
Abstract
Background:
Previous studies have described various techniques and confirmed the clinical utility of valgus stress radiography and stress ultrasound in overhead athletes. The addition of valgus stress and a high-resolution anatomic assessment of the elbow with magnetic resonance imaging (MRI) in the active throwing position (flexed elbow valgus external rotation [FEVER] view) can add valuable diagnostic or prognostic information in throwing athletes.
Purpose/Hypothesis:
The purpose of this study was to evaluate findings on MRI and subsequent performance in professional throwing athletes. It was hypothesized that joint space widening in the FEVER view would be predictive of performance and the risk of subsequent injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
All pitchers on 2 Major League Baseball teams who consented to participate during their preseason screening in 2019 and 2020 underwent standard and FEVER MRI, and performance data from the following season were recorded, including injuries, mean throwing velocity, number of innings pitched, strikeout percentage, walk percentage, weighted on-base average, and level of play reached (not signed, minor league, or major league). Categorical variables were compared using the Fisher exact test or chi-square test, and continuous variables were compared using the Kruskal-Wallis test, as appropriate. Ordered logistic regression was used to determine the independent factors predicting performance.
Results:
A total of 91 players underwent preseason imaging, and all players had subsequent performance data available. Multivariate analysis revealed that when controlling for age, mean velocity, history of injuries, presence of symptoms, and history of ulnar collateral ligament reconstruction, increased absolute joint space widening was predictive of a lower level of play (β = −0.63; P = .042). Univariate analysis demonstrated a significant correlation between relative joint space widening and level of play reached (β = −0.54; P = .034). Relative joint space widening remained a significant predictor of level of play (β = −0.87; P = .012) on multivariate analysis. Multivariate analysis also showed that both absolute joint space widening (β = −13.50; P = .012) and relative joint space widening (β = −13.60; P = .026) were predictive of the number of innings pitched in the subsequent season.
Conclusion:
The present study demonstrates that findings on MRI with valgus stress correlated with the level of play reached and number of innings pitched in professional throwing athletes.
The prevalence of ulnar collateral ligament (UCL) injuries and reconstruction has been steadily increasing in professional pitchers at all levels of play over the past decade. 13 Not all players who undergo UCL reconstruction are able to return to the same level of play or performance after surgery. 3 Given the impact and cost of UCL injuries for professional throwing athletes and Major League Baseball franchises, there is immense interest in improving the diagnosis and evaluating the risk of UCL injuries.
A standard evaluation of the UCL involves a history and physical examination, followed by imaging. Imaging typically includes radiography, followed by ultrasound or magnetic resonance imaging (MRI). 2 Standard MRI can provide important information to suggest a UCL injury, including thinning or thickening of the ligament, abnormal signal intensity, and ligament discontinuity or retraction. 4 MRI has been shown to be highly sensitive and specific for diagnosing complete UCL injuries in throwing athletes. 16 However, it is unclear whether findings on MRI with standard sequences are prognostic of the future injury risk or adaptive changes specifically found in throwing athletes.9,10 Magnetic resonance arthrography has been proposed because of its higher accuracy; however, it has a higher cost and associated procedural risk. 23 Furthermore, none of these imaging modalities evaluate the ligament in stressed or dynamic situations.
Previous studies have shown that the highest moment of torque and the greatest stress on the UCL occur during the late cocking/early acceleration phase of pitching, when the elbow is roughly at 90°.8,18 There is increasing interest in imaging the UCL in this position in which it is subject to stress. Stress radiography can be a useful adjunct to plain radiography; however, it provides an indirect evaluation of UCL competence and does not allow direct visualization of the ligament or other soft tissue structures. 19 There is increasing evidence to support the use of ultrasound for the dynamic evaluation of the UCL, showing that it effectively visualizes UCL abnormalities accurately and predicts future injuries inexpensively and quickly.5,12,24 However, ultrasound is operator dependent, and its examination is predominately limited to soft tissue structures. While MRI is the gold standard for the diagnosis of UCL injuries, studies have shown that a combination of MRI and stress ultrasound is more accurate than either modality alone. 21
Given the potential value of MRI as a tool for the evaluation of the UCL with valgus stress applied to the elbow, we developed the flexed elbow valgus external rotation (FEVER) view. The FEVER view is designed to be reproducible and minimize patient movement while applying valgus stress across the ulnohumeral joint in a position of shoulder flexion, shoulder external rotation, and elbow flexion, simulating the late cocking phase of pitching. In a pilot study, the FEVER view was found to increase reader confidence and identify additional UCL abnormalities without significant patient discomfort compared to standard MRI views. 14 Figure 1 demonstrates standard and FEVER views with minimal joint space widening compared with the FEVER view with an increased ulnar-sided joint space.
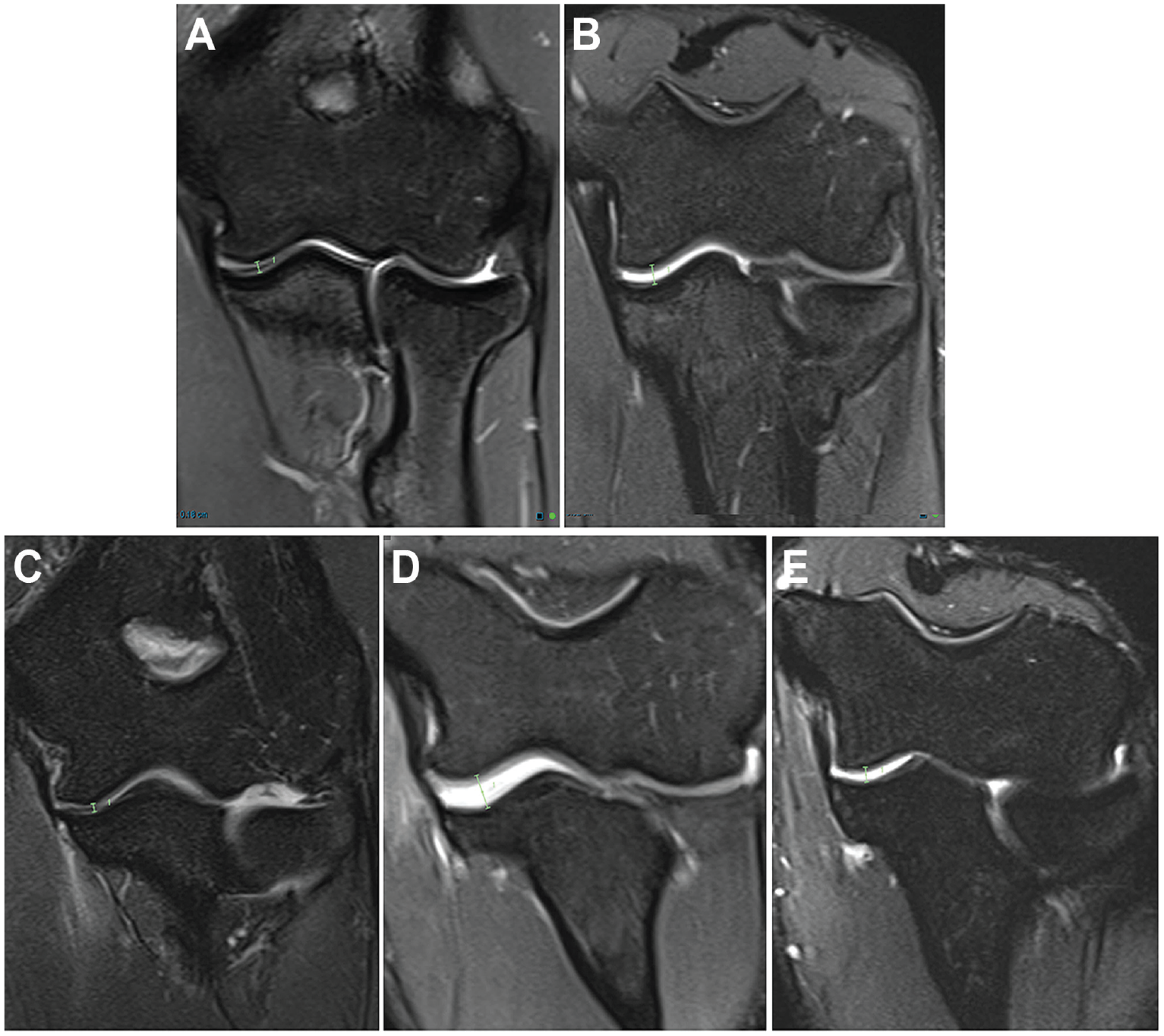
Standard and flexed elbow valgus external rotation (FEVER) views of coronal T2-weighted fat-suppressed magnetic resonance imaging. (A) Standard and (B) FEVER views of an asymptomatic athlete with an intact ulnar collateral ligament (UCL) showing typical joint space widening with the application of valgus stress. Ulnotrochlear joint space: 1.8 mm in standard view and 3.2 mm in FEVER view (green lines). Current (C) standard and (D) FEVER views and (E) 1-year prior FEVER view of a symptomatic athlete with a high-grade distal UCL tear demonstrating widening of the ulnar-sided joint space with the application of valgus stress. Ulnotrochlear joint space: 1.4 mm in current standard view, 5.0 mm in current FEVER view, and 2.5 mm in 1-year prior FEVER view (green lines).
In the present study, we sought to evaluate joint space widening seen on MRI performed as part of routine preseason screening and determine if any correlation exists with athlete performance in the subsequent season. We hypothesized that joint space widening in the FEVER view may be predictive of performance and the risk of subsequent injuries.
Methods
Study Population
All pitchers on 2 Major League Baseball teams who consented to participate during their preseason screening in 2019 and 2020 (n = 91) underwent standard and FEVER MRI. The imaging studies were requested by the head team physician of each of the 2 teams (G.W., E.L.). Institutional review board approval was obtained for the study protocol, and included players provided written informed consent before participation. All players who underwent preseason imaging were included. Players were excluded if they did not consent to the FEVER view in addition to standard sequences or if they were position players rather than pitchers. Players who were not signed or injured and did not have complete performance data were excluded from performance analysis but included with respect to level of play.
Imaging Protocol
MRI was performed with a 3-T system (MAGNETOM Vida; Siemens Healthineers). Sequences in standard and FEVER views were performed with a dedicated transmit-and-receive 16-channel elbow flex coil to optimize signal-to-noise ratio, contrast resolution, and spatial resolution. Standard sequences were obtained in the overhead elbow extended “superman” position and included the following: coronal T1-weighted (repetition time/echo time [TR/TE], 600-700 ms/10 ms), fat-saturated (FS) proton density–weighted (PDW) (TR/TE, 3000 ms/40-50 ms), and FS T2-weighted (TR/TE, 4000 ms/80-120 ms) imaging; axial T1-weighted and FS PDW imaging; and sagittal T1-weighted and FS T2-weighted imaging. For the FEVER view with valgus stress, the shoulder was immobilized in external rotation with the participant in the ipsilateral decubitus position. The shoulder and elbow were flexed to 90° with the palm up, and the elbow was elevated approximately 10 to 12 cm above the table using 2 foam pads and a sandbag or foam wedge. Then, two 1.7-kg sandbags (3.4 kg total) were placed on the distal forearm just proximal to the wrist to produce valgus stress and immobilization, resulting in approximately 10° to 20° of elbow-to-forearm valgus. After the dedicated elbow coil was placed, a 1.4-kg counterweight was applied at the elbow for immobilization and counterbalance, and the elbow was positioned at the isocenter of the magnetic field.
All sequences were performed at 2- to 3-mm slice intervals with 0.3-mm interslice gaps. The FEVER view was acquired by trained technologists before or immediately after standard sequences with the same MRI equipment and elbow coil, although with the participant in the lateral decubitus position lying on the pitching arm.
For the FEVER view, an oblique coronal FS PDW sequence (TR/TE, 3000 ms/40-50 ms) was obtained with a 256 × 256 matrix and 2-mm slice intervals with no interslice gap. Images were acquired through the UCL with an oblique angle of approximately 35°, approximating the course of the anterior bundle of the UCL in the flexed elbow position, as determined from the sagittal scout image (Figure 2). The FEVER view constituted approximately 10 minutes (4-7 minutes for positioning and scout imaging, 2-4 minutes for single FS PDW sequence) of the total examination time.

Patient positioning and sagittal scout magnetic resonance imaging in the flexed elbow valgus external rotation view. (A) Patient lying on the affected side with the shoulder and elbow in flexion and external rotation, the elbow elevated approximately 10 to 12 cm off the table, and two 1.7-kg sandbags applying valgus force. (B) Scout imaging showing an approximately 30° angle for image acquisition, demonstrated by the green lines aligned with the ulnar shaft and the 30° angle.
Data Acquisition
All images were read by 2 fellowship-trained musculoskeletal radiologists (M.S. and P.L.). The ulnotrochlear joint space was measured in standard and FEVER views from subchondral bone to subchondral bone at parallel joint surfaces along the approximate plane of the anterior bundle of the UCL based on the sagittal scout image (Figure 2). Absolute joint space widening was defined as the joint space in the FEVER view, while relative joint space widening was defined as the joint space in the FEVER view minus the joint space in the standard view.
Performance data from the following season were recorded. The specific performance variables were injuries, mean throwing velocity, number of innings pitched, strikeout percentage, percentage of players walked (walk percentage), weighted on-base average, and level of play reached. Level of play was categorized as not signed, minor league, or major league. If a player was injured after initial MRI but before the beginning of the season, his number of innings pitched was considered zero, and the remaining performance variables were not included.
Statistical Analysis
Descriptive statistics were used to summarize the data for all study variables. Continuous variables were reported as medians and interquartile ranges or means and standard deviations, as appropriate. Categorical variables were reported as counts and percentages. All categorical variables were compared using the Fisher exact test or chi-square test, and continuous variables were compared using the Kruskal-Wallis test, as appropriate. Ordered logistic regression was used to determine the independent factors predicting performance. All analyses were performed using STATA (Version 17; StataCorp), with a P value <.05 denoting statistical significance.
Power analysis was conducted based on a similar previous study that evaluated the risk of UCL injuries after stress ultrasound of medial joint space widening in throwing athletes. 24 With an alpha value of .05 and power of 80%, a sample size of 32 patients would be needed to determine a difference in UCL injuries based on increased joint space widening.
Results
A total of 91 players underwent imaging over a 2-year period (2019-2020). The mean age was 25.6 years (range, 20-38 years). Overall, 27 players were cut before the season (group 0), 50 players were assigned to a minor league level of play (group 1), and 14 players were signed as major league players (group 2). Player and injury characteristics, joint space widening in the FEVER view (absolute and relative), and performance variables are shown in Table 1. While there were no significant differences in absolute and relative joint space widening between groups, there was a trend toward decreased joint space widening as players achieved a higher level of play, with a mean absolute widening of 4.1, 3.8, and 3.5 mm (P = .107), respectively, and a mean relative widening of 2.1, 1.9, and 1.5 mm (P = .097), respectively, in groups 0, 1, and 2.
Player and Injury Characteristics, Joint Space Widening, and Performance Variables a

Data are reported as mean (range) or mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between groups (P < .05). UCLR, ulnar collateral ligament reconstruction.
Widening was measured in the flexed elbow valgus external rotation view.
With respect to specific variables, there was no significant difference between absolute and relative joint space widening in the players who were injured (P = .338 and .506, respectively). There was more absolute widening in patients with a history of UCL reconstruction (4.2 ± 0.92 vs 3.7 ± 0.91 mm, respectively; P = .036) but no difference in relative widening (2.1 ± 0.81 vs 1.8 ± 0.84 mm, respectively; P = .128).
Univariate regression analysis showed no significant correlation between absolute joint space widening and level of play reached (β = −0.44; P = .052) (Table 2). However, multivariate analysis revealed that when controlling for age, mean velocity, history of injuries, presence of symptoms, and history of UCL reconstruction, increased absolute joint space widening was predictive of a lower level of play (β = −0.63; P = .042). In addition, older age (β = 0.22; P = .007) and presence of symptoms (β = −1.90; P = .002) were significantly predictive of level of play (Table 3).
Results of Univariate Regression Analysis of Correlation of Level of Play With Absolute and Relative Joint Space Widening as Independent Variables a

Boldface P value indicates statistical significance (P < .05).
Results of Multivariate Regression Analysis of Correlation of Level of Play With Absolute Joint Space Widening as Independent Variable a

Boldface P values indicate statistical significance (P < .05). UCLR, ulnar collateral ligament reconstruction.
Univariate analysis demonstrated a significant correlation between relative joint space widening and level of play reached (β = −0.54; P = .034) (Table 2). This remained a significant predictor of level of play (β = −0.87; P = .012) on multivariate analysis when controlling for age, mean velocity, history of injuries, presence of symptoms, and history of UCL reconstruction. Once again, older age (β = 0.21; P = .012) and presence of symptoms (β = −1.93; P = .002) were also predictive of level of play (Table 4).
Results of Multivariate Regression Analysis of Correlation of Level of Play With Relative Joint Space Widening as Independent Variable a
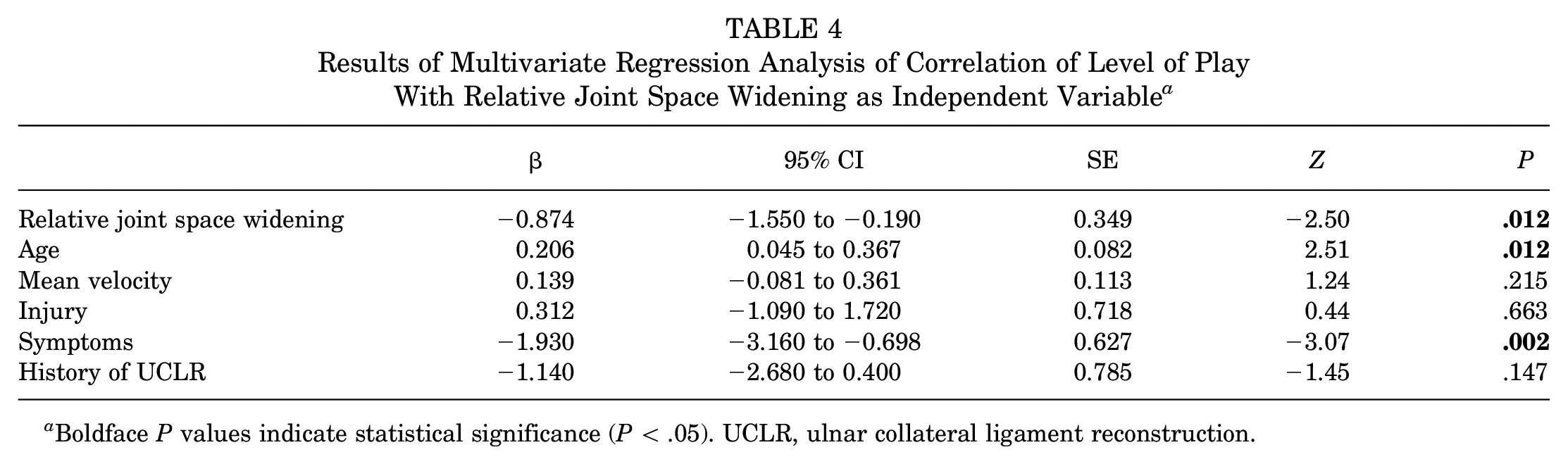
Boldface P values indicate statistical significance (P < .05). UCLR, ulnar collateral ligament reconstruction.
Multivariate analysis showed that both absolute (β = −13.50; P = .012) and relative (β = −13.60; P = .026) joint space widening were predictive of the number of innings pitched in the subsequent season (Tables 5 and 6). Age, mean velocity, history of UCL reconstruction, history of injury, and presence of symptoms were not significantly correlated. With respect to performance variables, no significant correlation was found between either absolute or relative joint space widening and strikeout percentage or walk percentage.
Results of Multivariate Regression Analysis of Correlation of Innings Pitched With Absolute Joint Space Widening as Independent Variable a

Boldface P value indicates statistical significance (P < .05). UCLR, ulnar collateral ligament reconstruction.
Results of Multivariate Regression Analysis of Correlation of Innings Pitched With Relative Joint Space Widening as Independent Variable a

Boldface P value indicates statistical significance (P < .05). UCLR, ulnar collateral ligament reconstruction.
Discussion
In the present study, multivariate analysis revealed that when controlling for age, mean velocity, history of injuries, presence of symptoms, and history of UCL reconstruction, increased absolute joint space widening was predictive of a lower level of play (β = −0.63; P = .042). Univariate analysis demonstrated a significant correlation between relative joint space widening and level of play reached (β = −0.54; P = .034). Relative joint space widening remained a significant predictor of level of play (β = −0.87; P = .012) on multivariate analysis. Multivariate analysis also showed that both absolute (β = −13.50; P = .012) and relative (β = −13.60; P = .026) joint space widening were predictive of the number of innings pitched in the subsequent season.
Professional pitchers place a tremendous amount of stress on the UCL of their elbow during the late cocking and early acceleration phases of throwing.7,8 Several studies have demonstrated changes that occur in the UCL over time, including ligament thickening, hypoechoic foci, calcification, and joint laxity.4,9,10,15,19 With respect to joint laxity in particular, a number of studies comparing throwing and nonthrowing arms have found increased joint space widening in the throwing arm with the application of valgus stress.5,6,17,22 There are conflicting data on whether these adaptive changes predispose throwing athletes to injuries.
Gutierrez et al 10 evaluated MRI scans of 26 professional throwing athletes who went on to pitch a mean of 1111.7 innings. They found various rates of positive findings on MRI, including UCL remodeling, partial UCL tears, ossification at the sublime tubercle, posteromedial articular cartilage loss, insertional triceps tendinitis, common extensor and/or flexor origin degeneration, and joint effusion. They found that none of these correlated with the number of innings pitched; however, they noted some trends that may have been insignificant because of their sample size.
In contrast, another MRI study looking at 41 asymptomatic pitchers with no history of placement on the disabled list (DL) who underwent preseason screening over 12 years found that some MRI findings were significantly correlated with future placement on the DL. 9 Players who were placed on the DL had a higher rate of UCL heterogeneity, humeral-sided partial tears, and signs of posteromedial impingement than those who did not become injured. Pitchers with increased UCL heterogeneity also had a lower career strike percentage and fastball percentage, with a smaller number of innings pitched than those with normal MRI findings.
Shanley et al 24 performed dynamic valgus stress ultrasound in 70 asymptomatic professional baseball pitchers during preseason training. They found that pitchers who subsequently went on to have an injury had significantly more joint space widening with valgus stress than those who did not become injured. Further analysis showed that specifically those patients with ≥5.6 mm of widening had a 6 times higher chance of becoming injured than those with <5.6 mm. They also found a statistically significant difference in the absolute ulnar-sided joint space between patients who injured their UCL and those who did not: 6.5 versus 5.3 mm, respectively. This contrasts with the present study, which did not demonstrate a correlation between joint space widening and injuries.
The gold standard for the diagnosis and evaluation of UCL injuries is MRI, as it can show soft tissue structures with high definition and evaluate other structures in the elbow joint with high intraobserver and interobserver reliability.16,19,20 However, typical MRI evaluates the UCL in a position of rest, and images are usually not obtained in the plane of the anterior bundle of the UCL, as in this study. Additionally, MRI may not be as valuable for the diagnosis of partial UCL tears. 11
The FEVER view was developed to improve the diagnostic accuracy of MRI as a tool for evaluating the UCL in throwing athletes. 14 It has previously been shown to be a safe, reliable method to produce valgus stress across the elbow and increase reader confidence for musculoskeletal fellowship-trained radiologists. 14 The main advantage of this view is that it can be added to standard routine MRI with little time and expense. In addition to the application of valgus stress, images are taken in the plane of the UCL. The combination of imaging in the standard view and the FEVER view allows for the evaluation of the UCL to include joint space widening under stress.
The present data indicate that there were correlations between joint space widening in the FEVER view with the level of play reached and the number of innings pitched in the subsequent season when controlling for other variables including age, history of UCL reconstruction, and mean pitching velocity. Although the differences noted between participants were small, there are previous data to suggest that in high-level throwing athletes, millimeters of joint space widening can suggest UCL incompetence or adaptive changes, with a predictive value for subsequent injuries. In a study of 273 baseball players with a UCL injury or complete tear who underwent UCL reconstruction, Bruce et al 1 performed stress radiography on dominant and nondominant arms as part of their routine preoperative evaluation. They found that the overall cohort had 0.4 mm of joint space widening, while patients with complete tears had 0.6 mm versus 0.1 mm for those with incomplete tears. Additionally, the present study demonstrates that while there were no significant differences between groups with respect to mean joint space widening, multivariate regression analysis showed that a greater amount of widening was predictive of a decreased number of innings pitched. Additionally, while it was not statistically significant, there was a trend toward decreasing absolute and relative joint space widening as the level of performance increased. The data also showed that group 0, or pitchers who were not signed to a minor or major league, had the highest mean absolute and relative joint space widening, although this was statistically insignificant. Moreover, they had the highest proportion of a history of UCL reconstruction, and this was statistically significant. It is interesting to note that despite no statistically significant difference in joint space widening, pitchers who were cut had a higher rate of previous UCL reconstruction.
However, it is unclear whether measuring the ulnar-sided joint space in throwing athletes is a reliable metric, as there may be variability in throwing athletes and imaging modalities. In a study of 736 pitchers, Ciccotti et al 5 found increased baseline joint space widening in throwing versus nonthrowing arms on stress ultrasound. They found a statistically insignificant trend toward increasing joint space widening in players who incurred a subsequent UCL injury as well as a mean increase of 0.78 mm in elbows of pitchers who underwent stress ultrasound at a later time point. This brings into question the accuracy of values collected at a single time point without considering pitching history, which is a weakness of the present study.
Limitations
There are limitations to the present study. While certain performance variables were accounted for, there are certainly other factors that contribute to whether a player reaches a higher level of play that were not controlled for. Additionally, it is possible that other variables, while controlled for, may not have been significant in this study, as it was not powered to detect a difference in these variables. In particular, the rate of previous UCL reconstruction was higher in players who were not part of a minor or major league roster. We did not consider pitch counts or pitching position, which could significantly impact the risk of injuries. In addition, we did not evaluate whether other findings noted in the FEVER view affect subsequent performance. The use of 2 sandbags on the wrist was also based on expert opinion rather than objective data and does not have a specific established relationship with valgus stress experienced during pitching.
Additionally, the methodology utilized during imaging can result in variable torques applied because of the variation in forearm length rather than a standardized distance from the elbow when placing the sandbags. No corroborative clinical or stress imaging (radiography or ultrasound) was performed. While these studies would add important clinical information, they could not practically be added or justified in routine preseason physical screening of these athletes. Overall, the incidence of injuries was low, and a larger sample size may show correlations not identified in the present study. This is the first study to evaluate findings on valgus stress MRI and performance in the subsequent season in professional baseball pitchers, and further investigation is warranted. Moreover, the present study population consists of professional pitchers, and these data may not be applicable to throwing athletes in other sports or pitchers with a lower level of play. Future directions include evaluating specific findings in the FEVER view and their correlation with performance and the risk of injuries as well as examining the FEVER view in pitchers with and without a history of UCL reconstruction and the influence of this on subsequent performance.
Conclusion
The FEVER view is a practical method of adding a valgus stress evaluation to routine MRI in throwing athletes. The present study demonstrates that findings on MRI with valgus stress correlated with the level of play reached and number of innings pitched in professional throwing athletes.
Footnotes
Final revision submitted March 1, 2023; accepted June 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.L. has received royalties from Arthrex, nonconsulting fees from Arthrex, consulting fees from Arthrex, hospitality payments from Steelhead Surgical, and education payments from Goode Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Touro University Nevada (TUNIRB000070).