
Abstract
Background:
While increased posterior tibial slope (PTS) is an important risk factor for failure after anterior cruciate ligament (ACL) reconstruction, controversy exists regarding indications and outcomes of proximal tibia anterior closing-wedge osteotomy (ACWO) with concomitant ACL reconstruction in patients with ACL tears.
Purpose:
To assess clinical outcomes after combined ACL reconstruction and proximal tibia ACWO.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
In accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines, we performed a systematic review of the existing literature on ACWO and ACL reconstruction using PubMed (MEDLINE), Cochrane Library, Scopus, and Embase. The search phrases included “anterior closing wedge osteotomy,”“anterior closing wedge tibial osteotomy,”“anterior closing wedge proximal tibial osteotomy,”“anterior cruciate ligament,” and “revision anterior cruciate ligament.” Non-English publications and single-patient case reports were excluded. Extracted data included study details, patient demographics, patient-reported outcomes (PROs), clinical outcomes, radiographic outcomes, complications, and return-to-sport (RTS) rates.
Results:
A total of 6 studies with 110 patients (110 knees) were included. Two-stage ACWO and ACL reconstruction was reported in 2 studies of 78 patients (71%), while a single-stage technique was reported in 4 studies of 32 patients (29%). ACWO was performed in the setting of primary ACL tear in 23 patients (21%) and in recurrent ACL tear in 87 patients (79%). Patients demonstrated postoperative improvements in Lysholm, pivot-shift test, and side-to-side difference in anterior tibial translation. After ACWO, all studies reported mean postoperative PTS of <10° (range, 4.4°-9.2°). Of patients with available RTS data (n = 43), the same-level RTS rate ranged from 65% to 100%. A two-stage procedure reported in 1 study had a lower RTS rate (n = 13 of 20 [65%]) than that of 2 studies with single-stage procedure (n = 4 of 5 [80%] and n = 18 of 18 [100%]). The overall complication rate was 0.9% to 1.3%, and there were no reported ACL retears.
Conclusion:
The current evidence, which is constrained by the quantity and quality of studies, showed that ACWO with single- or two-stage ACL reconstruction in patients with ACL insufficiency and increased PTS was associated with significant improvements in PROs and high RTS rates.
Keywords
Anterior cruciate ligament (ACL) reconstruction remains the standard of care for young, active patients with ACL injuries, with an increasing incidence over the past 2 decades. 6 While ACL reconstruction has been associated with high return-to-sport (RTS) rates and improved clinical and functional outcomes, ACL retears are reported in up to 11% of adult patients, often necessitating revision surgery.15,24,25,35 A number of technique-related factors (ie, graft type, tunnel position, fixation method) and patient-related factors (age, sex, body mass index [BMI], activity level) have been associated with increased risk of ACL retear.3,35
Increased posterior tibial slope (PTS) is an important anatomic variable, and previous studies have demonstrated a strong association with increased risk of primary and recurrent ACL tears with increased PTS. A study by Webb et al 36 claimed that a tibial slope of 12° increases the likelihood of graft failure by 5 times after ACL reconstruction. Therefore, a tibial slope of 12° was recommended as the threshold for a slope-reducing high tibial osteotomy, which is consistent with the findings of previous investigations.2,4,7,18,23,27 Slope correction via proximal tibia anterior closing-wedge osteotomy (ACWO) may provide an effective surgical augment to ACL reconstruction in these patients. Previous biomechanical studies have demonstrated reduced anterior tibial translation after ACWO in ACL-deficient knees and after ACL reconstruction.11,20,21,32 In addition, ACWO has been shown to decrease forces across the ACL, suggesting a lower likelihood of retear after ACL reconstruction in patients with high PTS.10,38 Clinical studies have demonstrated ACWO to be safe and effective for decreasing PTS; however, the existing literature on clinical and functional outcomes after ACWO as an adjunct to ACL reconstruction is limited to small case series or case reports. This paucity of data has limited the generalizability of conclusions regarding outcomes after this procedure.
The purpose of this systematic review was to summarize the available literature on combined ACWO and ACL reconstruction in ACL-deficient knees, to assess patient-reported outcomes (PROs), objective outcomes, RTS rate, complications, and reoperations after ACWO. We hypothesized that ACWO in combination with ACL reconstruction is a safe procedure, resulting in favorable PROs, with a high RTS rate and a low complication rate.
Methods
Literature Search and Selection
A systematic review of the published literature on outcomes after ACWO and ACL reconstruction was performed. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) standards were utilized. 28 A database search was performed across PubMed (MEDLINE), Scopus, Cochrane Library, and Embase using the following search terms: “anterior closing wedge osteotomy,”“anterior closing wedge tibial osteotomy,”“anterior closing wedge proximal tibial osteotomy,”“anterior closing wedge tibial osteotomy” AND “anterior cruciate ligament,”“anterior closing wedge osteotomy” AND “anterior cruciate ligament,”“knee osteotomy” AND “anterior cruciate ligament,” and “knee osteotomy” AND “revision anterior cruciate ligament.” The search included studies from database inception through July 31, 2022.
After exclusion of 244 duplicates, a total of 256 unique citations between January 1, 1979, and July 31, 2022, were available for review; 20 studies were not human studies/available in English and were excluded. Abstracts were screened for the following inclusion criteria: clinical, functional or PROs after single- or two-stage ACWO with primary or revision ACL reconstruction and >2 patients in series. Case reports, abstracts, and biomechanical or animal studies were excluded. Studies were also excluded if they included patients who underwent additional osteotomies. After screening of abstracts, 8 full-text articles were eligible for review, with 6 studies included in the final analysis (Figure 1). For each full-text article reviewed, the reference section was searched for additional articles not retrieved by the first database search. Two independent reviewers (T.I. and T.U.) assessed the final full text-articles, and any disagreements were discussed with the other investigators (A.R. and S.M.) and resolved by consensus.
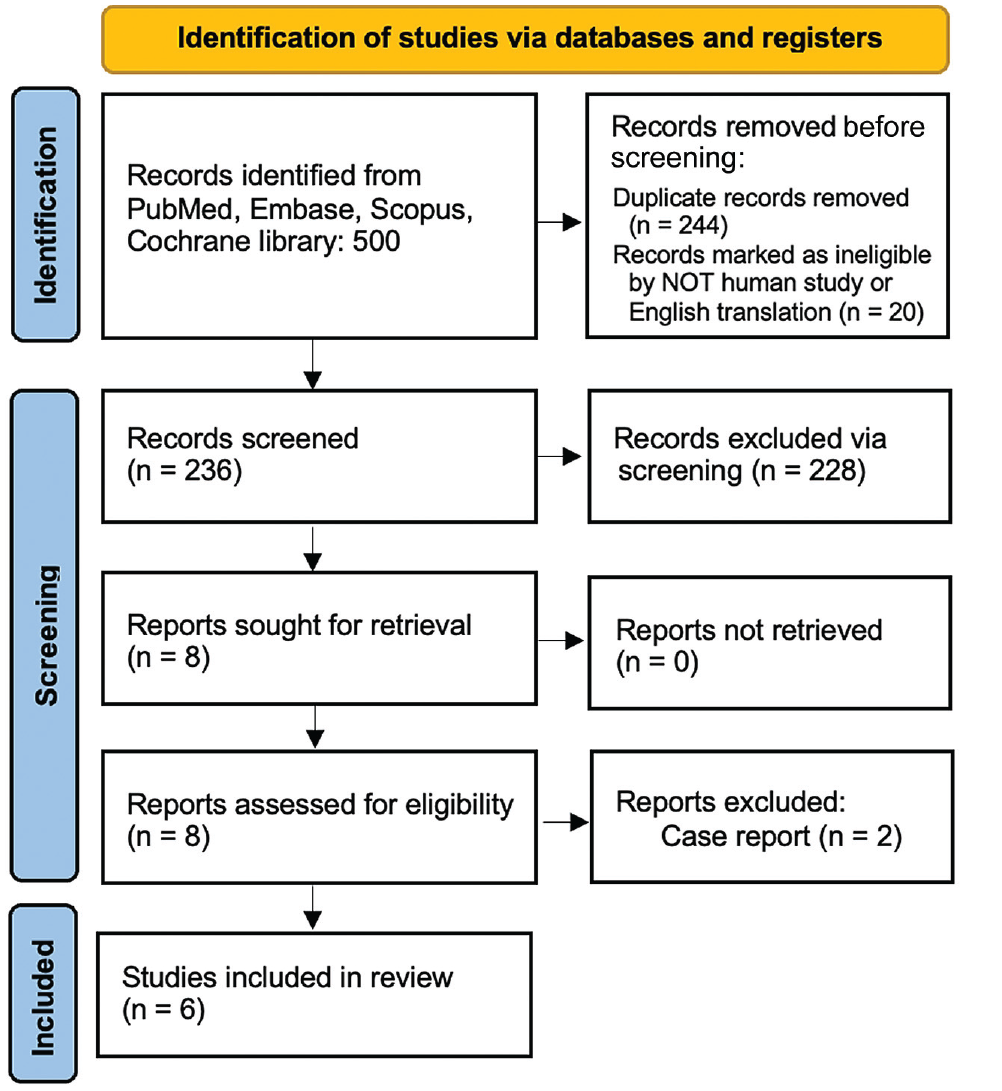
Flow diagram outlining the process of study selection.
Bias Assessment
Two authors (T.I. and T.U.) completed a quality assessment of the included papers to ensure that bias was minimized using the Methodological Index for Non-randomized Studies (MINORS) criteria. The lack of randomization and prospective comparison control groups in Level 4 studies might result in inherent selection and performance bias, particularly in populations with heterogeneous injury patterns. Selected studies were examined to ensure the authors reduced bias while acknowledging the limitations of such investigations. Any disagreements were discussed with the other investigators (A.R. and S.M.) and resolved by consensus.
Data Collection
Data extraction was completed by 2 independent reviewers (T.I. and T.U.), and disagreements were resolved by consensus. Extracted data included study characteristics (ie, accepted journal, study design, level of evidence), patient demographics (age, sex, BMI), duration of clinical follow-up, concomitant procedures, surgical technique (ie, primary vs revision ACL reconstruction), PRO measures, clinical examination (ie, Lachman grade, pivot-shift grade, collateral ligament stability), RTS rate, complications, and reoperations.
Statistical Analysis
Microsoft Excel Version 16 was used to analyze the data retrieved. This study used descriptive statistics in its analysis, reporting the total number of patients for each difference in surgical method and indication. Clinical outcomes and demographic information were provided as means and standard deviations, with ranges.
Results
This review included 6 studies,1,11,30,33,34,37 with a total of 110 patients (110 knees). All 6 studies were retrospective case series (Table 1). Of note, the study by Rozinthe et al 30 was a follow-up study using the same cohort of patients as the study by Dejour et al. 11 Mean age of the patients varied from 24 to 32.2 years (range, 16- to 49 years). The clinical outcomes and PROs were available in 52 patients (47.3%), with a minimum follow-up of 23 months. The MINORS score for methodological quality assessment ranged from 6 to 9.
Study Characteristics a
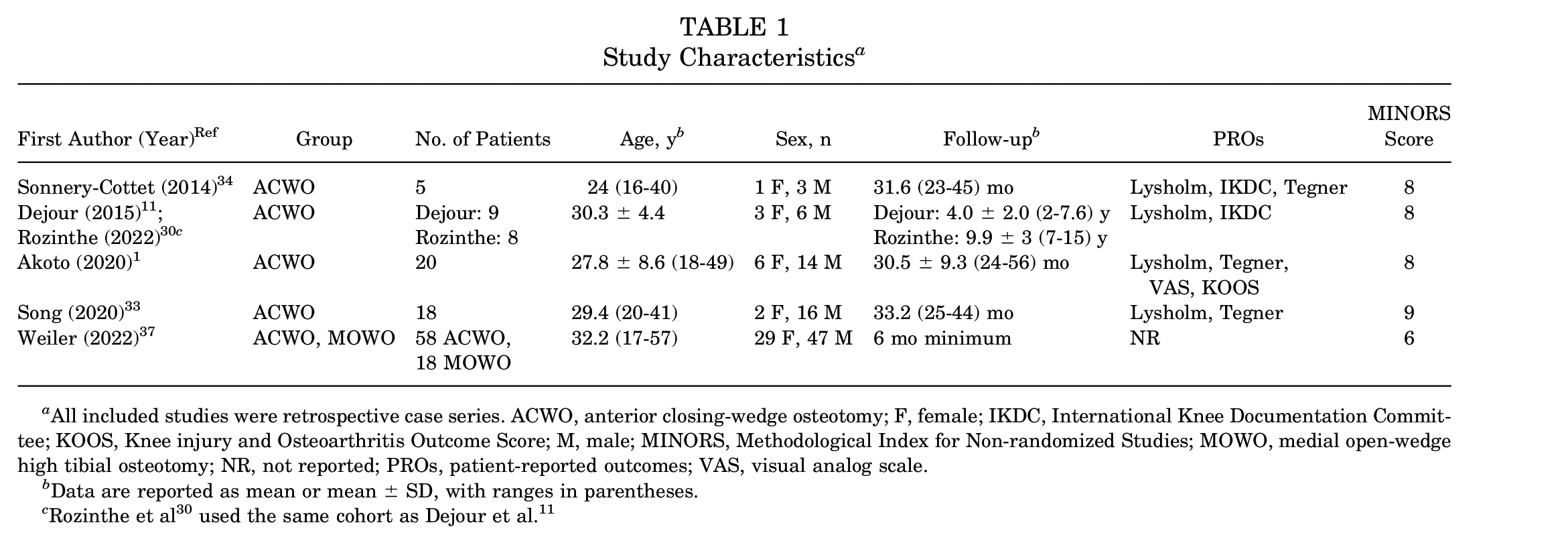
All included studies were retrospective case series. ACWO, anterior closing-wedge osteotomy; F, female; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; M, male; MINORS, Methodological Index for Non-randomized Studies; MOWO, medial open-wedge high tibial osteotomy; NR, not reported; PROs, patient-reported outcomes; VAS, visual analog scale.
Data are reported as mean or mean ± SD, with ranges in parentheses.
Surgical Data and Operative Technique
Two studies reported on 78 patients (70.9%) who underwent two-stage ACWO and ACL reconstruction,1,37 with 73 (93.5%) of these patients treated for recurrent ACL tear (Table 2). Three studies reported on 32 patients (29.1%) who underwent single-stage ACWO and ACL reconstruction,11,33,34 with 14 of these patients (43.8%) treated for recurrent ACL tear. Overall, primary ACL injuries comprised 21% (n = 23) of patients, whereas revision surgery comprised 79% (n = 87) of patients. All 9 patients from the Dejour et al 11 and Rozinthe et al 30 studies underwent a second revision ACL reconstruction surgery. The infra-, trans-, and supratuberosity approaches accounted for 60% (n = 66), 31.8% (n = 35), and 8.2% (n = 9) of the ACWOs performed in this group, respectively. The lateral extra-articular tenodesis (LET) was performed in addition to ACL reconstruction and ACWO in 26.4% (n = 29) of patients.
Surgical Data and Operative Technique Used in Each Study Reviewed a

Data are reported as n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; ACWO, anterior closing-wedge osteotomy; LET, lateral extra-articular tenodesis; MM, medial meniscus; LM, lateral meniscus; NR, not reported.
Patient-Reported Outcomes
Four studies reported PROs after ACWO with ACL reconstruction.1,30,33,34 The Lysholm score was included in all 4 studies. The other PROs included the International Knee Documentation Committee (IKDC) (2 studies),30,34 Tegner activity scale (3 studies),1,33,34 and the Knee injury and Osteoarthritis Outcome Score (KOOS) (1 study). 1 The P values for preoperative versus postoperative Lysholm and IKDC scores were statistically significant in all studies that provided them. In the 4 studies that provided Lysholm scores, the average scores after ACWO and ACL reconstruction were all higher than 70. In contrast, the average values before the procedure were all lower than 50. Table 3 presents these significant differences in preoperative versus postoperative PROs.
PRO Data for the Studies Reviewed a

Data are reported as mean (range) or mean ± SD (range). ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; NR, not reported; postop, postoperative; preop, preoperative; QoL, quality of life; Sport/Rec, sport and recreation; VAS, visual analog scale.
Clinical Outcomes
Four studies (52 patients) reported clinical outcomes after ACWO with ACL reconstruction.1,11,33,34 All studies reported significant improvement in side-to-side differences in anterior tibial translation, pivot shift, and the IKDC objective score from preoperative versus postoperative. All 4 studies found that the mean side-to-side difference in anterior tibial translation improved significantly, ranging from 6.1 to 11.4 mm (Table 4). There were no reports of ACL retear and no cases of revision surgery.
Objective Outcome Data for the Studies Reviewed a

Data are reported as number of patients unless otherwise indicated. Gr, grade; IKDC, International Knee Documentation Committee; NR, not reported; postop, postoperative; preop, preoperative; SSD, side-to-side difference.
Data are reported as mean or mean ± SD, with ranges in parentheses.
Radiologic Outcomes
All studies reported postoperative PTS after ACWO (Table 5). The mean preoperative PTS ranged from 13° to 18.5°. Postoperatively, all patients in all studies demonstrated a statistically significant decreased in PTS after ACWO, with average postoperative PTS values ranging from 4.4° to 9.2° (Table 5).
Radiologic Outcomes of PTS Data for the Study Reviewed a

Data are reported as mean ± SD (range) or mean (range). NR, not reported; postop, postoperative; preop, preoperative; PTS, posterior tibial slope.
Anterior closing-wedge osteotomy cohort (n = 58).
Return to Sports
Three studies (43 patients; 39.1%) reported RTS rates1,33,34 and demonstrated that 65% to 100% of patients were able to RTS at their preinjury level (Table 6). Akoto et al 1 reported that 13 (65%) of the patients who underwent two-stage ACWO and ACL reconstruction were able to return to their preinjury sports level. In comparison, 4 of 5 (80%) and 18 of 18 (100%) patients reported by Sonnery-Cottet et al 34 and Song et al, 33 who underwent single-stage ACWO and ACL reconstruction were able to return to the preinjury sports level. In contrast to the studies by Sonnery-Cottet et al 34 and Akoto et al, 1 all 18 patients described by Song et al 33 underwent primary surgery. Among the studies by Sonnery-Cottet et al, 34 Akoto et al, 1 and Song et al, 33 only Song et al 33 mentioned the level of sports of the patients on return to play. The mean postoperative Tegner scores reported in these studies were 7.2, 6.1, and 7.3, respectively (Table 3).
RTS Data a

RTS, return to sport.
Adverse Events and Complications
There were 2 reported complications across all studies. Akoto et al 1 reported 1 case (0.9%) of a postoperative hematoma that required evacuation at 4 days postoperatively. Weiler et al 37 reported 1 case (1.3%) of hardware infection at 5.5 months postoperatively, which was definitively treated with local debridement and removal of hardware. There were no cases of osteotomy nonunion or delayed union. There were no reported ACL retears after ACWO with ACL reconstruction. More than half of the knees analyzed were from the study conducted by Weiler et al, 37 which had a minimum follow-up period of only 6 months, making it a relatively short-term study.
Discussion
This systematic review included 6 studies of 110 patients who underwent either single-stage or two-stage ACWO and ACL reconstruction for ACL insufficiency with associated increased PTS. In this group, the majority of the procedures were performed in two-stage fashion (71%) and for recurrent ACL tear (79%). Postoperatively, patients demonstrated improvement in PROs, clinical examination, and radiologic parameters. In addition, this study demonstrated a 65% to 100% RTS rate after ACWO with ACL reconstruction, with higher RTS rates after single-stage procedures reported from studies by Sonnery-Cottet et al 34 (80%) and Song et al 33 (100%) compared with two-stage procedures reported by Akoto et al 1 (65%). However, other factors, such as primary or revision surgery, may need to be considered. The complication rate was 0.9% to 1.3%, and there were no reports of ACL retears or need for revision ACL reconstruction. However, most of the included knees are from Weiler et al, 37 which had short-term follow-up.
Brandon et al 5 previously demonstrated an association between ACL rupture and increased PTS. Furthermore, patients with increased tibial slope had a significantly higher failure rate after primary ACL reconstruction. 5 More recently, a comprehensive review of 20 studies by Liu et al 23 demonstrated that an increase in medial tibial plateau slope and lateral tibial plateau slope is associated with an increased likelihood of ACL graft failure after primary ACL reconstruction. However, controversy exists regarding the specific cut-off for excessive PTS, with reports of PTS between 7.4° and 17° associated with ACL reconstruction failure.4,18,22,23,26,27,31 Based on recent evidence, indications for ACWO include PTS >12° for recurrent instability and PTS >15° for primary ACL injury.2,11,12,19,29,36 In the current systematic review, the mean preoperative PTS in this review ranged from 13° to 18.5°, within this recommended range for ACWO.
Regardless of the surgical technique used, management of the tibial tuberosity is a critical consideration, as iatrogenic patella baja or patella alta may be induced by a poorly placed osteotomy.2,37 In general, there are 3 locations for creation of an ACWO relative to the tibial tuberosity: supratuberosity, transtuberosity, and infratuberosity. 2 The supratuberosity ACWO, initially described by Dejour et al, 11 does not require detachment of the patellar tendon but has been associated with interference with the ACL tibial tunnel.8,11,14,29 Alternatively, the transtuberosity approach is more effective at avoiding convergence with the ACL tunnel but requires detachment of the patellar tendon.1,12,34 In contrast, the infratuberosity approach involves performing the ACWO distal to the tibial tuberosity, but leaves the tuberosity intact. While the primary benefit of this approach is decreased risk of tibial tuberosity fracture and absence of interference with the ACL tibial tunnel, due to the more distal and oblique tibial cut, this technique requires stronger fixation. 33 In this systematic review, the infratuberosity approach was the most frequently used technique. Furthermore, there were no cases of tibial tuberosity nonunion or delayed union across all ACWO types, suggesting that all 3 ACWO techniques may provide reliable healing potential.
In this systematic review, patients demonstrated significant improvement in postoperative PROs after ACWO with ACL reconstruction in all studies. Patients also demonstrated favorable postoperative clinical outcomes, with no recurrent instability. Furthermore, complication rate after ACWO with ACL reconstruction was found to be only 0.9% to 1.3% in this review. However, it is difficult to infer that ACWO with ACL reconstruction had a low risk of complications, given that most included knees only had short-term follow-up. ACWO also has the potential to cause postoperative recurvatum, a condition that can increase the risk of ACL graft rupture, especially if the angle of recurvatum is >5°. 16 To prevent knee recurvatum, it is not recommended to overcorrect the PTS. Instead, some authors have suggested the use of a posterior cruciate ligament brace for postoperative recurvatum, with the PTS correction limited to 6° to 8°. In patients with hyperextension >10°, surgery may be avoided altogether.17,19
At the current time, there is no consensus on goal correction of PTS after ACWO. Based on our analysis, the average postoperative PTS in all included studies was <10°, with a range between 4.4°and 9.2°. The postoperative PTS value in all patients in this review was lower than the number suggested at risk for ACL rerupture by Dejour et al.10,11 Furthermore, Weiler et al 37 discovered no statistically significant difference in anatomic medial proximal tibial angle after the ACWO operation in the coronal view, indicating that this technique may only provide reliable sagittal alignment correction.
In this young, active patient population, RTS is an important outcome variable to consider. In this systematic review, 3 studies of 43 patients reported RTS rates, with 65% to 100% returning to same-level activity postoperatively. Only 1 study by Song et al 33 documented specific RTS activity levels, which in most cases were recreational basketball, football, and skiing. Interestingly, this systematic review suggests that two-stage ACWO with delayed ACL reconstruction appears to have a lower RTS rates compared with single-stage ACWO with concomitant ACL reconstruction. The prolonged recovery time associated with a two-stage procedure may be a contributing factor to this result, although further research is required to corroborate these findings. However, other considerations, such as primary or revision surgery, must be considered. In the study by Song et al, 33 a high RTS rate is predicted, given that all of their patients had primary ACL injuries.
While the present study reported favorable results for ACL reconstruction with ACWO, the absence of a comparison group precludes us from definitively concluding that ACWO is superior to other treatment modalities. Therefore, future studies should aim to compare the effectiveness of ACL reconstruction with ACWO with other treatment options, such as ACL reconstruction with a LET or ACL reconstruction alone.
Limitations
This study has a number of limitations. First, given the systematic review study design, there remains a possibility that our search criteria may have failed to capture all relevant citations. Of note, screening of all reference lists from all 8 reviewed full-text citations revealed no missing studies. Second, inherent biases and limitations of each of the included studies may limit the findings of the systematic review. All the studies included in this review were classified as Level 4 evidence and lacked a comparison group. Third, surgical techniques, patient populations, demographic data, and imaging protocols differed among the included studies. Several of the studies included in this review utilized additional methods, such as LET, and used various graft choices. Another important point to note is the variation in technique used to measure PTS, including use of the mechanical versus anatomic axis of the tibia, use of the medial tibial slope versus the lateral tibial slope, and use of long versus short lateral knee radiographs.9,13 In this systematic review, the majority of the studies utilized medial tibial plateau slope to evaluate PTS. However, these variations in measurement technique may result in discrepancies in PTS values. In addition, due to the limited number of studies, overall low level of evidence, and a high degree of methodologic variation, quantitative comparison and pooling of data was not possible. Finally, the wide variation in clinical, radiographic and PRO measures across the included studies prevents direct comparisons and limits generalizability.
Conclusion
The findings of this systematic review demonstrated that ACWO with ACL reconstruction may be of value as a surgical technique for addressing ACL insufficiency in patients with increased PTS, with low rates of ACL retear, improved PROs, and low complication rates. However, most of the included studies had short- or intermediate-term follow-up. Future prospective studies are required to evaluate long-term outcomes after ACWO with ACL reconstruction.
Footnotes
Final revision submitted May 22, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.R. has received consulting fees from Bodycad, Smith & Nephew, Xiros, Anika Therapeutics, Arthrex, Flexion Therapeutics, Stryker, and Heron Therapeutics; nonconsulting fees from Smith & Nephew and Arthrex; and education payments from Gotham Surgical Solutions & Devices. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.