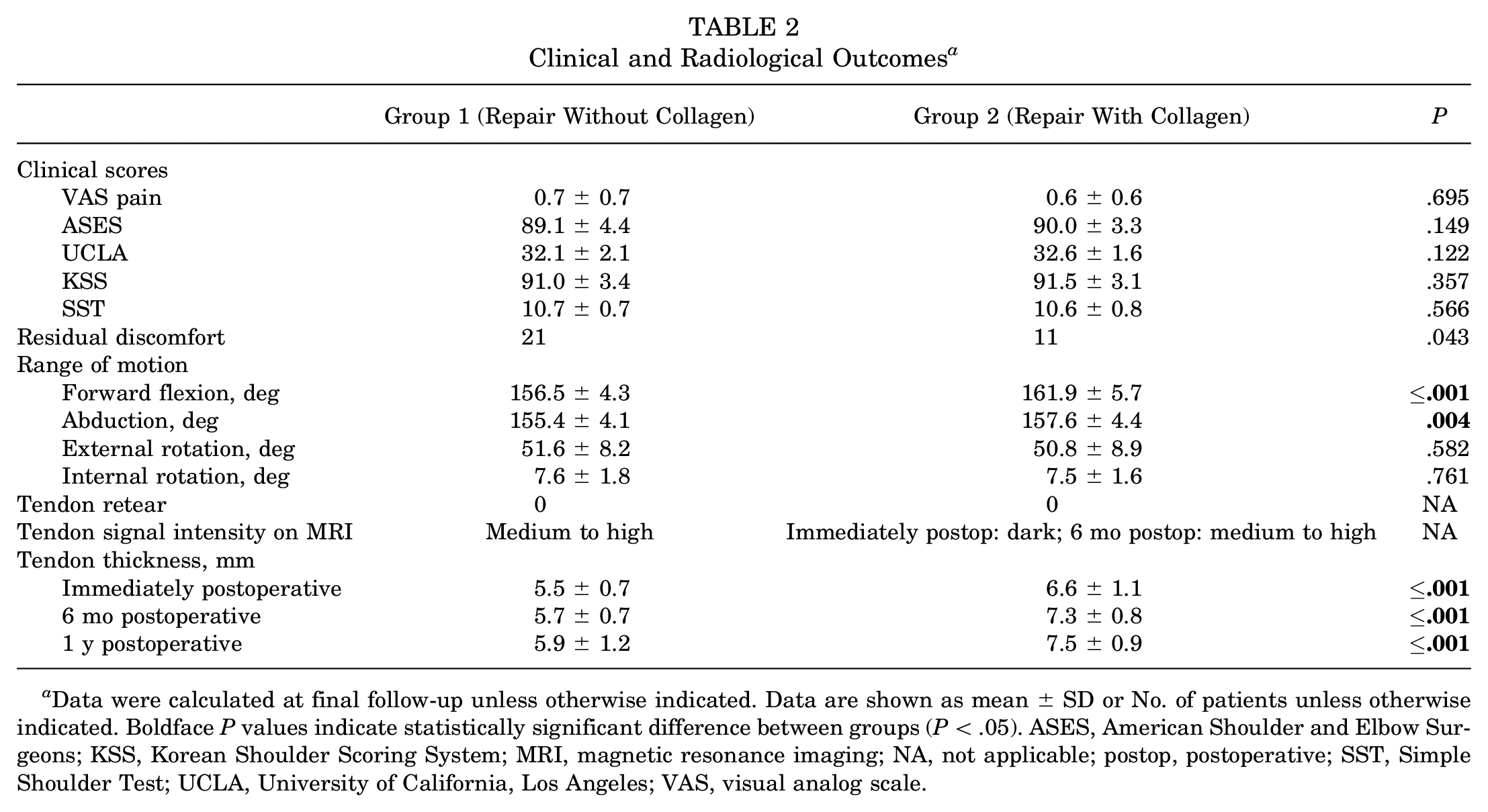
Data were calculated at final follow-up unless otherwise indicated. Data are shown as mean ± SD or No. of patients unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; KSS, Korean Shoulder Scoring System; MRI, magnetic resonance imaging; NA, not applicable; postop, postoperative; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Patients in both groups showed improvement in ROM over time. Forward flexion at 1 year (mean difference, 3.7°; P = .001) and final follow-up (mean difference, 5.4°; P≤ .001) and abduction at final follow-up (mean difference, 2.2°; P = .004) were slightly but statistically significantly greater in group 2 versus group 1, but no statistically significant differences in external rotation and internal rotation were found (Table 2 and Figure 5).
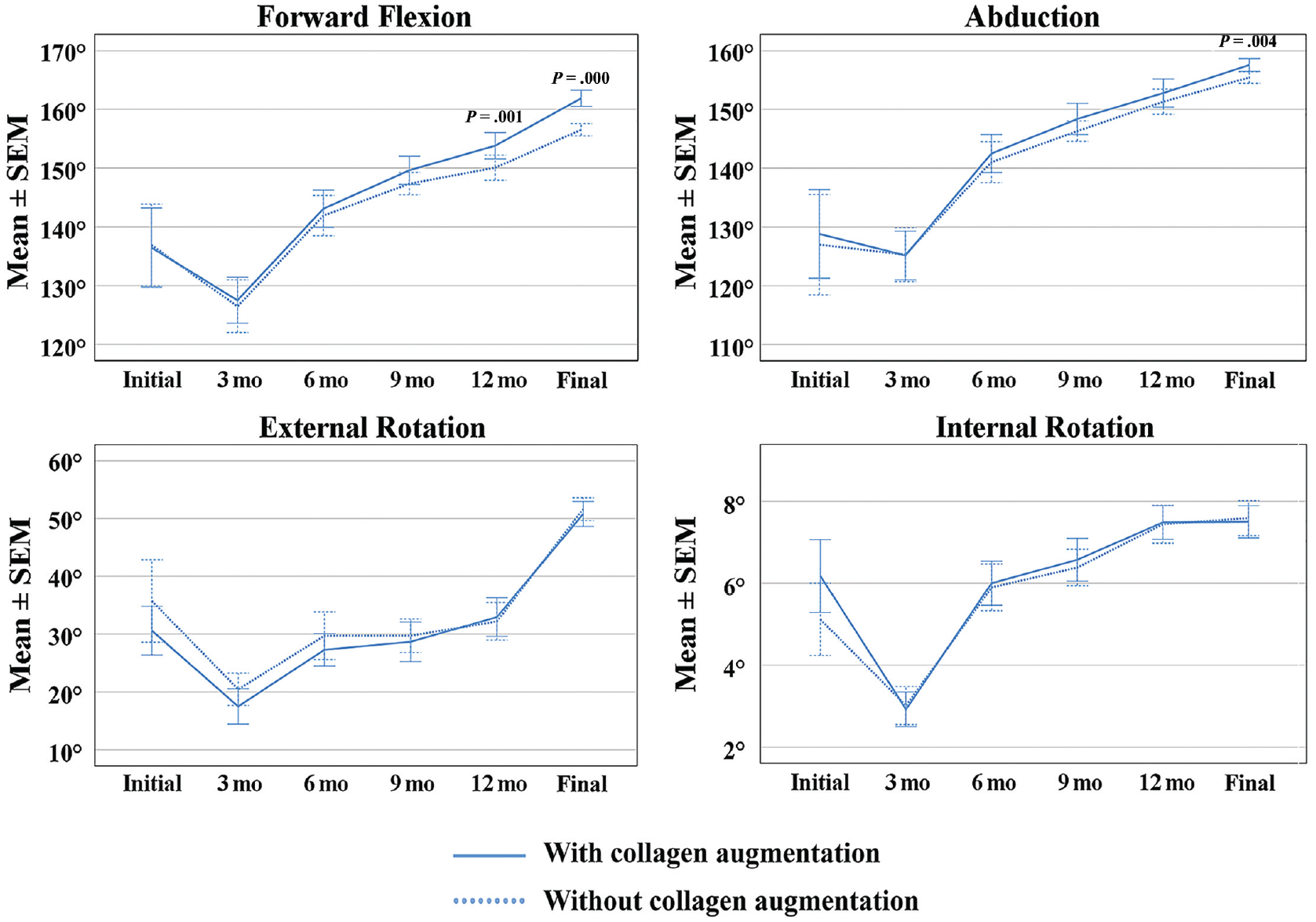
Passive range of motion (ROM) was improved in all measures of ROM at the final follow-up. There were no significant differences between the groups regardless of time except forward flexion at 12-month and final follow-up and abduction at final follow-up.
Postoperative follow-up MRI was performed at both 6 months and 1 year after surgery. Neither group showed retear at follow-up, and there was no significant difference in the tendon integrity or retear rate. However, the thickness of the repaired tendon was significantly greater in group 2 compared with group 1 on the immediately postoperative (6.6 mm vs 5.5 mm), 6-month follow-up (7.3 mm vs 5.7 mm) and 1-year follow-up (7.5 mm vs 5.9 mm) MRI (P≤ .001 for all) (Table 2 and Figure 6).

A 55-year-old woman with a high-grade partial articular supraspinatus tendon avulsion lesion experienced an increased tendon thickness on 12-month follow-up magnetic resonance imaging (MRI) after injection of 1 mL of atelocollagen (T2-weighted fat suppression oblique coronal image). (A) Preoperative MRI. The measuring point of tendon thickness (arrow) was located 1.2 cm behind the bicipital groove. The double-sided arrow indicates the tendon thickness at the tear site. (B) Immediate postoperative MRI after rotator cuff repair with atelocollagen injection. Compared with preoperative MRI, tendon thickness (arrow) was increased and dark signal intensity was found in the repaired tendon substance. The double-sided arrow indicates the tendon thickness. (C) On the 6-month follow-up MRI, the dark signal intensity had disappeared in the repaired tendon substance. (D) Increased tendon thickness with improved tendon signal intensity continued at the 1-year follow-up MRI. The arrows in (C) and (D) indicate the previous tendon tear sites.
Discussion
The main finding of our study was that, in contrast to our hypothesis, there were no significant differences in outcome scores or retear rates between the study groups. However, we found that atelocollagen-inserted rotator cuff repair resulted in greater tendon thickness and less residual discomfort in PASTA lesions. Also, forward flexion at 1-year follow-up and final follow-up and abduction at final follow-up were slightly but significantly greater in the patients with atelocollagen augmentation.
In the clinical application of atelocollagen to the shoulder, 2 types of atelocollagen may be used: gel type and patch type. Patch-type atelocollagen is used for augmentation after full-thickness rotator cuff repair, while gel-type atelocollagen is administered more commonly in outpatient clinics. Gel-type atelocollagen is also used for ultrasonography-guided injection for partial rotator cuff tears or arthroscopic injection to the repaired rotator cuff tendon. For gel-type atelocollagen delivery, the injection is performed directly to the tear site using ultrasound in the outpatient clinics2,15 or intraoperatively after rotator cuff repair.12,14
Table 3 summarizes the findings of 2 level 1 randomized controlled trials that reported on clinical applications of atelocollagen.12,15 Using gel-type atelocollagen injection, Jeong et al 12 observed an additional effect after coinjection of atelocollagen and hyaluronic acid. These authors found that coadministration of atelocollagen and hyaluronic acid did not differ significantly in terms of the clinical findings; however, it led to decreased retear rates (P < .05) and improved rotator cuff healing and increased the integrity of the rotator cuff repair site. Kim et al 15 reported that atelocollagen injection was able to improve functional outcomes and tendon integrity in intratendinous rotator cuff tears.
Summary of 2 Level 1 Randomized Controlled Trials of Atelocollagen a

ASES, American Shoulder and Elbow Surgeons; CSS, Constant Shoulder Score; HA, hyaluronic acid; MRI, magnetic resonance imaging; VAS, visual analog scale.
Patch-type atelocollagen is used to treat rotator cuff tears with poor tendon quality. A prospective study of 23 patients using a bioinductive collagen patch for large and massive rotator cuff tears showed good clinical outcomes (mean ASES score, 82.87) at 2 years of follow-up. 31 Bioinductive atelocollagen patch augmentation after complete rotator cuff repair led to a 96% healing rate in 23 patients with large to massive rotator cuff tears. An increased tendon thickness was documented at 3, 12, and 24 months after surgery (6.29, 7.72, and 7.28 mm, respectively).
With their experimental setup, Martinello et al 21 reported that the presence of a collagen gel improved penetration of injected adipose-derived mesenchymal stem cells and showed successful recellularization of human tendon using atelocollagen scaffold. Separately, Suh et al 29 conducted a biomechanical and histological study that revealed better healing of the rotator cuff tendon in a rabbit model. The results of these studies are positive and offer encouraging results regarding the effect of atelocollagen.
There are studies that have analyzed radiological results after ultrasound-guided injection with follow-up ultrasound or MRI.2,15 In a study by Chae et al, 2 rotator cuff integrity was measured via an ultrasound performed 2 months after surgery, while muscle volume, fatty infiltration, and retear were measured at 6 months after surgery using MRI. Clear differences in tendon integrity from preinjection to postinjection were not found. Kim et al 15 reported that ultrasound-guided atelocollagen injections have the best effect in intratendinous rotator cuff tears (Table 3), suggesting that better clinical results can be obtained if injections are performed by selecting the patient population appropriately. It is believed that atelocollagen can be an effective tool to reduce chronic shoulder pain in patients with PTRCTs.
Although the retear rate, which is considered the most important finding on MRI, decreased according to Jeong et al 12 and Kim et al, 15 other studies found no significant statistical differences in the healing rate or regeneration.2,14 Most studies reported improved clinical outcomes, especially in the VAS pain score.2,12-15 In the present study, intraoperative addition of atelocollagen did not improve outcome scores. However, there was slighter greater ROM. Also, there was less residual discomfort at final follow-up.
In the outpatient clinics, immediate postinjection pain is a relatively common complication, affecting up to 50% of patients. Severe pain (VAS score, 7-8) may continue for 2 to 7 days after injection.2,15 The causes of the severe pain might be the volume effect, normal inflammatory reaction, or immunologic reactions. Because of high pressure during atelocollagen injection and atelocollagen leakage through the tear site, it is not easy to inject atelocollagen in the exact tear site, especially the site of intratendinous tears, even when using ultrasound. In contrast, intraoperative injection of atelocollagen between the bone and repaired tendon during PASTA repair is easy to complete. During surgery, 2 methods were used to improve atelocollagen insertion in the PASTA lesion. The first was CO2 gas inflation using a CO2 gas infusion pump; after rotator cuff repair, water was removed in the subacromial space, and a CO2 infusion pump was connected to inflate the subacromial space. Without water, the gel-type atelocollagen is well contained between the bone and repaired tendon after PASTA repair without any leakage. The second method was to use white-colored atelocollagen. During the procedure, the leakage of white-colored atelocollagen could be easily observed and the injection speed and location could be adjusted while appropriately observing the leakage. As a result, it was possible to observe an increase in tendon thickness due to the reinforced collagen, and flexion and abduction were slightly improved, which is clinically noteworthy.
Strengths and Limitations
An assessment of the thickness of the repaired tendon after rotator cuff repair is important for predicting the long-term progress of patients diagnosed with high-grade PASTA lesions. Moreover, to the best of our knowledge, no study has reported on the differences in clinical and radiologic outcomes between atelocollagen-augmented or atelocollagen–nonaugmented rotator cuff repair in high-grade PASTA lesions. This is the first study to investigate the effect of atelocollagen application, especially considering repaired tendon thickness and residual discomfort after rotator cuff repair, in high-grade PASTA lesions. Even though histological improvement of poor tendon quality could not be confirmed, postoperative follow-up MRI revealed significant improvements in tendon thickness. Another important finding in this study was the level of residual discomfort after atelocollagen injection during rotator cuff repair in patients with PASTA lesions. Castagna et al 1 previously described residual shoulder symptoms after transtendon repair of high-grade PTRCTs. In the current study, residual discomfort was significantly improved at the final follow-up. This seems to be due to the effect of collagen as a scaffold that increases and promotes the proliferation of new tendon-like tissues and is thought to be the cause of increased ROM and reduced residual discomfort.
The present study has several limitations. First, this study was a retrospective comparative study. A major limitation was that a prospective randomized controlled comparison study to assess atelocollagen augmentation in high-grade PASTA lesions was not performed. Second, a difference in outcomes can arise from treating several concomitant lesions, such as subscapularis partial tears or biceps partial tears. However, the procedure performed, such as debridement, was simple and can be considered to have only a minimal effect on clinical outcomes. Third was a degree of selection bias. Randomized controlled studies with longer follow-up periods are needed. The final limitation was doubt as to whether minimal improvement in ROM and modest increase in tendon thickness could justify the cost and time efficiency of using atelocollagen. In this situation, with uncertain results, there were ethical limits to conducting retrospective or prospective studies.
Conclusion
Addition of atelocollagen did not improve outcome scores. However, there was slightly greater flexion and abduction at final follow-up. Also, there was less residual discomfort at final follow-up.
Footnotes
Final revision submitted June 3, 2023; accepted June 7, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Daejeon St Mary's Hospital (reference No. XA FA-02-2).