
Abstract
Background:
Previous biomechanical studies of the meniscotibial ligament have determined that it contributes to meniscal stability. An injury to it can cause the meniscus to extrude, and reconstruction of that ligament significantly reduces extrusion.
Purpose:
To assess the biomechanical effects of sectioning the lateral meniscotibial ligament (LMTL) and the meniscofibular ligament (MFL) with respect to the radial mobility of the lateral meniscus and to evaluate the biomechanical effects of the capsulodesis and centralization techniques.
Study Design:
Controlled laboratory study.
Methods:
The lateral meniscus of 22 porcine knees was evaluated. They were mounted on a testing apparatus to apply muscle and ground-reaction forces. The meniscus was evaluated at 30° and 60° of knee flexion using 2 markers placed on the posterior cruciate ligament and the lateral meniscus after applying an axial compression of 200 N to the knee joint. Measurements were recorded under 5 conditions: intact lateral meniscus, injury of the LMTL, subsequent injury of the MFL, the use of the open capsulodesis technique, and the reconstruction of the LMTL and the MFL with the centralization technique.
Results:
The distance between the 2 markers was significantly greater in the extrusion group (combined lesion of the LMTL and MFL) than in the intact or reconstruction groups (capsulodesis and centralization techniques; P < .001 in all cases). In the cases of load application, no significant differences were observed between the control group (intact meniscus) and the groups on which the reconstruction techniques were performed. There were also no differences when comparing the results obtained between both reconstruction techniques. In all settings, the distance between the 2 markers increased with the increase in the knee flexion angle.
Conclusion:
In a porcine model, the LMTL and the MFL participated as restrictors of the radial mobility of the lateral meniscus during loading. Their injury caused a significant increase in lateral meniscal extrusion, and the centralization and the capsulodesis procedures were able to reduce extrusion.
Clinical Relevance:
This study demonstrates the capacity of the LMTL and the MFL to restrict the radial mobility of the lateral meniscus during loading and how it is affected when they are injured.
Keywords
Meniscal extrusion is characterized by the meniscus extending and drifting away from the tibial margin of the knee joint. The meniscus displaces from its native position between the tibiofemoral joint and extends into the gutter,26,29 thereby losing some of its mechanical function. It induces dysfunction of load distribution caused by the disruption of the meniscus hoop function. 12 Previous studies have hypothesized that the recently described meniscocapsular attachments of the lateral meniscus, the so-called menisco-tibio-popliteus-fibular complex, and its main component, the lateral meniscotibial ligament (LMTL), act as restrictors of the radial mobility of the lateral meniscus.17,27
Meniscal extrusion is associated with various pathologies (eg, early knee osteoarthrosis, meniscus posterior root tears, radial tears) after anterior cruciate ligament reconstruction 28 and after meniscectomy for symptomatic discoid lateral meniscus.3,14,23 It is frequently accompanied by rapid progression of the degenerative process of the knee as well as by substantial morbidity and pain. 14 Restoring the lost function caused by meniscal extrusion can delay osteoarthrosis progression 25 and/or lead to improvement of articular cartilage after a meniscal allograft transplantation. 13 After meniscal extrusion, the tibial cartilage receives all the load with the knee in extension. 10
Previous biomechanical studies on the medial meniscotibial ligament have determined that it contributes to meniscal stability. 4 An injury to it can cause the meniscus to extrude and the repair of that ligament significantly reduces extrusion.4,6,26 There are no similar studies involving the lateral meniscocapsular junctions, especially the important structures that are part of the lateral knee complex, which are the LMTL, the meniscofibular ligament (MFL), the popliteofibular ligament (PFL), and the popliteomeniscal ligament (PML). 17
The capsulodesis technique was described by Monllau et al 19 in 2017 as a quick and inexpensive solution to reduce meniscal extrusion after lateral meniscal allograft transplantation, with satisfactory results after 2 and 7 years of follow-up.15,16,20 The arthroscopic centralization technique consists of suturing the capsule attached to the meniscus to the edge of the tibial plateau using suture anchors. A decrease in lateral extrusion rates in the clinical follow-up at 2 years has been seen through the evaluation with functional scales and magnetic resonance imaging. 9
The purpose of this study was to determine the normal function and establish an injury and reconstruction model of the LMTL and the MFL in porcine knees in a biomechanical model with simulated weightbearing and knee flexion. We hypothesized that the injury to these ligaments would increase meniscal extrusion. We also hypothesized that the capsulodesis and centralization techniques would restore their biomechanical function to a preinjury state.
Methods
A total of 22 fresh-frozen left hind legs from 6-month-old commercial pork pigs weighing approximately 100 to 120 kg were used in the present investigation. The specimens used for the experiments were purchased within 24 hours of slaughter and were stored temporarily at 9°C (the sacrifice of the animals was for commercial purposes and was not related to the performance of this study). There was no evidence of previous injury and the joint capsules were perfectly sealed. The current study was approved by the Research Ethics Committee, Research Committee and Institutional Committee for the Care and Use of Laboratory Animals of our institution, following the current official Mexican standard (NOM-062-ZOO-1999).
Before testing, all the knees were evaluated with anteroposterior and lateral radiographs to rule out bone abnormalities, previous surgeries, or evidence of previous fractures. Before testing, a lateral parapatellar arthrotomy was performed on each specimen to check for any intra-articular defect, including lateral meniscal damage. No significant macroscopic osteoarthritic changes of the tibial plateau and femoral condyles were found.
Surgical Techniques
The knees were divided equally into 2 groups (n = 11 per group). In the first group, a modification of the capsulodesis technique described by Monllau et al 19 was realized. In the second group, an LMTL reconstruction was performed following the method described by Condron et al, 4 with modifications for working in the knee lateral compartment and adding a reconstruction of the MFL with the help of a third anchor.
A board-certified knee surgeon with experience in the field of orthopaedic sports medicine (R.M.-A.) performed all surgical steps. The knees were resected 15 cm from the joint line proximally and distally and stripped of skin and fat tissue. The deep fascia and medial and lateral retinacula were preserved in each specimen. As a first step, the 2 ligaments of interest were intentionally sought in each pig knee, following the classical anatomic description in humans,17,21,22 and were found in 100% of the specimens with an anatomy very similar to that of humans.
Capsulodesis Technique
Modifications of the capsulodesis technique here consisted of performing it openly. Through a minimal anteromedial and anterolateral capsulotomy (approximately 3 cm due to the great thickness of porcine tissues) and under direct vision, 2 tibial tunnels of 2.4-mm diameter were made. The tunnels were drilled from the anteromedial aspect of the tibia using a low-profile meniscus root tibial guide (Arthrex) with a distance of 0.5 cm between them (Figure 1). Then, two 18-gauge spinal needles loaded with a No. 2 PDS (polydioxanone) suture (ETHICON) were used to pierce the peripheral rim of the meniscus and the capsule with an outside-in technique. This shuttle suture was substituted by a high-strength suture (No. 2 Orthocord; DePuy Synthes) and retrieved through each tibial tunnel. They were then tied to each other on the anteromedial tibial cortex, bringing the capsule together with the tibial plateau (Figure 1). After this, the joint capsule was closed using No. 3 Vicryl suture (Ethicon).

Representative diagram of the capsulodesis technique showing the transtibial tunnels (dashed lines) from the anteromedial cortex of the tibia (red ovals) to the joint capsule attached to the lateral tibial plateau.
Centralization Technique
First, a complete circumferential tear at the midbody of the lateral meniscus was performed, equidistant from the posterior and anterior horns, at the level of the tibial insertion of the LMTL. The technique of cutting the MFL consisted of making a circumferential cut of the ligament at the level of its fibular insertion under direct vision using a No. 22 blade scalpel. A complete tear was chosen in both cases to ensure that only the repair construct was tested. For this study, other stabilizing structures such as the PFL, the superior and inferior PMLs, and the meniscofemoral ligaments were not used.
Briefly, the LMTL reconstruction consisted of placing 2 high-strength sutures (No. 2 Orthocord) in a horizontal mattress formation through the LMTL and the border between the meniscus, and the remaining capsule was attached to the meniscus using an inside-out technique (Figure 2). One suture was placed at the transition point of the anterior horn and mid-body while the other was placed at the transition point of the posterior horn and midbody. The last suture was placed through the MFL using an inside-out technique. After retrieval from the posterolateral capsule incision, these sutures were threaded through two 3.0-mm anchors (Gryphon; Depuy Synthes), which were inserted into the lateral cortex of the proximal tibia under suitable tension for the LMTL (Figure 2). The first anchor was inserted 1 cm anterior to the popliteal hiatus, the second was inserted 1.0 to 1.5 cm anterior to the first anchor, and the third was inserted in the vertex of the fibula for the MFL. Macroscopically, it resulted in an extruded meniscus that was reduced to its original position. The incisions were closed, and specimens were ready for final testing and measurements.

Representative scheme of the centralization procedure using 3 anchors (circles), which moved the inner margin of the meniscus to the original position of the intact meniscus (red lines). Posterolateral view.
Testing Procedure
The femur and tibia were fixed by means of fiberglass resin (resin pp250; Poliformas Plasticas) and polyvinyl chloride piping (10-cm length and 10-cm diameter) in a custom-made universal tester. One 4.5-mm cortical screw was placed through the polyvinyl chloride tubing, fiberglass resin and shaft of each long bone to provide further stability to withstand loads during testing procedures. All muscle groups, the 2 cruciate ligaments, the lateral and medial collateral ligaments, and the knee extensor apparatus were preserved.
A custom-made testing apparatus capable of loading muscle groups and delivering ground-reaction forces independently during a simulated squatting maneuver and under a direct axial compression load was constructed (Figure 3). This device was based on a model previously published by McCulloch et al, 18 with the difference that the one used in this study allowed for angulation of 10° in the coronal plane, maintaining the other axes of mobility (flexion and extension from 0° to 150°, internal and external tibial rotation of 10°, and mediolateral translation of 1 cm in the axial plane). When mounted, the tibial axis was perpendicular to the floor and was attached to a loading head that allowed rotational freedom and the femur was attached to a loading head that permitted translational and varus-valgus movement. Isolated muscle leads from the hamstrings and quadriceps were attached individually using suture tape and were reinforced with multiple mediolateral rip-stop passes of No. 2 sutures (Orthocord) to pneumatic actuators, with a tibial pneumatic actuator delivering a ground-reaction force.

Custom-made testing apparatus. Medial view of a porcine right knee showing the preparation of the muscle groups.
Before testing, the specimen tissue was preconditioned. To that end, 100 full flexion-extension cycles were performed to minimize hysteresis. Starting from a base load of 1 N, a repetitive load with a magnitude of 10 N was then applied 100 times (frequency, 1 Hz). A ground-reaction force of 200 N was applied to the distal tibia,5,8 and scaled loads of 50 N and 20 N were applied to the quadriceps and hamstrings, respectively, at 30° and 60° of flexion (each angle of flexion was confirmed using a goniometer and defined as the angle formed between the anatomic axes of the femur and the tibia at their lateral aspects). The porcine knee cannot extend to 0°, beginning its range of motion at 30° of flexion. The change in marker translation was then averaged and compared for each specimen state at each flexion angle.
Measurement of Meniscal Extrusion
The classic measurement method of meniscal extrusion is performed by measuring the distance from the lateral edge of the tibial plateau to the free edge of the meniscus; however, for this morphometric study in a cadaveric animal specimen, we used the method presented in a previous study. 24
The measurement of meniscal extrusion was performed in accordance with the method described by Ozeki et al, 24 in which spherical plastic color markers (long pins that pierced to the soft tissue 2 cm deep and 4 mm in diameter) were attached to the center of the tibial attachment of the posterior cruciate ligament and the lateral edge of the lateral meniscus in the posterior view (Figure 4). The placement of the spherical markers was agreed among 2 experienced surgeons and 1 anatomist (J.R.P.-M., A.G.T.-G., and H.A.H.-P.), who did not participate in the subsequent measurements. To carry out the measurements, a digital vernier with a precision of 0.01 mm was used (IP67; Skysummr). The markers were put in place before the cut for the meniscal extrusion model (during the preconditioning phase, trial pins were placed in the same locations to ensure that their position did not change during manipulation). Before and after application of the loading forces, the distance between the marker on the posterior cruciate ligament and the marker of the meniscus was measured to evaluate the extrusion. The measurement was made from the medial edge of the lateral marker to the lateral edge of the medial marker. A comparison was not made between the preload and postload conditions in the 2 ligament injury groups as it was considered that the meniscus was extruded before applying the load.

Distance between the marker attached to the PCL attachment, A, and lateral side of the lateral meniscus, B, measured as the medial-lateral extrusion. PCL, posterior cruciate ligament.
The measurement of the medial-lateral extrusion was carried out in 6 different conditions: intact lateral meniscus (control group) without the application of the loading force (n = 22), control group after applying the 200-N loading force (n = 22), isolated injury of the LMTL (after applying the loading force; n = 22) (Figure 5A), the subsequent injury of the MFL (after applying the loading force; n = 22) (Figure 5B), reconstruction of the LMTL with the open capsulodesis technique (before and after applying the loading force; n = 11) (Figure 5C), and reconstruction of the LMTL and the MFL with the centralization technique (before and after applying the loading force; n = 11) (Figure 5D). Measurements were made at both 30° and 60° of flexion.
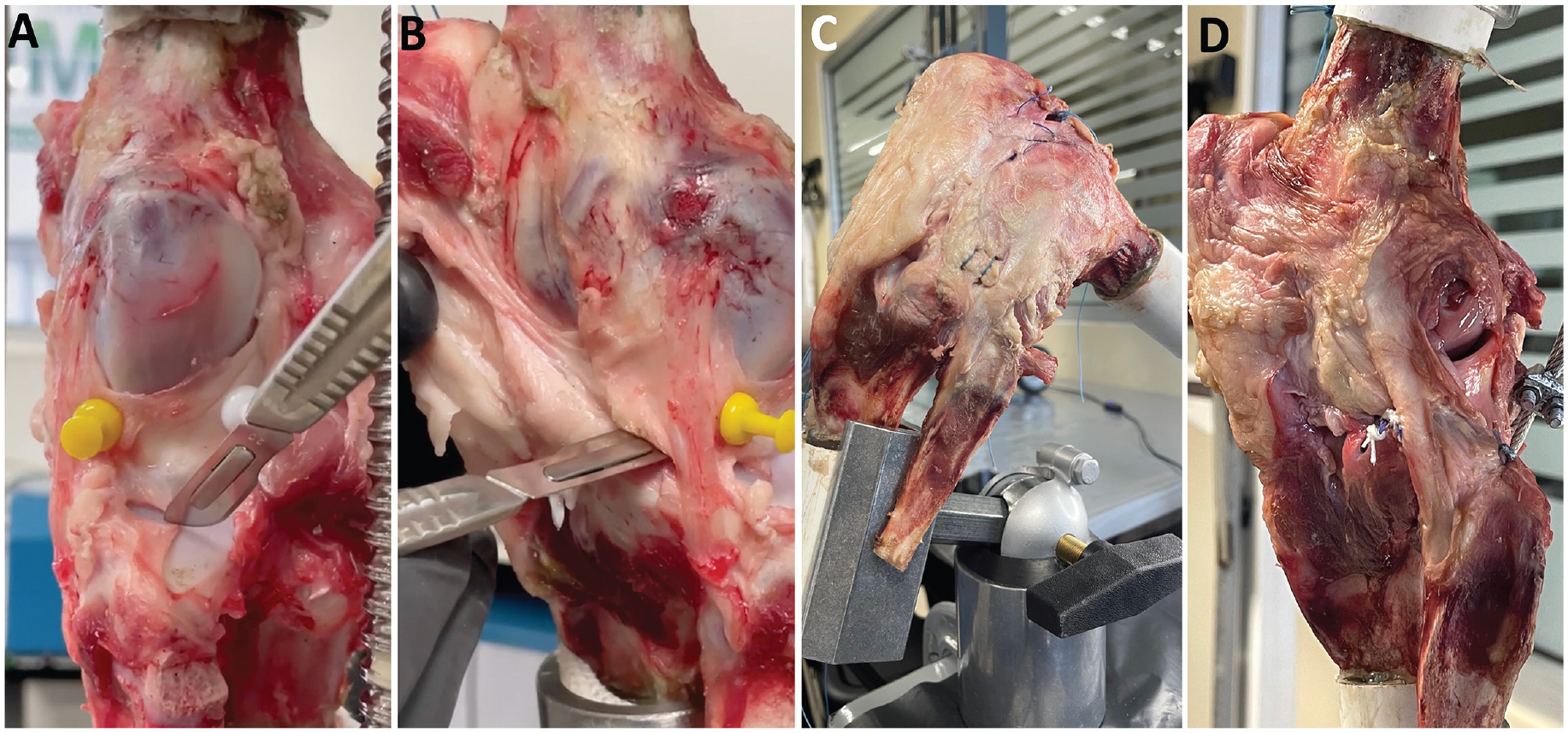
Lateral view of a porcine left knee showing the 4 different study conditions. (A) Isolated LMTL injury, (B) combined LMTL and MFL injury, (C) reconstruction of the LMTL with the open capsulodesis technique, (D) reconstruction of the LMTL and MFL with the centralization technique. LMTL, lateral meniscotibial ligament; MFL, meniscofibular ligament.
Statistical Analysis
Before performing the analysis, all numerical sets of data were tested for normal distribution using the Shapiro-Wilk test. Numerical variables are described as means and standard deviations, while categorical variables are described as frequencies and percentages.
Each measurement was performed by 3 independent observers (R.M.-A., R.A.E.-V., and S.P.). The observers made 2 alternating sets of measurements 50 minutes apart from one another and the difference between each set of measurements was used to calculate the relative intraobserver reliability. The significance of the absolute difference between measurements was also tested using the paired Student t test. If no significant difference was detected and the relative intraobserver reliability was <0.2%, the first measurement of the observer was used for further analyses. If this criterion was not met, the measurement was repeated after revising the technique of the observer. Regarding interobserver reliability, the difference between each set of measurements was used to compute the average interobserver difference, and the significance of the difference between each set of measurements was also tested using a 1-way analysis of variance test. If no significant difference was detected and the average interobserver difference was <0.01, any of the measurements was considered acceptable. If this criterion was not met, a consensus was reached by the 3 observers on the final measurement used for the rest of the analysis.
The difference in the degree of meniscal extrusion at baseline and after the axial load was applied, and at 30° and 60° of flexion, was compared in each group using the paired Student t test. Regarding the differences between the groups, comparisons were made based on the type of injury and type of reconstruction technique, with the knee at 30° and 60° of flexion, with the Student t test.
An a priori sample size calculation was performed using the model described by Kubota et al, 12 considering an expected effect size of 0.7 derived from the difference in degree of meniscal extrusion after the use of either reconstruction technique. With a precision of 0.05 and power of 80%, a sample size of 16 was enough for the determination of our outcome of interest. A decision was taken to increase the sample to 22 due to the availability of samples and the lack of previous models examining the biomechanical effects of the capsulodesis technique.
A P value threshold of <.05 was considered indicative of statistical significance for all the tests. All tests were performed using the IBM SPSS statistical package (Version 26) for Windows 11. The sample size calculation was performed using the G*Power statistical tool package for Windows 11 (Version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany).
Results
The percentage of interobserver variability for all meniscal extrusion measurements was <0.2%, which indicates a difference of <0.01 mm between each measurement. Therefore, no relevant interobserver error was considered. As for the interobserver reliability, the average difference between measurements was <0.01, indicating no impactful errors of measurements were detected. No significant difference was detected between the intra- or interobserver measurements.
The greatest meniscal extrusion occurred in the combined LMTL and MFL lesion group with the application of 200 N at 60° of flexion (25.11 ± 2.19 mm) (Figure 6 and Table 1). The lowest extrusion index occurred in the group in which the centralization technique was applied at 30° of flexion without the application of load (13.02 ± 0.54 mm) (Figure 6 and Table 1).

Bar graph showing mean meniscal extrusion measurements according to study and loading conditions and flexion angle. Error bars indicate standard deviations. LMTL, lateral meniscotibial ligament; MFL, meniscofibular ligament.
Meniscal Extrusion Measurements in the Different Groups by Flexion Angle and Load a
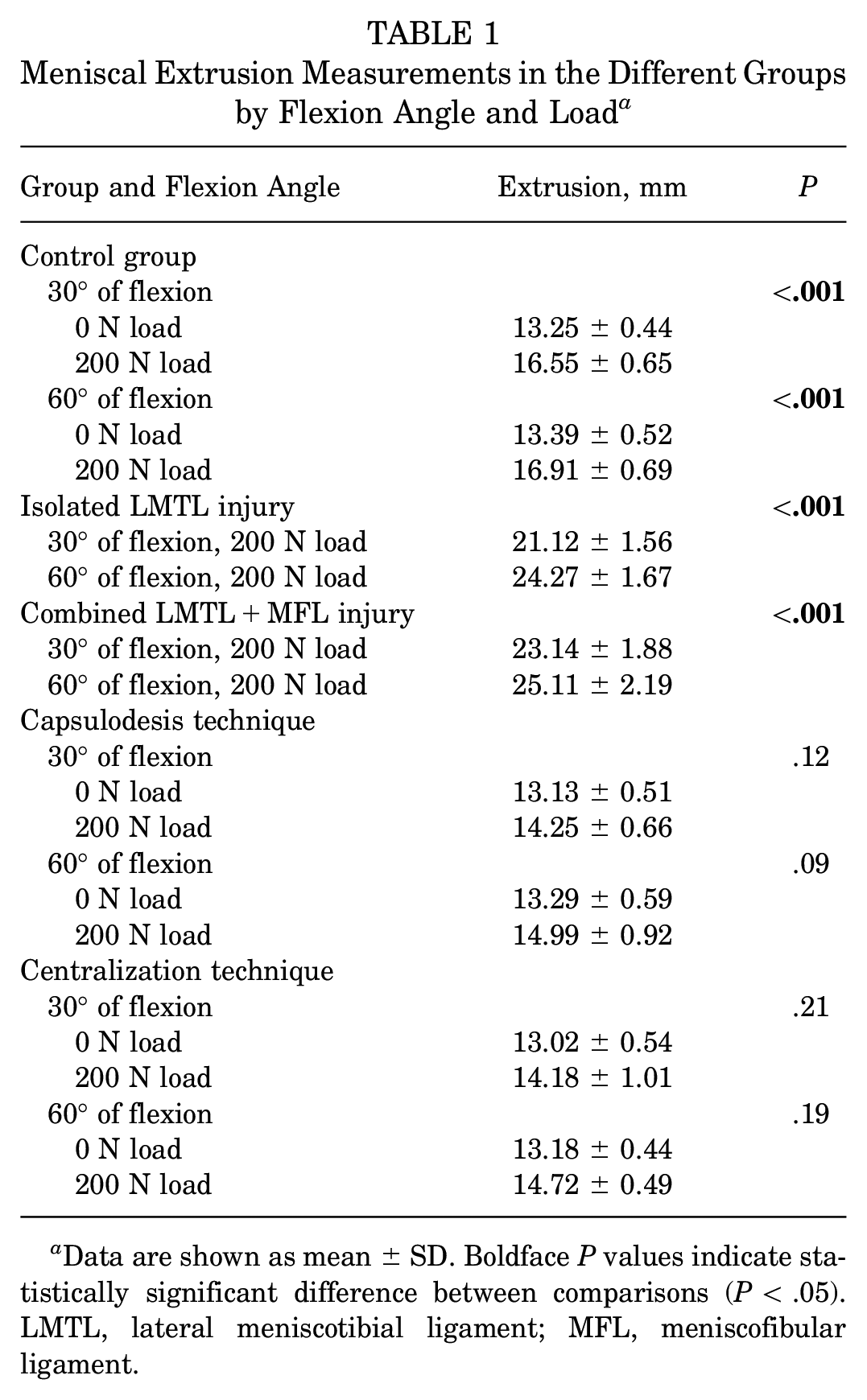
Data are shown as mean ± SD. Boldface P values indicate statistically significant difference between comparisons (P < .05). LMTL, lateral meniscotibial ligament; MFL, meniscofibular ligament.
The application of loading force significantly increased meniscal extrusion compared with the intact meniscus (P < .05) (Table 1). However, this increase did not occur with the application of both techniques. On the other hand, it was not compared with the state before the application of load in the situations of ligamentous rupture as it was considered that the meniscus had already been extruded previously with the application of the load to the original meniscus.
Regarding the differences in meniscal extrusion in the cases of load application, no significant differences were observed between the control group (intact meniscus) and the groups in which the reconstruction techniques had been performed. There were also no differences when comparing the results obtained between both reconstruction techniques. There were differences between the groups with ligament injuries and in the groups in which the reconstruction was performed when compared with the control group (P < .05 for both); this was also the case when comparing the state of injury of 1 ligament versus the injury of 2 ligaments with each other (P < .05) (Table 2).
Comparison of the Results Obtained Between the Different Study Groups During Load Application a

Boldface P values indicate statistically significant difference between comparisons (P < .05). LMTL, lateral meniscotibial ligament; MFL, meniscofibular ligament.
In all settings, the distance between the 2 markers increased with the knee flexion angle in the cases in which no load was administered. Conversely, there were no differences in the results between the 2 flexion angles when the 200 N load was applied (Figure 6). Finally, there were no significant differences in the results between the 2 flexion angles analyzed in this study in most cases. However, there were differences in the ligament injury groups (P < .05) (see Table 1).
Discussion
The present study demonstrated that the LMTL and the MFL act as restrictors of the radial mobility of the lateral meniscus during loading and that injury to them produces a significant increase in meniscal extrusion. Therefore, our first hypothesis was confirmed. Furthermore, this meniscal extrusion can be restored to its preinjury state by means of the open capsulodesis technique or the centralization technique, without significant differences between the 2 procedures. Using either the centralization or capsulodesis technique, the lateral meniscus was no longer displaced laterally. Therefore, our second hypothesis was confirmed.
As far as we know, this is the first study to analyze the biomechanical effects of an isolated and combined lesion as well as their reconstruction. Although there were no significant differences between the 2 reconstruction techniques, a somewhat greater decrease in extrusion was observed with the centralization technique. The fact that some modification in the capsulodesis technique was introduced may help explain this subtle difference. In addition, a modification was made in the centralization technique in this study to also perform a reconstruction of the MFL.
Previous studies have determined that isolated LMTL abnormalities lead to severe meniscal extrusion, even in the absence of other knee pathologies.7,11 A meniscotibial ligament injury leads to the dislodgment of meniscus from the tibial plateau, thereby losing its normal attachment sites and causing meniscal extrusion. 1 Previous studies in porcine models have been carried out under other pathological conditions that also led to meniscal extrusion. They include injury to the posterolateral meniscus root. Ozeki et al 24 found the greatest extrusion with the application of 200 N was 21.9 mm (range, 17.8-25.6 mm) and 15.3 mm (range, 12.9-18.0 mm) in the group that underwent posterior root injury and the centralization technique respectively, which represent values like those of the current investigation in which extrusion was greater after injury and lower following the reconstruction techniques. These differences could be explained because the injured structures in our experiment are different from theirs; however, both led to the appearance of meniscal extrusion. In addition, the differences in the way the centralization procedures were done in both studies might also have contributed to the slight biomechanical differences found. Like Kubota et al 12 in a study on porcine knees, very similar results confirming the fact that the meniscal extrusion increases with the degrees of knee flexion were seen in this study.
The MFL was found in all specimens studied. Therefore, we consider it an anatomically constant structure in humans and pigs. 22 The MFL connects the inferolateral portion of the body of the lateral meniscus, anteriorly and laterally, to the popliteus tendon with the head of the fibula. In its anterior portion, its fibers interconnect and are in continuity with the more posterior fibers of the LMTL. This observation had already been evidenced in a previous study. 21 Previous studies have hypothesized that the function of the MFL is to stabilize the lateral meniscus in external rotation and varus movements. This is due to the fact that, during dorsiflexion of the ankle, the fibula tends to rotate externally, causing a displacement of the external meniscus in that direction. 2 However, to our knowledge, this is the first study to analyze the biomechanical characteristics of the MFL. In addition, we believe that its true function is to reinforce the function of the LMTL and prevent anterolateral displacement of the lateral meniscus. This has been proposed previously in another study. 30 In that study, they also considered rebuilding this ligament during lateral allogeneic meniscal transplantation.
Limitations
The present study has several limitations. First, this was an in vitro bench test study using a porcine rather than a human model. Second, the meniscal extrusion was evaluated only on the mediolateral plane, leaving out evaluations in the anteroposterior plane. Third, only 2 flexion angles were considered, leaving aside greater angulations than 60°. Fourth, the number of samples was limited, although the current sample size was greater than that used in most biomechanical studies. Fifth, the surgical techniques evaluated were originally assisted arthroscopically and were adapted to be performed as open surgery for the purpose of the current work. Sixth, no determinations of the variability in pressure and load on the lateral meniscus were made.
Conclusion
The LMTL and MFL participate as restrictors of radial mobility of the lateral meniscus. Injury to these structures causes a significant increase in lateral meniscal extrusion and the centralization and the capsulodesis procedures reduce extrusion in a porcine model.
Footnotes
Acknowledgements
The authors thank Eric Goode for his help in correcting the manuscript. This work was carried out in the framework of the PhD program in Surgery and Morphological Sciences of the Universidad Autónoma de Barcelona, as part of the thesis by a compendium of publications of the first author of the study.
Final revision submitted August 1, 2023; accepted August 18, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Universidad Autonoma de Nuevo Leon (ref No. PI23-00044).