
Abstract
Background:
Current evidence supports favorable short-term clinical outcomes with few complications after surgical management of proximal hamstring injuries; however, the durability of clinical benefits beyond approximately 2 years after surgery is unknown.
Purpose:
To evaluate patient-reported clinical outcomes and complication rates associated with open and endoscopic repair of proximal hamstring tears at minimum 5-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
A single-surgeon registry of patients was queried between October 1, 2014, and December 31, 2017, to identify patients who underwent open or endoscopic repair of a proximal hamstring tear. Patients who reported minimum 5-year follow-up data were included. Multiple patient-reported outcome measures, including the Hip Outcome Score Activities of Daily Living (HOS-ADL) and Sports-Specific (HOS-SS) subscales, 12-Item International Hip Outcome Tool (iHOT-12), and Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function (PF) and Pain domains, along with surgical complications, were analyzed.
Results:
Among 35 eligible patients (65.7% female; mean age, 52.3 ± 8.4 years), 24 had full-thickness tears and 11 had partial-thickness tears. There were 23 open repairs and 12 endoscopic repairs. Mean duration from symptom onset to surgical intervention was 37.9 weeks (range, 1.3-306.9 weeks). At a mean follow-up of 69.0 months (range, 60.0-95.0 months), mean postoperative outcome scores were as follows: HOS-ADL, 86.8 ± 12.7; HOS-SS, 83.1 ± 19.5; iHOT-12, 86.3 ± 14.9; PROMIS-PF, 50.0 ± 11.8; and PROMIS–Pain, 50.2 ± 7.9. Regarding complications, 28.6% of patients had a complication including persistent peri-incisional numbness (11.4%), wound infection (11.4%), postoperative neuropathy (8.6%), and revision surgery (2.9%).
Conclusion:
Both open and endoscopic surgical techniques for repair of proximal hamstring injuries produced favorable patient-reported clinical outcomes at a minimum 5-year follow-up.
Hamstring injuries are among the most frequently encountered lower extremity conditions experienced by recreational and elite athletes alike, with a reported incidence of 30%.1,3,4 Frequently, hamstring injuries can occur in traumatic injuries of rapid, explosive acceleration, such as sprinting, water skiing, soccer, and football.1-3,8,21 While acute strains of the hamstring muscle belly occur more commonly and are often amenable to nonoperative treatment, tears of proximal hamstring tendons at their origin on the ischial tuberosity are relatively less common and may require surgical intervention. Further, chronic, attritional injury to the proximal hamstring tendons can cause an insidious onset of progressive pain and dysfunction recalcitrant to nonoperative management.7,17 Surgical indications for proximal hamstring injuries are predicated on the number of tendons involved, tear severity (full thickness vs partial thickness), injury chronicity, amount of tear retraction, quality of the remaining hamstring muscle, and patients’ current and desired activity levels.9,19
Traditionally, an open surgical technique has been the gold standard approach for surgical repair of proximal hamstring tears.11,13 However, open repair has been associated with surgical complication rates of up to 23.2%, including neurologic complications, peri-incisional numbness, surgical-site infection, and tendon rerupture. 6 Since its initial description in 2012, 10 an endoscopic approach has gained traction for its minimally invasive approach and improved visualization of both the hamstring footprint on the ischium and adjacent neurovascular structures.11,13 Favorable outcomes and high rates of return to sporting activities have been reported for both approaches. Following endoscopic surgical management, previous studies have reported significant improvements in patient-reported outcomes (PROs), high return to work/sport achievement, and high satisfaction rates at minimum 1- and 2-year follow-up, respectively.14,15 Similarly, high patient satisfaction and favorable PROs among patients undergoing either open or endoscopic surgical treatment for chronic tears (ie, >4 weeks from injury) at a minimum 2-year follow-up have also been demonstrated. 17 The available literature, therefore, is adequate with evidence to support favorable short-term outcomes after surgical treatment of proximal hamstring injuries. However, to our knowledge, there is no evidence on the durability of these clinical benefits at ≥5 years postoperative follow-up.
The aim of the present investigation was to evaluate postoperative clinical outcomes and surgical complications of both open and endoscopic repairs of proximal hamstring tears at a ≥5-year follow-up. We hypothesized that patients undergoing proximal hamstring repair would have good outcomes after surgery that would be maintained at 5-year follow-up.
Methods
Patient Selection
Institutional review board approval was obtained before study initiation. A retrospective review of patients who underwent primary proximal hamstring repair by the senior author (S.J.N.) was performed from a single-institution repository. All patients provided written, informed consent to be included in the repository. Included were patients who had undergone either primary open or endoscopic hamstring repair from October 1, 2014, to December 31, 2017, with 5-year follow-up data, as determined by either completion of ≥1 PRO or secondary revision case. Patients who had undergone prior hamstring surgery, were indicated for concomitant hip procedures (eg, hip arthroscopy), claimed workers’ compensation for their operative condition, or underwent hamstring reconstruction with an allograft were excluded. Patient characteristics including sex, age, and body mass index (BMI) as well as injury characteristics including mechanism of injury, duration of pain, and type of pain onset (acute vs insidious) were collected. Intraoperative findings were collected, including the extent of tendon tear (full thickness vs partial thickness) and amount of tendon retraction.
A total of 56 patients underwent primary proximal hamstring repair between October 1, 2014, and December 31, 2017. Two patients were excluded for their status as a workers’ compensation case, 1 patient had a concomitant hip arthroscopy procedure, and 4 patients had chronic and extensively retracted tears and underwent hamstring allograft reconstruction. Fourteen patients were unable to be reached to provide outcome data at ≥5 years postoperatively, resulting in 35 patients (71.4% compliance) included in our analysis (Figure 1).
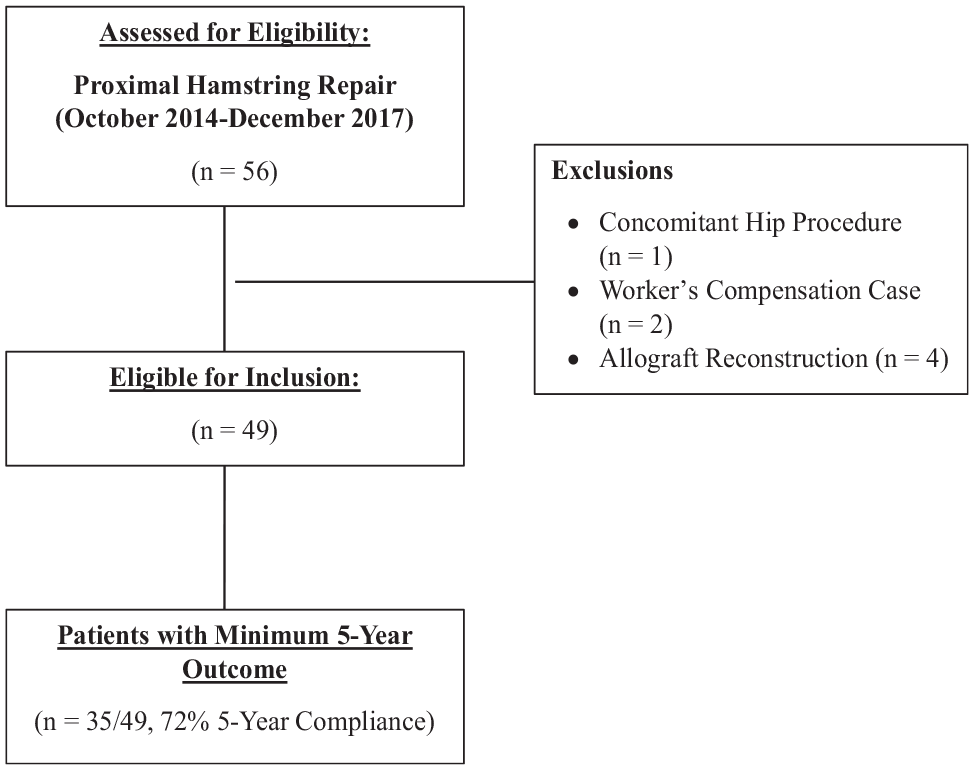
CONSORT (Consolidated Standards of Reporting Trials) diagram of patient selection for this study.
Preoperative MRI Assessment
All patients with clinical suspicion for a proximal hamstring tear underwent magnetic resonance imaging (MRI) of the injured hip with explicit instructions to capture and evaluate the integrity of the proximal hamstring attachment to the ischial tuberosity. For this study, a fellowship-trained musculoskeletal radiologist (J.W.E.) reviewed all MRI scans to assess the severity of proximal hamstring tear (full thickness vs partial thickness). A partial-thickness tendon was defined as a lesion to the conjoint tendon or the semimembranosus tendon. For full-thickness tears, the amount of hamstring tendon retraction from its origin on the ischial tuberosity was also measured (Figure 2).

Coronal magnetic resonance imaging measurement of a full-thickness proximal hamstring avulsion with 4.2 cm of retraction (yellow line).
Patient Stratification by Tear Pattern and Procedure
Patients were grouped into the following categories: procedure type (open vs endoscopic), chronicity (acute vs chronic), and tear size (partial vs complete). Chronic cases were defined as ≥4 weeks duration of pain before surgery, as previously described. 17 Patients with full-thickness tears in both the open and the endoscopic cohort were categorized based on having <3 cm or >3 cm of retraction based on MRI.
Surgical Indications
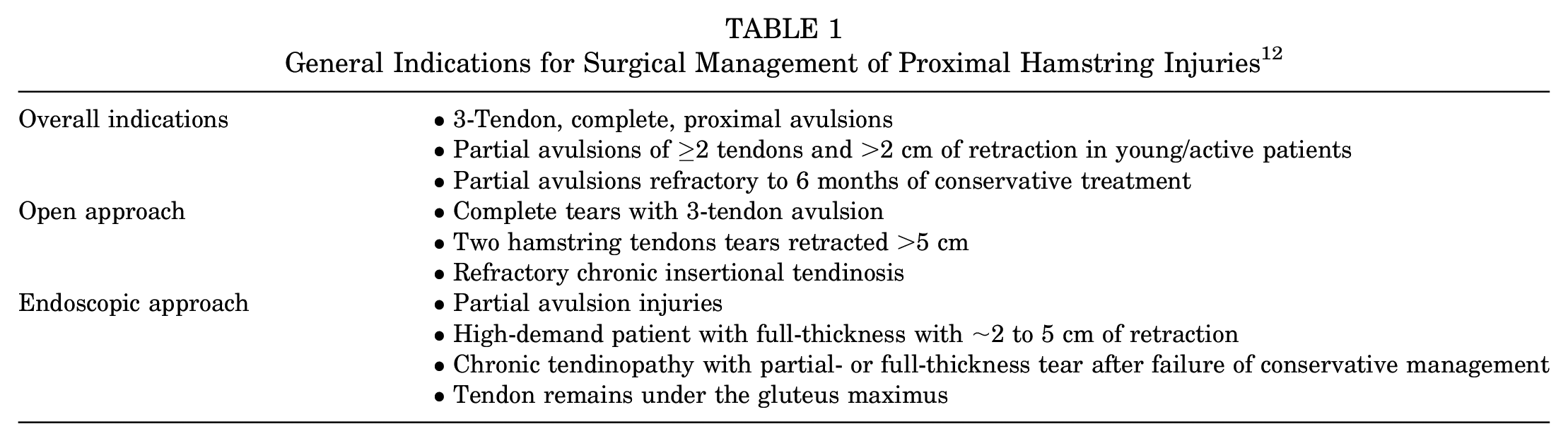
All surgical procedures were indicated and performed by the senior author (S.J.N.) using criteria outlined in Table 1.
General Indications for Surgical Management of Proximal Hamstring Injuries 12
Surgical Technique: Open Approach
With the patient placed in the prone position and following standard surgical-site preparation and draping, a 5-cm incision was made within the gluteal crease and centered over the ischial tuberosity. After subcutaneous tissue dissection, a transverse incision was made through the gluteal fascia. The gluteus maximus was retracted proximally and dissection was carried out bluntly to identify the sciatic nerve and, if necessary, free the nerve from adjacent adhesions. With the sciatic nerve visualized and retracted laterally, the hamstring tendon stump was dissected and mobilized proximally, and traction sutures were placed. The footprint on the ischial tuberosity was cleaned of soft tissue debris and the bone decorticated with a high-speed burr (Stryker Endoscopy) to promote tendon-to-bone healing. After bony preparation, 1 to 2 triple-loaded suture anchors (AlphaVent, Stryker; Kalamazoo, MI) were placed into the ischium and sutures were passed through the tendon stump in a simple, running configuration along the medial and lateral borders of the tendon. Utilizing a docking technique, the tendon was reduced down to the ischial tuberosity. Once the knots were secured, the suture strands were cut, the sciatic nerve was reevaluated, and meticulous hemostasis was obtained before a layered wound closure.
Surgical Technique: Endoscopic Approach
The endoscopic operative technique employed in this patient cohort has been reported previously 22 ; however, a brief review is provided. As when performing an open approach, the patient was placed in the prone position. Endoscopic portals were created along the gluteal crease, with the first, medial portal established just medial to the lateral border of the ischial tuberosity and approximately 2 cm distal to the distal ischial border. To avoid iatrogenic sciatic nerve injury, the lateral portal was then established under spinal needle localization approximately 3 to 4 cm lateral to the first portal, also within the gluteal fold. Next, an arthroscopic shaver (4.0 Smooth Bite; Stryker Endoscopy) was placed through the lateral portal to perform an ischial bursectomy, improving visualization and clearing the subgluteal space. Care was taken to not injure the nearby neurologic structures including the posterior femoral cutaneous nerve and sciatic nerve (Figure 3A). Using the tip of the shaver or switching stick, the tear was identified by palpating the tendon footprint against the ischium, which was ballotable relative to intact tendon. Once the tear was identified, radiofrequency ablation (RFA) was used to open the sheath longitudinally (Figure 3B). The ischium was prepared using the RFA to clear soft tissue and a 5.5-mm cylindrical burr to decorticate the tendon footprint, and 2 triple-loaded 5.5-mm AlphaVent polyetheretherketone suture anchors (Styrker) were placed after drilling, punching, and tapping (Figure 4, A and B). Next, using a tissue penetrator from the lateral portal, sutures were passed through the lateral aspect of the tendon split in a combination of simple or mattress suture configurations (Figure 4C). Subsequently, the tissue penetrating device was then used from the medial portal to retrieve the sutures from the medial aspect of the tendon. Finally, the sutures were tied from the lateral portal using half hitches on alternating posts in a mattress configuration (Figure 4D).

(A) Identification and release of the sciatic nerve (yellow arrow) that lay approximately 1.2 ± 0.2 cm lateral from the lateral aspect of the ischial tuberosity. (B) Identification of the proximal hamstring defect (red arrow) was performed by palpating the tendon with radiofrequency ablation or arthroscopic shave, as torn tissue is more ballotable and softer than intact tissue.
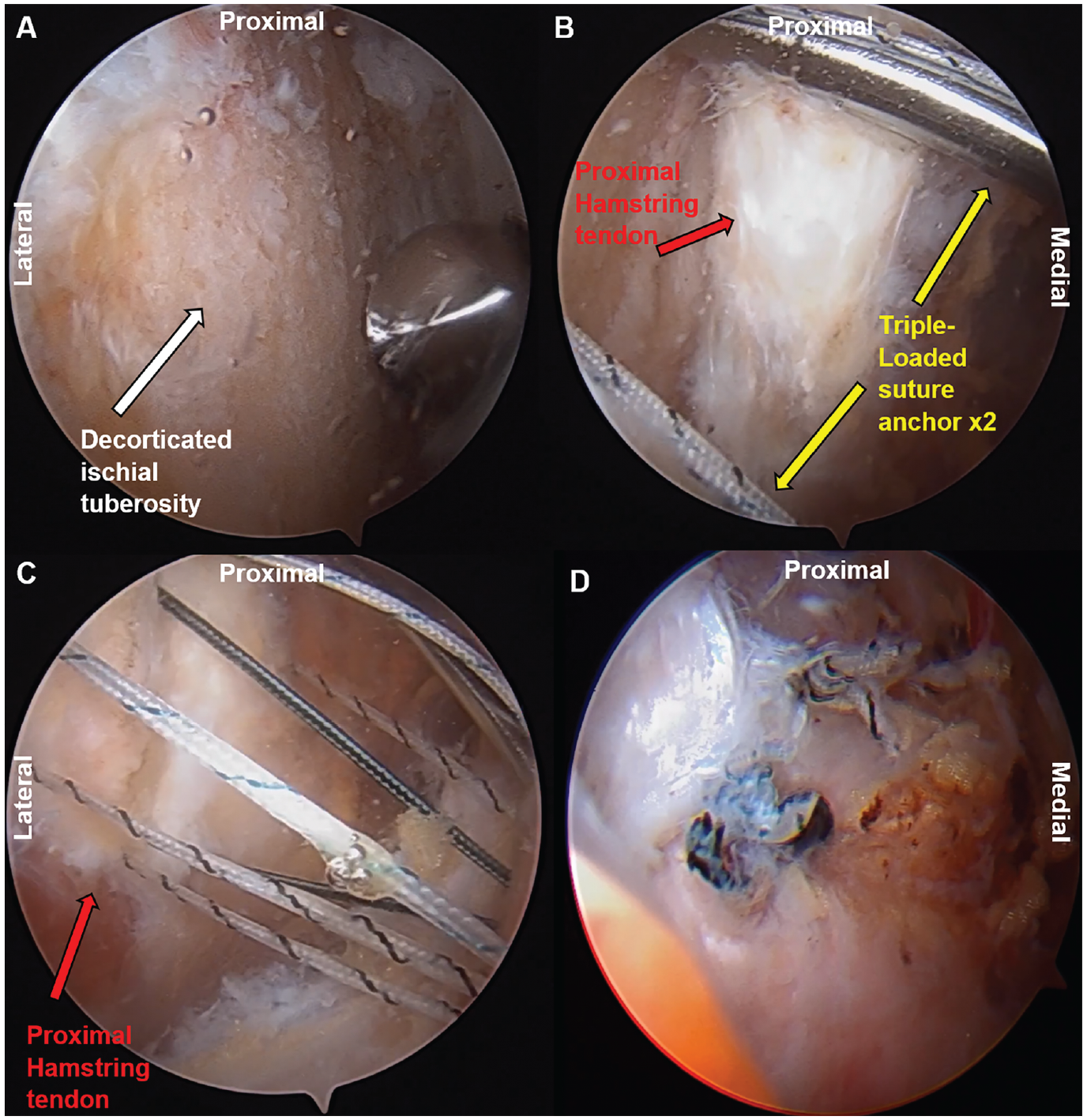
(A) The ischial tuberosity (white arrow) was prepared using a 5.5-mm arthroscopic bur to decorticate the footprint to create a bed of bleeding bone and augment the biologic healing process. (B) Two triple-loaded 5.5-mm AlphaVent anchors (yellow arrows) were placed at the tendon footprint. (C) Suture limbs were passed through the proximal hamstring defect (red arrow) from lateral to medial to avoid iatrogenic injury of the sciatic nerve. (D) Matching suture limbs were tied into a mattress suture configuration for the final anatomic hamstring repair.
Postoperative Rehabilitation
All patients received a postoperative rehabilitation protocol standard to our institution. Briefly, phase 1 rehabilitation (weeks 0-6) was focused on protection of the repaired tendons and avoiding hip flexion and knee extension (hamstring stretch), while patients were placed in a hinged kneed brace locked at 45° using axillary crutches for up to 8 weeks. Of note, for endoscopic repair, formal therapy was deferred until 4 weeks postoperatively whereas therapy was deferred until 6 weeks postoperatively for open repair. Phase 2 rehabilitation (weeks 7-12) was focused on normalizing gait and good lower extremity control with functional movements, while the knee brace was gradually unlocked to 30° of flexion and then to 0°, with gradual progression off crutches and weightbearing as tolerated. Phase 3 rehabilitation (weeks 13-16) was focused on good control and limited pain with sport-/work-specific movement with continued advancing in hamstring strengthening. Finally, phase 4 rehabilitation (weeks 16-24) was focused on continued proper control and no pain with sport-/work-specific movements, with the goal of return to sport/work.
Patient-Reported Outcomes
PROs were collected via secure electronic data collection platforms at ≥5 years postoperatively. PRO measures included the Hip Outcome Score Activities of Daily Living (HOS-ADL) and Sports-Specific (HOS-SS) subscales, 12-Item International Hip Outcome Tool (iHOT-12), and Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function (PF) and Pain domains.
Evaluation of Complications
Postoperative complications including infection (superficial cellulitis, abscess, deep wound infection), neuropathy (persistent posterior thigh/calf pain), deep vein thrombosis, persistent numbness around the incision, and persistent pain with sitting were collected. Additionally, data on all-cause revision surgery during the 5-year postoperative interval were recorded.
Statistical Analysis
Descriptive statistics were reported for patient demographics and characteristics, intraoperative findings, PROs, and postoperative complications. Parametric continuous variables are reported as mean ± SD, while nonparametric variables are reported as medians and interquartile ranges. Categorical variables are reported as counts and percentages. An a priori power analysis was performed to determined power for a subanalysis comparison between open and endoscopic 5-year PROs with a medium effect size (0.5), power of 80%, and alpha level of 0.05. It was determined that 51 patients in both the open and the endoscopic group were necessary to be adequately powered. Therefore, because of the small sample size, the analyses were underpowered to make comparisons between procedure type, chronicity, tear size, or amount of retraction, and statistical comparisons were not performed.
Results
A total of 35 eligible patients (65.7% female; mean age, 52.3 ± 8.4; BMI, 26.3 ± 5.2) were included in the final analysis at a mean follow-up of 69.0 months (range 60.0-95.0 months). Of these, 11 had partial-thickness tears (10 tears of the conjoint tendon, 1 tear of the semimembranosus), and 24 had full-thickness tears. Mean duration from symptom onset to surgical intervention was 37.9 weeks (range, 1.3-306.9 weeks) with 23 patients (65.7%) having chronic preoperative symptoms (Table 2).
Combined Cohort Preoperative Patient Demographics (N = 35) a

Data are reported as mean ± SD or n (%). BMI, body mass index; preop, preoperative.
Of the 35 patients, 23 patients (60.9% female; age, 53.0 ± 9.1 years; BMI, 26.4 ± 4.7 kg/m2) had an open repair approach, and 12 patients (75% female; age, 54.1 ± 5.7 years; BMI, 27.4 ± 6.2 kg/m2) had an endoscopic approach. Of the patients with a full-thickness tear, 6 were treated endoscopically, and 18 were treated open; for partial tears, 8 were treated endoscopically, and 3 were treated via the open approach. Hamstring ruptures in open repair patients were most commonly caused by running (22%), slipping mechanisms during activities of daily living (22%), and water skiing (22%). Similarly, for endoscopic repairs, running (34%) and slipping mechanisms during activities of daily living (34%) were the most common mechanism of injuries. When looking at mechanism of injury by acute versus chronic injuries, the common mechanisms of injury for acute patients were running (41.7%), sports-related (41.7%), and water skiing (16.7%), while the common mechanisms of injury for chronic patients were slipping mechanism during activities of daily living (43.5%) and running (21.7%).
5-Year PROs
The combined cohort had mean 5-year PROs as follows: HOS-ADL, 86.8 ± 12.7; HOS-SS, 83.1 ± 19.5; iHOT-12, 86.3 ± 14.9; PROMIS-PF, 50.0 ± 11.8; and PROMIS–Pain, 50.2 ± 7.9. Additionally, favorable 5-year postoperative PROs were reported for both the open and the endoscopic groups, with equivalent outcomes between the cohorts (Table 3).
Open and Endoscopic 5-year PROs

Data are reported as mean ± SD. HOS, Hip Outcome Score; ADL, Activities of Daily Living; SS, Sports-Specific; iHOT-12, 12-Item International Hip Outcome Tool; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; PF, Physical Function.
Postoperative Complications
Overall, 28.6% (n = 10) of patients had a postoperative complication including persistent peri-incisional numbness (11.4%), wound infection (11.4%), postoperative neuropathy (8.6%), and prolonged sitting pain (2.9%). One patient (2.9%) required a revision proximal hamstring surgery because of a traumatic retear.
Seven (30.4%) patients in the open approach cohort reported postoperative complications and 1 person had a revision at 50.1 months postoperatively (Figure 5). Of the 7 patients reporting complications, 2 patients reported persistent neuropathy (1 posterior thigh, 1 posterior calf pain), 1 patient reported persistent numbness around the incision, 1 patient had both superficial cellulitis and prolonged sitting pain, 1 patient had a deep surgical wound infection that required surgical wound evacuation, and finally, 2 patients had both superficial cellulitis and reported persistent numbness around the incision. Of note, all patients who had a complication had retraction >2 cm (range, 2.5-6 cm). At 5-year follow-up, of the 2 patients who had persistent neuropathy, 1 patient reported that neuropathy had resolved while the other reported no significant change. Of the 3 patients who reported persistent numbness around the incision, 2 patients reported receding numbness while 1 reported no change. Finally, of the single patient with prolonged sitting pain, the patient reported no significant change.

Open and endoscopic postoperative complications and revisions.
Of the patients who underwent endoscopic treatment, 2 (16.7%) patients reported postoperative complications (Figure 5). One patient reported persistent neuropathy (posterior thigh/calf pain) and the other reported persistent incisional numbness. No patients in the endoscopic cohort required a revision surgery. At 5-year follow-up, both patients with persistent neuropathy and incisional numbness reported that the complication had receded but not resolved completely.
Acute Versus Chronic Symptoms
Equivalent scores in all measured PROs were demonstrated between both time points (acute and chronic), as well as between procedure type, although statistical comparisons were not made because of limited sample size (Figure 6).
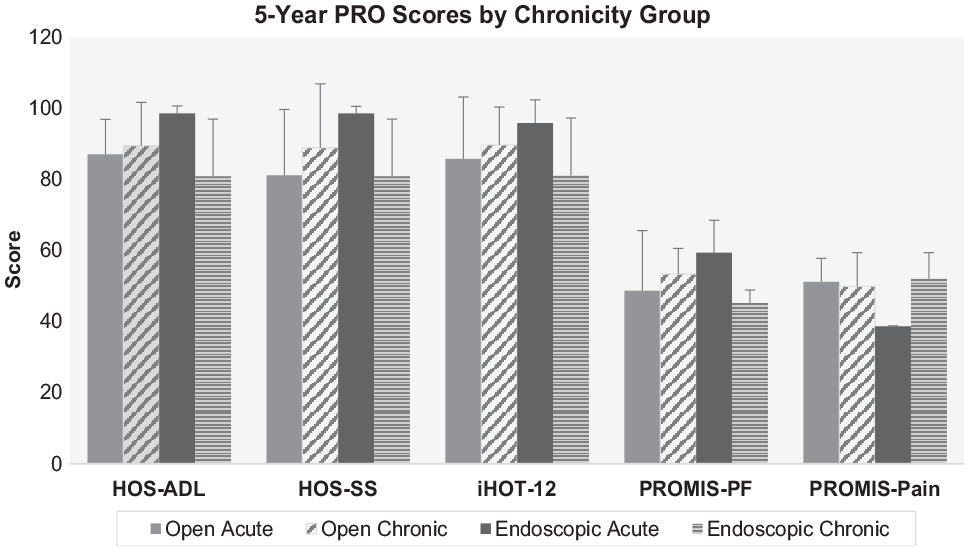
Open and endoscopic 5-year patient-reported outcomes (PROs) stratified by chronicity group (acute vs chronic). Error bars indicate standard deviations. HOS-ADL, Hip Outcome Score Activities of Daily Living subscale; HOS-SS, Hip Outcome Score Sports-Specific subscale; iHOT-12, 12-Item International Hip Outcome Tool; PROMIS, Patient-Reported Outcomes Measurement Information System for Physical Function (PF) and Pain subscales.
When looking at complication rates between the stratified cohorts, the open acute (n = 10) group had 2 patients with postoperative complications (1 patient with numbness around the incision, 1 patient with deep surgical infection/prolonged sitting pain), while the open chronic (n = 13) group had 5 patients with postoperative complications (2 patients with neuropathy, 2 patients with superficial cellulitis/numbness around incision, 1 with deep wound infection) as well as the 1 revision case. The endoscopic acute (n = 2) group had no postoperative complications, while the endoscopic chronic (n = 10) group had both (n = 2) patients with the postoperative complications (1 patient with persistent neuropathy, 1 patient with numbness around incision).
Partial- Versus Full-Thickness Tears
Equivalent scores in all measured PROs were demonstrated between both partial- and full-thickness tears of both procedure type, although statistical comparisons were not made because of limited sample size (Figure 7).

Open and endoscopic 5-year patient-reported outcomes (PROs) stratified by tear size (partial vs full). Error bars indicate SDs. HOS-ADL, Hip Outcome Score Activities of Daily Living subscale; HOS-SS, Hip Outcome Score Sports-Specific subscale; iHOT-12, 12-Item International Hip Outcome Tool; PROMIS, Patient-Reported Outcomes Measurement Information System for Physical Function (PF) and Pain subscales.
The open partial-thickness (n = 3) cohort had 1 patient with postoperative complications (neuropathy), and the open full-thickness (n = 20) group had the 6 remaining complications and the 1 revision case. The endoscopic partial-thickness (n = 8) cohort reported 1 complication (neuropathy), and the endoscopic full-thickness (n = 4) group reported the other complication (incisional numbness).
Discussion
Proximal hamstring injuries comprise a substantial source of sport-related injuries to the lower extremities of active individuals. Advancements in surgical techniques have resulted in expanded clinical indications for operative management, with good clinical outcomes in short-term patient outcomes. The present study is the first to demonstrate that proximal hamstring conditions treated through both open and endoscopic surgical techniques provide excellent clinical outcomes that extend to ≥5 years postoperatively.
The present series provides evidence that the favorable outcomes achieved at short-term follow-up remain durable to a minimum of 5 years postoperatively. Results of this study build upon prior work evaluating clinical outcomes associated with proximal hamstring repair. In 2011, a cohort of 23 patients were reviewed at minimum 1-year follow-up who underwent open surgical repair for full-thickness proximal hamstring ruptures of varying acuity. 5 The authors identified a 91% return-to-sport rate with near-full restoration of isokinetic hamstring strength. Posterior thigh numbness was reported in 61% of patients and neuropraxic symptoms were reported in 17% of patients. In a cohort of 30 patients who underwent endoscopic repair and followed for ≥2 years, the authors reported that 80% of patients achieved a Patient Acceptable Symptom State, with a complication rate of 3%. 14 Similarly, a multicenter study reported high scores on the iHOT-12 and modified Hip Harris Score in a heterogeneous cohort of 50 patients with full-thickness and partial-thickness tears treated via both open and endoscopic techniques and a ≥2-year follow-up. 17 Finally, at a mean follow-up of 27.2 ± 22.9 months, patients reported a significant increase in Tegner activity level score and high rate of return to sport at the same level (79.4%) at final follow-up. 16
In this series, outcomes after both endoscopic and open surgical repair were included, by design, to illustrate the favorable outcomes achieved across a spectrum of proximal hamstring injuries and different procedures with a follow-up duration greater than that previously reported. While subsequent work is necessary to parse out tear characteristics that predispose to more or less favorable outcomes with a particular surgical treatment (eg, open or endoscopic approach), the present study provides a generalized benchmark to inform patients and providers of longer-term follow-up data. Inclusion of outcome data for both open and endoscopic techniques tempts a direct comparison between techniques. However, beyond the insufficient sample size to detect differences between these groups, endoscopic and open surgeries are employed for distinct patient pathologies within the treating surgeon’s clinical practice. Within this cohort, open repair was performed on 7 cases in which tendon retraction exceeded 5 cm. Currently, such cases are not performed endoscopically in the senior author’s treatment algorithm. Taken together, endoscopic and open surgical techniques may be considered complementary surgical tools in contemporary proximal hamstring repair.
Distinct indications for endoscopic and open approaches are predicated, in part, on existing limitations associated with endoscopic techniques. For example, open tendon repair commonly uses a Krackow suture–based construct to maximize security at the suture-tendon interface. Accordingly, biomechanical studies of proximal hamstring repair have employed Krackow suturing in their experiments as the gold standard. However, contemporary endoscopic approaches typically use mattress-based suture configurations, such as single- and double-row constructs.18,22 This has caused some providers to reserve endoscopic approaches for only partially torn tendons, or those with minimal retraction, because of concern for an ability to achieve a durable repair construct. Recent evidence has begun comparing what is achievable in terms of repair strength between endoscopic and open approaches, with comparable results. 20 As both implant technology and surgical techniques improve, indications for endoscopic repair are likely to expand. Although the endoscopic approach has theoretical advantages for lower complications, as previously stated, a complication rate of 16.7% (n = 2 patients) was still demonstrated in this study. Further studies with greater patient numbers are needed to make statistical comparisons of complication rates between open and endoscopic surgical approaches.
Limitations
As the study was designed to report on a convenience sample of patients with longer follow-up than that previously reported in the literature, the sample size was insufficient to perform subgroup comparisons based upon tear type (full thickness vs partial thickness), chronicity (symptom duration >4 weeks or <4 weeks), or surgical intervention (open vs endoscopic). The heterogeneity within our patient cohort is consistent with prior published case series and highlights the generalizability of favorable outcomes conferred by surgical treatment for various clinical circumstances. Nonetheless, further investigations are needed to stratify long-term clinical outcomes based on aforementioned clinical characteristics and treatment approaches. Additionally, our study did not include a nonoperative control group for comparisons of long-term outcomes. Further investigations focused on long-term results of operative versus nonoperative management are needed to determine the adequacy of surgical intervention. Moreover, return to sport and functional/strength testing was not performed in this study, as these metrics may be indicators of durability and return to function after surgical intervention. Finally, all procedures were performed by a fellowship-trained sports medicine surgeon with extensive experience in hip arthroscopic and endoscopic techniques, and thus, the study’s results may not be generalizable to patients treated by surgeons with varying degrees of experience and/or technical expertise.
Conclusion
Both open and endoscopic surgical techniques for repair of proximal hamstring injuries produce favorable patient-reported clinical outcomes at a minimum 5-year follow-up.
Footnotes
Final revision submitted May 20, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received consulting fees from Stryker, Springer, and Ossur; royalties from Stryker, Ossur, and Springer; research support from Allosource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, Stryker, and Springer; and education payments from Elite Orthopaedics and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (No. 12022108-IRB01-CR10).