
Abstract
Background:
Several techniques have been used by surgeons for anatomic tibial tunnel placement in anterior cruciate ligament (ACL) reconstruction, including the ACL stump positioning (ASP) technique and the tibial spine positioning (TSP) technique.
Purpose/Hypothesis:
The purpose of this study was to evaluate whether bony landmarks (medial and lateral tibial spine [MLTS]) can be a reliable reference for improving the accuracy of tibial tunnel placement in anatomic single-bundle ACL reconstruction compared with the ACL stump. It was hypothesized that the MLTS would not be a reliable bony landmark for tibial tunnel placement.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The 3-dimensional computed tomography images of 111 patients who underwent ACL reconstruction between 2020 and 2021 were included in this study. For tibial tunnel placement, the ASP technique was used in 49 patients, and the TSP technique was used in 62 patients. The 3-dimensional computed tomography images were reconstructed to enable measurements of the locations of the MLTS and tunnel center based on a grid method. Statistical analysis was conducted to compare the MLTS location and tibial tunnel position as well as the accuracy (mean distance of each actual location from the anatomic center) and precision (standard deviation of the accuracy, indicating the reproducibility of the tunnel position) of the tunnel position between the ASP and TSP groups.
Results:
Significant differences were observed between the ASP and TSP groups in terms of the tibial tunnel position on the mediolateral axis (46.7% ± 2.0% vs 45.9% ± 2.2%, respectively; P = .034), while no significant differences were found in terms of the accuracy (4.1% vs 4.6%, respectively; P = .259) or precision (2.1% vs 2.1%, respectively; P = .259) of tibial tunnel positioning between the 2 groups.
Conclusion:
In anatomic single-bundle ACL reconstruction, the use of the MLTS for tibial tunnel placement achieved comparable accuracy and precision compared with the use of ACL remnants, supporting its role as a reliable bony landmark in tibial tunnel positioning.
Keywords
Currently, there are several surgical techniques used for anatomic single-bundle anterior cruciate ligament (ACL) reconstruction, and 2 common methods are classified by whether ACL remnants are preserved: the remnant-preserving technique and the non–remnant-preserving technique. 4 Correct graft placement is critical in anatomic ACL reconstruction because it plays an important role in preventing intra-articular impingement and restoring the stability and kinematics of the knee joint. 18 Some clinical studies have demonstrated that anatomic ACL reconstruction can achieve better postoperative knee outcomes than the traditional isometric technique by reducing the possibility of graft failure, pain, and early osteoarthritis.3,20 Anatomic ACL reconstruction requires comprehensive knowledge of the ACL attachments to allow for accurate tunnel positioning. 2 To guide surgeons during reaming of the tibial tunnel and avoid intraoperative damage to the anterior root of the lateral meniscus (ARLM), several landmarks have been used by surgeons in ACL reconstruction for anatomic tibial tunnel placement, including the ACL stump, the posterior border of the ARLM, the posterior cruciate ligament (PCL), and the medial tibial spine, which has been shown to be a valid and reliable reference.2,22,31
In the current study, we categorized ACL reconstruction procedures according to the landmark chosen by the surgeon: the ACL stump positioning (ASP) technique and the tibial spine positioning (TSP) technique. Arthroscopic knee surgery with the TSP technique, in which the torn ACL is resected, provides complete visibility of the tibial spine. 5 A previous study has shown that the location of the medial and lateral tibial spine (MLTS) can affect the judgment of surgeons in determining tibial tunnel placement when applying the transportal technique in anatomic single-bundle ACL reconstruction, which may lead to tunnel misplacement. 5 However, Dimitriou et al 2 reported that both the ARLM and medial tibial spine might be reliable landmarks for an anatomic tunnel, especially in cases of revision in which the ACL stump on the tibial side is not available. Whether the medial tibial spine can be a reliable bony landmark in ACL reconstruction is still a matter of debate. With the ASP technique, even if more than 25% of the residual graft remains, different types of tears may still make the tibial spine visible. To date, no placement of the tibial tunnel by referencing the MLTS has been reported, and no study has compared the accuracy and precision of this surgical technique versus the ASP technique. Therefore, whether the MLTS can be a reliable bony landmark and whether it can affect the accuracy and precision of tibial tunnel placement in comparison to the ASP technique remain unknown.
The purpose of this study was to compare the accuracy and precision of tibial tunnel placement using the TSP technique with those of the ASP technique. It was hypothesized that using the MLTS as a reference in ACL reconstruction would not be as accurate as using ACL remnants for tibial tunnel positioning.
Methods
Study Design and Patient Selection
This single-center, retrospective case-control study received institutional review board approval, and all included patients provided informed consent to participate. A retrospective analysis was conducted based on predefined inclusion and exclusion criteria. Included were patients with a recent (<3 months) isolated ACL tear who underwent anatomic single-bundle ACL reconstruction between 2020 and 2021 and underwent 3-dimensional computed tomography (3D-CT) after surgery according to routine practice. Exclusion criteria were (1) age <18 or >50 years, (2) multiligamentous injuries, (3) delayed surgery exceeding 3 months, (4) revision ACL surgery, and (5) low-quality 3D-CT images. The choice of the ASP or TSP technique depended on the length of the ACL remnant, which was determined arthroscopically at the time of surgery. All surgical procedures were performed according to a pre-established protocol and were recorded.
Surgical Procedure
All patients underwent anatomic single-bundle ACL reconstruction using a hamstring or quadriceps tendon autograft within 3 months after the ACL injury, and operative procedures were arthroscopically conducted by the same surgeon (S. G.). At the beginning of the procedure, normal anteromedial and anterolateral portals were used to assess the intra-articular condition, and all knees were determined to have a complete ACL tear and fresh ACL remnants. The choice of a surgical protocol depended on the intraoperative findings of the length of ACL remnants as measured by the chief surgeon (S. G.) and the attending physician (Y. Xiong) using a tunnel gauge (Acufex; Smith & Nephew). The ASP technique was performed only if both investigators agreed that the length of ACL remnants was over 25% compared with the original length of the intact ACL and that the ACL remnants had no partial disruption at the tibial attachment site. This determination method was consistent with previous research carried out for evaluating the tibial tunnel. 11 If the length of the ACL remnants was under 25% or if the tibial attachments were disrupted, the remnants were debrided using an arthroscopic shaver or a radiofrequency probe (Smith & Nephew) to mark the tibial tunnel position for good visualization of the MLTS, and the TSP technique was performed.
For the ASP group, tibial tunnel placement was mainly determined by the morphology of the ACL remnants. An ACL guide pin (Acufex) was placed in the center of the ACL stump, and the position of the pin was confirmed by referencing several landmarks, including the anterior edge and medial and lateral borders of the residual ACL as well as the PCL and the ARLM. Subsequently, the tibial tunnel was drilled using an appropriately sized reamer. For the TSP group, the remnants on the tibial side were confirmed to be less than 25%. The method for locating the tibial tunnel with the TSP technique involves the surgeon estimating, under direct visualization, a point approximately one-third of the distance along a line connecting the medial and lateral tibial eminences and then locating the tibial tunnel around 15 mm anteriorly along a perpendicular line extending from this point. Surgeons primarily relied on the MLTS as an anatomic landmark, while also taking into account the ARLM and PCL, under clear arthroscopic visualization, based on their surgical expertise (Figure 1). A guide pin was placed according to the positioning method mentioned above under direct visualization (through a standard anteromedial portal) with the guide and then drilled with an appropriately sized reamer. In both groups, tibial fixation of the graft was accomplished by an interference screw (Biosure PK; Smith & Nephew).
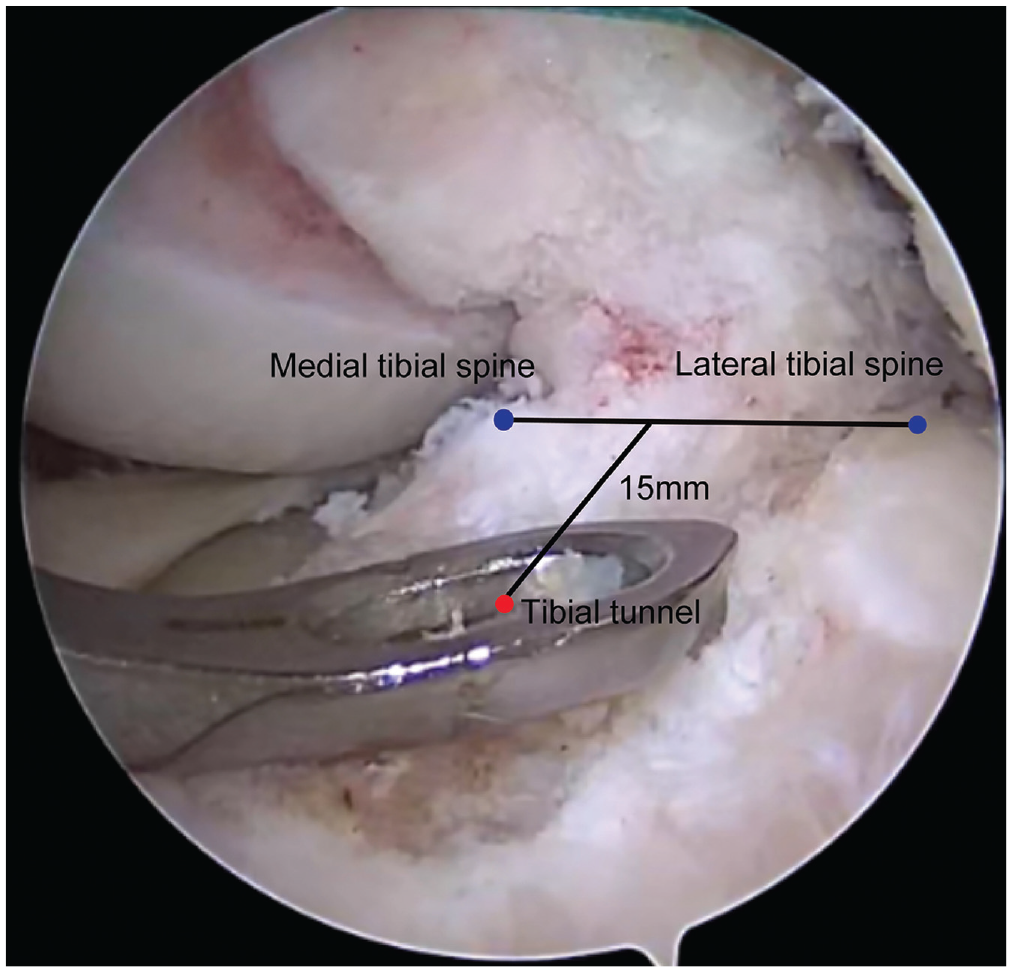
Positioning method demonstrated in an arthroscopic view using the tibial spine positioning technique.
Image Processing and Tunnel Position Measurement
All included patients underwent 3D-CT (LightSpeed 4-slice scanner; GE) at 2 or 3 days postoperatively, and the images were collected through a spiral sequence with 0.625-mm cuts. Imaging data, which were retrieved from a picture archiving and communication system by a single technician (Y.W., who was blinded to the surgical technique), were reconstructed by a digital orthopaedic technician (X.W., who was blinded to the surgical technique) using Mimics Medical software (Version 21.0; Materialise) to create a 3D model for each patient's proximal tibia. All of the reconstructed 3D models were measured by 2 observers (S.K. and C.S.), who were blinded to the surgical technique, using 3-matic Medical (Version 13.0; Materialise), a software application supporting 6 degrees of freedom model positioning as well as 3D model cutting and modification. The reconstructed 3D model of the tibia of each patient was then rotated to a “strictly top view position” by utilizing the fit plane tool in this software. The top view of the proximal tibia was considered satisfactory when the visual axis was perpendicular to the plane of the medial tibial articular margin. This method has been detailed in the study by Lertwanich et al. 15
A grid system 15 was positioned parallel to the posterior condyles of the tibia and sized to include the maximum dimensions of the plateau. This system was used to measure the MLTS and tunnel location, which were recorded from the center of the aperture of the tunnel to the maximum extents of the grid, expressed as percentages of the total grid dimensions along the anteroposterior (AP) axis (B1/B2 in Figure 2) and mediolateral (ML) axis (A1/A2 in Figure 2). The ML axis was defined as a line between the most posterior margin of the medial and lateral tibial condyles. The anterior transverse line was defined as a line parallel to the ML axis and touching the most anterior margin of the tibial plateau. The AP axis was defined as a line perpendicular to the transverse line and touching the medial edge of the tibial plateau. As the tunnel aperture is usually elliptical (because of the obliquity of drilling), the tunnel center was determined by the intersection of 2 vertical lines corresponding to the maximum dimensions of the aperture. 11 To determine the location of the tibial spine, the distances from the AP axis and the ML axis to the top of the tibial spine were measured as well. The location of the anatomic center (AC) was acquired from previously published 3D-CT data of cadaveric specimens (38.7% [AP] and 49.1% [ML]) to define the AC of the ACL tibial footprint.11,15 To evaluate the measurement variability, we also made reference to the standard deviation documented in the anatomical study of Lertwanich et al, which was reported as 11.1% along the AP axis and 3.2% in the ML axis. 15 The measurement was kept to 1 decimal place, and so was the expression of the results. The accuracy (the mean distance of each actual location from the AC) and precision (the standard deviation of the accuracy, indicating the reproducibility of the tunnel position) of tibial tunnel positioning were calculated by applying the percentage grid system and using the Pythagorean theorem (C = √ [A2+B2] in Figure 2). This method was in reference to Iriuchishima and Goto’s 5 research and has been proven to be reliable and valid in previous studies.10,11
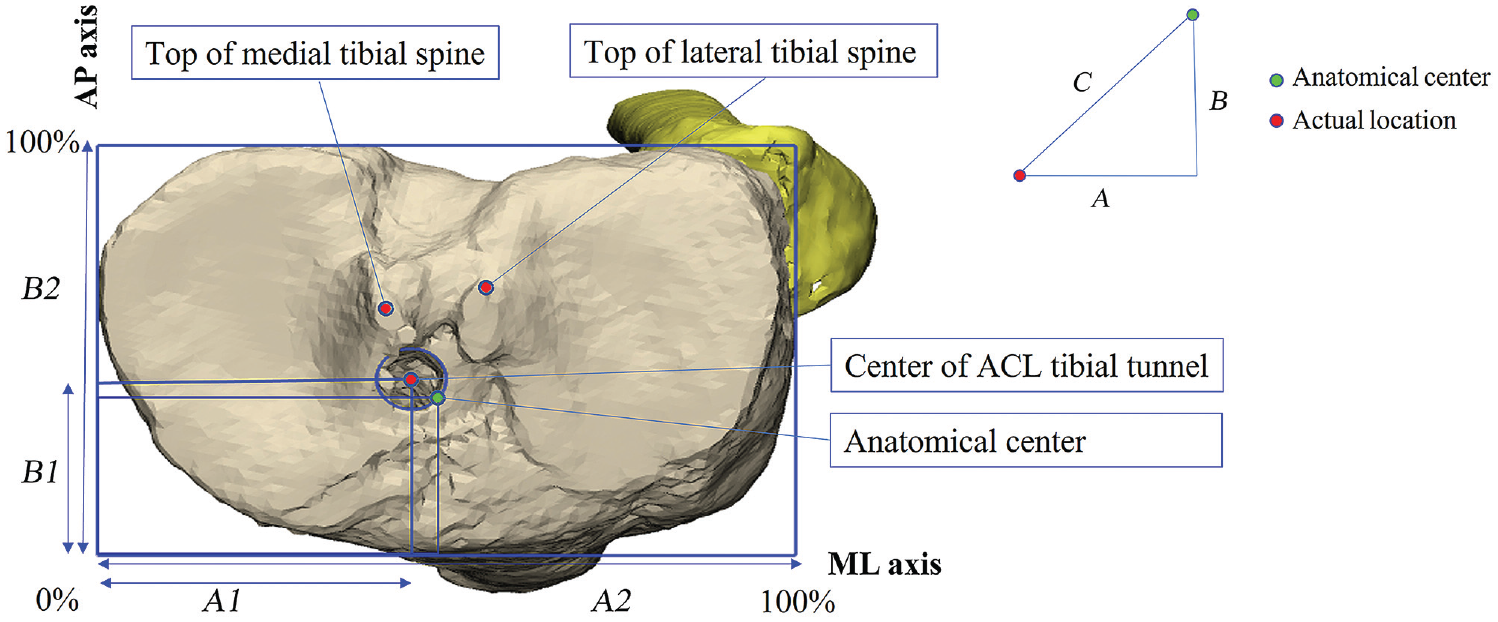
Three-dimensional computed tomography measurements using a conventional anteroposterior (AP) and mediolateral (ML) grid system. The tibial tunnel position and location of the tibial spine were measured (AP = B1/B2; ML = A1/A2) in the “strictly top view position” of the tibial plateau. The medial and anterior margins of the tibial plateau were regarded as 0%, and the lateral and posterior margins were regarded as 100%. Accuracy distance: C = √ (A2+B2). ACL, anterior cruciate ligament.
The 2 observers evaluated the tunnel position and MLTS location independently, and all the measurements were performed twice within 3 weeks so that intraobserver and interobserver reliability could be calculated. The mean value was used in the final analysis.
Statistical Analysis
Intraobserver and interobserver reliability of the measurements were calculated with the intraclass correlation coefficient (ICC). All data are reported as the mean ± standard deviation. For continuous data, the Kolmogorov-Smirnov test was used to analyze normal distributions. The demographic data were compared between the ASP and TSP groups, with the independent-samples t test for continuous variables or the chi-square test for dichotomous variables. SPSS (Version 26.0; IBM) was used for statistical analysis, with P < .05 defined as statistical significance.
The sample size was calculated using G*Power (Version 3.1, Heinrich-Heine-Universität Düsseldorf, http://www.gpower.hhu.de/) based on the results of a preliminary study. The alpha and beta values were set to .05 and 0.20, respectively, and the calculated sample size was 98 (49 in each group).
Results
Of the 132 patients who were initially assessed, 111 patients (49 patients in the ASP group and 62 patients in the TSP group) were ultimately included. Figure 3 shows the flowchart of patient inclusion, and Table 1 shows the characteristics of the ASP and TSP groups.
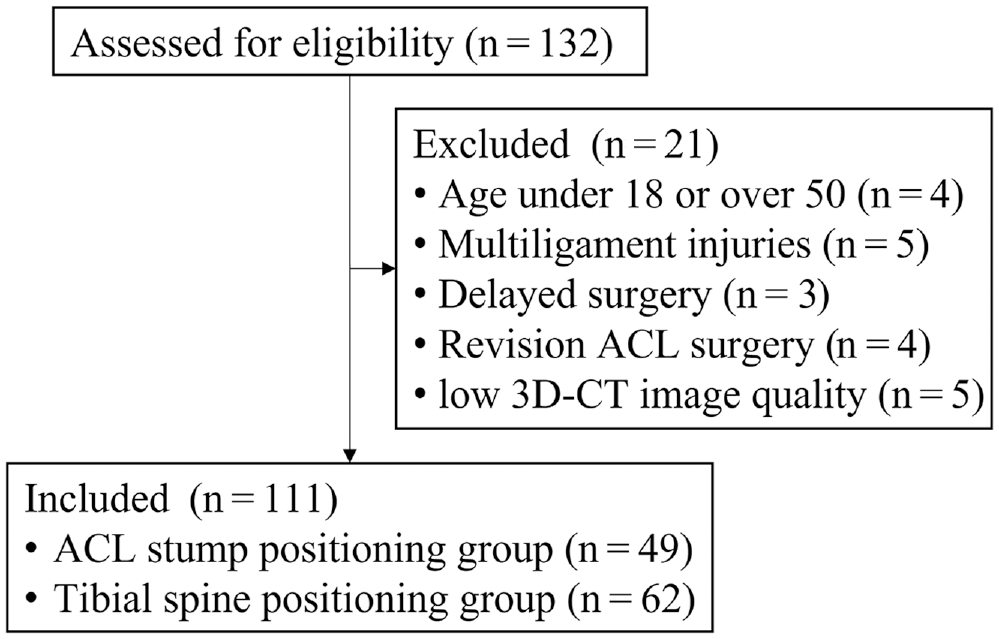
Patient flowchart. 3D-CT, 3-dimensional computed tomography; ACL, anterior cruciate ligament.
Patient Characteristics (N = 111) a

Data are reported as percentage or median (interquartile range). Boldface P value indicates a statistically significant difference between groups (P < .05). ASP, anterior cruciate ligament stump positioning; TSP, tibial spine positioning.
Interobserver and Intraobserver Reliability
Table 2 presents a summary of the interobserver and intraobserver ICCs. For measurements of the tibial tunnel position and the MLTS location, the intraobserver ICC was 0.965 (observer 1) and 0.974 (observer 2), and the interobserver ICC was 0.891, indicating excellent reliability.
Interobserver and Intraobserver Reliability of Measurements a

Data are reported as intraclass correlation coefficient (95% CI). ASP, anterior cruciate ligament stump positioning; TSP, tibial spine positioning.
MLTS Location and Tibial Tunnel Position
No difference was found between the ASP and TSP groups in the location of the MLTS (medial tibial spine [ML: P = .488; AP: P = .054] and lateral tibial spine [ML: P = .773; AP: P = .451]). The tibial tunnel position in the TSP group was, on average, 0.8% more medial compared with the ASP group (P = .034). However, no difference was found in the AP axis (P = .227). No differences in the accuracy (distance from the AC: 4.1% vs 4.6%, respectively; P = .259) and precision (2.1% vs 2.1%, respectively; P = .259) of the tibial tunnel position were found between the ASP and TSP groups (Table 3). The individual tibial tunnel positions and MLTS locations are graphically demonstrated in a scatterplot (Figure 4A) and a scatterplot with the grid method (Figure 4B).10,11 Additionally, the location of the MLTS was found to be relatively fixed, as shown in Figure 5.
MLTS Location and Tibial Tunnel Position a

Data are reported as mean ± SD (95% CI) unless otherwise indicated. Boldface P value indicates a statistically significant difference between groups (P < .05). AP, anteroposterior; ASP, anterior cruciate ligament stump positioning; ML, mediolateral; MLTS, medial and lateral tibial spine; TSP, tibial spine positioning.
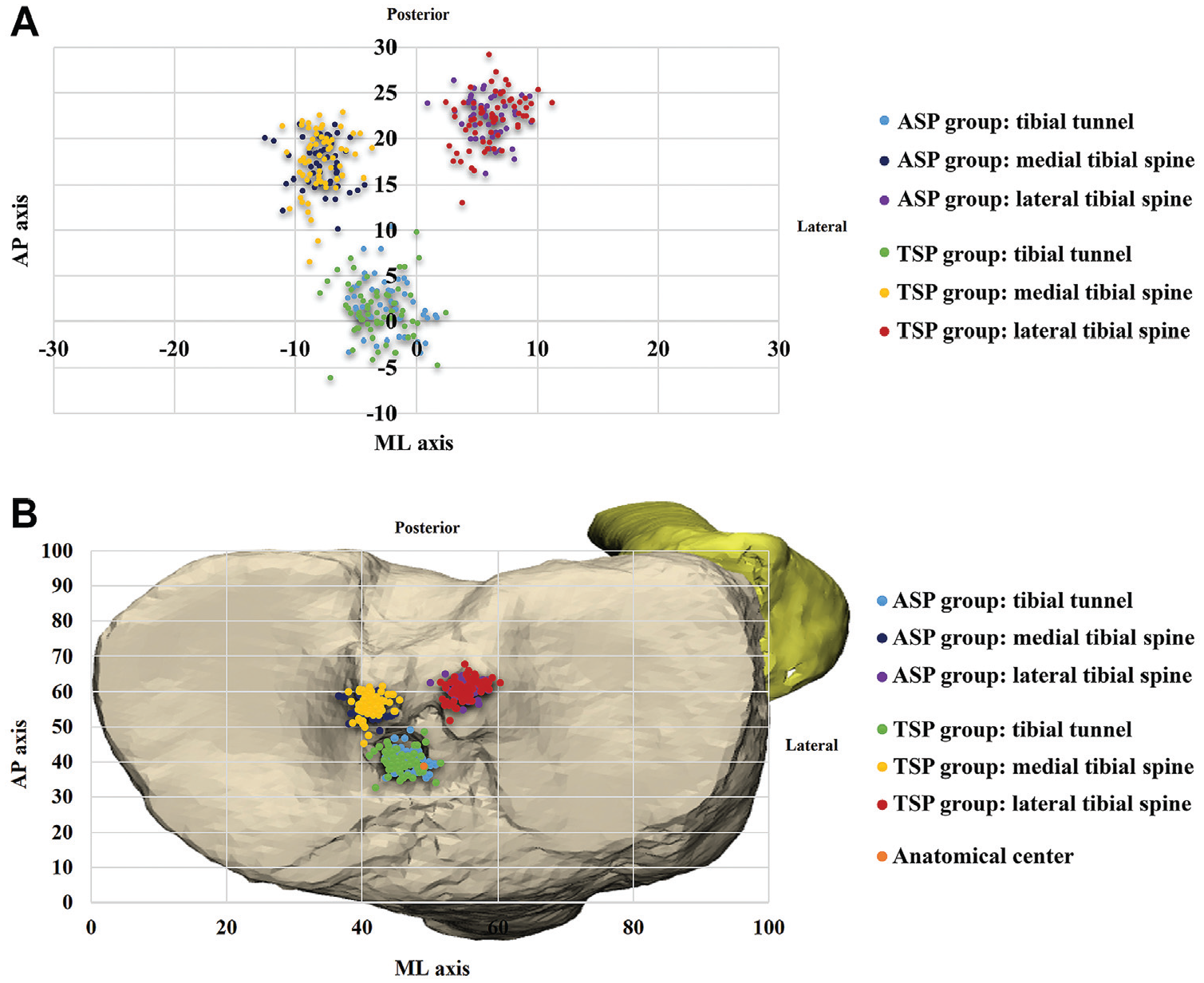
(A) Scatterplot demonstrating the individual tibial tunnel and medial and lateral tibial spine (MLTS) locations as a percentage of the distance from the anatomic center along the anteroposterior (AP) and mediolateral (ML) axes. (B) Scatterplot of the grid in the “strictly top view position” of the tibial plateau showing the anatomic center and mean tibial tunnel and MLTS locations in the anterior cruciate ligament stump positioning (ASP) and tibial spine positioning (TSP) groups. Measurements are shown as a percentage of overall dimensions along the AP and ML axes.
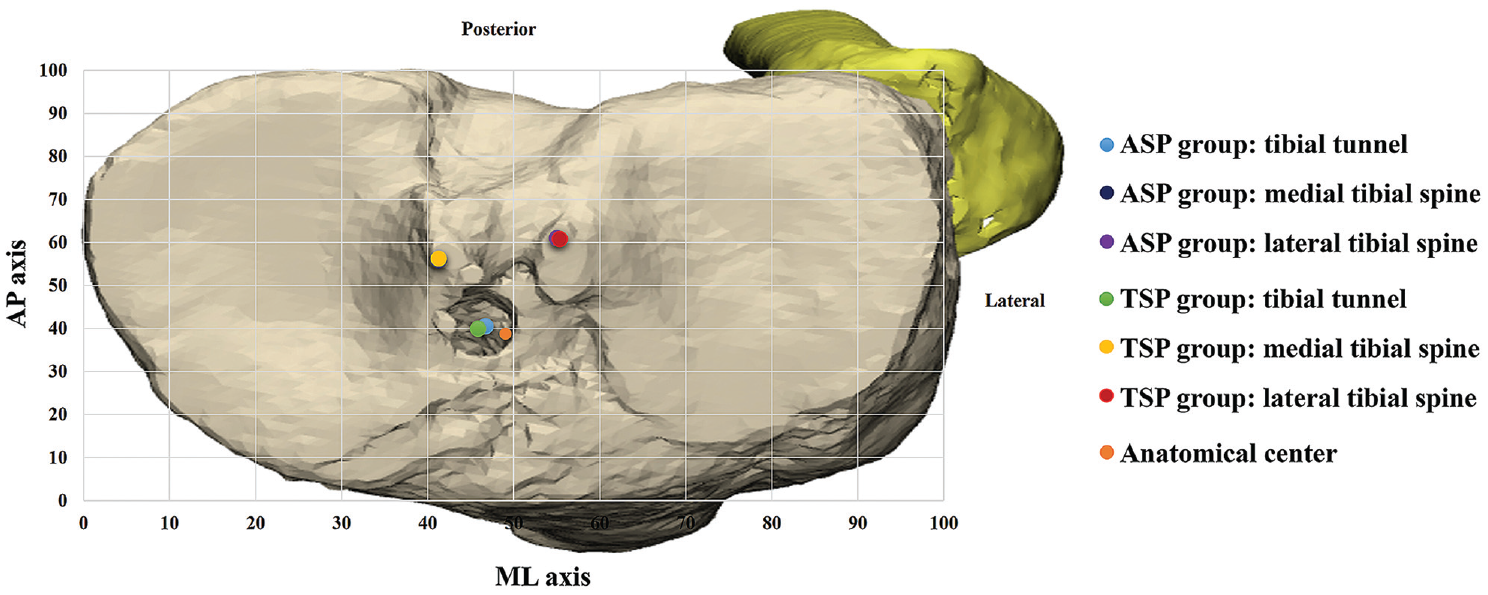
The grid showing the anatomic center and mean tibial tunnel and medial and lateral tibial spine locations in the anterior cruciate ligament stump positioning (ASP) and tibial spine positioning (TSP) groups. Measurements are shown as a percentage of overall dimensions along the anteroposterior (AP) and mediolateral (ML) axes.
Discussion
The most important finding of this study was that the 2 surgical techniques did not produce any difference in the accuracy and precision of tibial tunnel positioning, indicating that the MLTS is a reliable bony landmark for tibial tunnel placement in ACL reconstruction. A significant difference was found in the placement of the tibial tunnel on the ML axis. However, this small discrepancy (<1%) likely does not have a significant clinical impact. These findings indicate that surgeons can position the tibial tunnel by referencing the MLTS.
Few studies have evaluated the relationship between the ACL footprint and the morphology of the tibial spine. It has been widely accepted that the ACL footprint is attached to the tibial spine.6,12,16,19,23 Oka et al, 19 based on a histological evaluation of the ACL footprint, reported that the medial margin of the ACL footprint was attached to the anterior part of the medial tibial spine and that the lateral tibial spine was located far from the ACL footprint. Tensho et al 27 performed a 3D-CT evaluation of the ACL footprint and reached the same conclusion that some ACL fibers were attached to the medial tibial spine while no ligamentous tissue was found to be attached to the lateral tibial spine. Our study showed that even though the lateral tibial spine was visible in the ASP group, it did not affect the surgeon's positioning when performing the ASP technique.
Tunnel malpositioning in ACL reconstruction is a major cause of graft failure. 28 Anatomic positioning of the graft during ACL reconstruction plays an important role in restoring stability, preventing impingement, and lowering the risk of graft failure.13,21 In anatomic ACL reconstruction, the tibial tunnel should be placed within the ACL footprint. The tibial spine can be regarded as a bony landmark for tibial tunnel positioning. 2 A previous study investigated the correlation between the location of the tibial spine and the ACL footprint morphology with the TSP technique, and the results indicated that the location of the tibial spine was likely to influence tibial tunnel placement. 5 Both techniques positioned the tibial tunnel medially in comparison to the anatomic site. Therefore, considering the requirement for an anatomically correct position, the surgeon should adjust the guide pin slightly more laterally when utilizing either of these positioning techniques.
By comparatively analyzing the magnetic resonance imaging scans of an ACL-ruptured group and an ACL-intact group, Dimitriou et al 2 found that the medial tibial ridge and ARLM might be used as reliable landmarks for anatomic ACL reconstruction. In the present study, it was found that the location of the MLTS did not differ between the 2 groups, suggesting that the MLTS is a reliable anatomic landmark for tibial tunnel placement, with little variation between patients (Table 3). Iriuchishima and Goto 5 argued that the MLTS could unintentionally affect the judgment of surgeons in determining the tibial tunnel position and might result in tunnel misplacement. In contrast, our study showed that the tibial spine had no influence on the accuracy and precision of tibial tunnel positioning in the TSP group. With the ASP technique, the medial tibial spine is covered by ACL fibers, which means that surgeons mainly reference ACL remnants and other landmarks such as the posterior border of the ARLM and PCL for tibial tunnel placement.8,19,22 Additionally, the ASP technique has shown benefits in retaining proprioceptors on the synovium of residual ligamentous tissue, accelerating the recovery of neuromuscular control and knee function,1,7 maintaining the stability of the knee joint and decreasing the mechanical load on the graft,9,14,25 and hastening biological healing of the graft by enhancing cell proliferation and revascularization .24-26,29 Moreover, owing to the presence of functional cells in the remnants, tunnel widening, which is thought to result from synovial fluid egress, can be prevented.17,30
Both techniques showed a standard deviation less than what was reported by anatomic studies (AP: ASP = 2.9%, TSP = 3.0%, anatomic = 11.1%; ML: ASP = 2.0%, TSP = 2.2%, anatomic = 3.2%), implying that they can reflect the natural variation among individual patients without increasing the deviation in positioning. 15 This comparison method was in reference to the study of Kosy et al. 11 Although significant differences were detected in the tibial tunnel position on the ML axis, this effect cannot be converted to a clinical impact, as we found no differences between the 2 surgical techniques in terms of the accuracy and precision of tibial tunnel positioning. In general, our results were consistent with the conclusion of Dimitriou et al 2 that the medial tibial spine might be a reliable landmark for identifying the center of the ACL footprint. Our new findings were that the tibial spine had no influence on the accuracy and precision of tibial tunnel positioning compared with the ASP technique and that the MLTS might be a reliable landmark for positioning the anatomic tibial tunnel with the TSP technique. In addition, both surgical techniques produced accurate and precise tibial tunnels. The MLTS specifically aided in achieving proper ML placement of the tibial tunnel. However, it is important to note that the surgeon must rely on other anatomic structures to determine the AP position of the guide pin.
The findings of our study suggest that surgeons can place the tibial tunnel accurately and precisely by either referencing the MLTS with the TSP technique or by referencing ACL remnants with the ASP technique. The TSP technique can be useful in chronic cases and perhaps in revision cases. Although evidence supports that the TSP technique allows for accurate and precise tibial tunnel positioning, individual anatomic variability in the MLTS location cannot be ignored, and the position of the tibial spine must be carefully determined with the TSP technique to avoid tibial tunnel misplacement.
Limitations
The main limitations of this study were as follows. (1) As a retrospectively designed study, our results may be less robust than those of randomized research. However, in view of standardized CT scanning, the reconstruction and measurement protocols followed by the researchers, and the standardized surgical and documentation procedures followed by the surgeon, the data in this study were sufficient and reliable. (2) Our results were confined to the clinical experience of a single center and even a single surgeon, and that likely contributed to the accuracy and precision (especially in the AP direction), which were subjected to limited external validity. However, single-center studies usually have more standardized CT images and higher measurement reliability compared with multicenter studies. Moreover, because all operative procedures were performed by the same surgeon, the potential impact imposed by the differences in surgical technique could be well avoided. Nonetheless, future multicenter prospective studies with appropriate grading of surgeons’ proficiency are still needed to find out whether general surgeons can safely perform the TSP technique. (3) The ACL stump fiber length in our study was manually measured by the chief surgeon and the attending physician, and the results were subjected to an error of 0 to 10 mm because of the precision of measurements. (4) The apex position of the tibial spine in reconstructed 3D-CT images could not accurately represent the actual anatomic position, and there was even a bias in the selection of the apex position. To solve this problem, each measurement was repeated twice by 2 independent authors, and ICC analysis was performed, which indicated excellent reliability. (5) Only ethnically Chinese patients were included in this study, and future studies should control for the variable of ethnicity.
Conclusion
The MLTS served as a reliable anatomic landmark for positioning of the tibial tunnel during ACL reconstruction, as it enabled the placement of an accurate tunnel similar to that referencing the ACL stump. In anatomic single-bundle ACL reconstruction, both the ASP and TSP techniques achieved reproducible accurate tibial tunnels.
Footnotes
Final revision submitted May 26, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University (2021KFJJ06); the Hunan Provincial Natural Science Foundation of China (2021JJ30040); and the High Performance Computing Center, Central South University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Xiangya Hospital, Central South University (No. 202106108).