
Abstract
Background:
Synovitis of the glenohumeral (GH) joint and the subacromial (SA) space is commonly observed during arthroscopic rotator cuff surgery.
Purpose:
To investigate the distribution, severity, and clinical implications of synovitis in the GH joint and SA space in patients with a full-thickness rotator cuff tear (RCT).
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were retrospectively collected from 207 patients with a full-thickness RCT who underwent arthroscopic repair. Preoperative parameters used in the clinical assessment included pain, range of motion (ROM), muscle strength, and functional scores. Macroscopic assessment of synovitis was performed intraoperatively in the 3 regions of interest (ROIs) of the GH joint and 4 ROIS of the SA space using an evaluation system. The distribution and severity of synovitis and the association between synovitis and clinical assessment were evaluated.
Results:
Synovitis was more severe in the GH joint than in the SA space (P < .001). Synovitis in the posterior GH joint and the lateral SA space, where most of the rotator cuff was located, was the most severe area among the ROIs of the GH joint and the SA space, respectively (P < .05). All types of pain, except for pain at rest, were associated with synovitis in the posterior GH joint (P < .05). All ROM measures were associated with synovitis in the posterior and inferior GH joint (|r| > 0.20; P < .05 for both). The strength of the supraspinatus and the infraspinatus was associated with synovitis in the posterior GH joint (P < .05). Shoulder function was associated with synovitis in the posterior and inferior GH joint and more in the posterior GH joint (P < .05 for both). Synovitis in the SA space was not associated with any of the clinical parameters.
Conclusion:
Synovitis in the posterior GH joint was the most severe form of synovitis in the GH joint in patients with a full-thickness RCT. Synovitis in the posterior GH joint was closely associated with increased pain and decreased ROM, muscle strength, and functional score. Synovitis in the SA space was milder and not associated with any clinical parameters.
The shoulder joint consists of 2 synovial areas, the glenohumeral (GH) joint and the subacromial (SA) bursa, and the rotator cuff is interposed between the 2 spaces.13,22 Shoulder pain is the third most common musculoskeletal symptom and is mainly caused by rotator cuff disease,15,18,27,32 which is considered a spectrum of rotator cuff pathologies from tendinopathy through rotator cuff tear (RCT) to rotator cuff arthropathy.29,36 It may be better regarded as a pan-joint disease in that it consists of the rotator cuff tendon and cuff muscles and tissues of the GH joint and the SA space, such as the synovium and proximal humerus.3,8,11,14,18,35,42
Synovitis in the GH joint and the SA space is commonly observed in arthroscopic rotator cuff surgery. Some studies on the knee have reported that synovitis is associated with symptoms such as pain and joint dysfunction in osteoarthritis and rheumatoid arthritis.1,16,30,34 These results imply that these symptoms may also be associated with synovitis in rotator cuff disease. Some laboratory studies have reported that synovial inflammation in the SA space plays an important role in shoulder pain in rotator cuff disease.2,4,13,26,37,42 However, few studies have investigated the distribution, severity, and clinical implications of synovitis with macroscopic grading because a systematic and reliable macroscopic grading system for synovitis in the GH joint and the SA space has only recently been proposed.6,18,25
This study aimed to investigate the distribution and severity of synovitis in the GH joint and the SA space and analyze its clinical implications in patients with a full-thickness RCT. We hypothesized that the distribution and severity of synovitis would vary in the GH joint and the SA space and would have different clinical implications in these patients.
Methods
Patient Enrollment
The institutional review board approved this retrospective cohort study of our hospital, and informed consent for registration was obtained from all patients. We reviewed the records of 311 patients with full-thickness RCT who underwent arthroscopic rotator cuff repair by a single surgeon (C.H.J.) at a single hospital between January 2013 and February 2015. Of these, 104 patients were excluded for the following reasons: (1) partial-thickness RCT (n = 51); (2) rotator cuff arthropathy (n = 11); (3) pyogenic infection (n = 1); (4) calcific tendinitis (n = 6); (5) isolated subscapularis tear (n = 7); (6) retear (n = 9); (7) impingement disease (n = 5); and (8) assessment questionnaire not available (n = 14). Thus, 207 patients were included in this study.
Preoperative Clinical Assessments
All patients were asked to complete a standardized assessment questionnaire to preoperatively evaluate their shoulder status. The clinical parameters used in the assessments included various types of pain, range of motion (ROM), muscle strength, and 6 commonly used functional scores. A visual analog scale (VAS) using a 10-cm scale ranging from no pain (0 cm) to unbearable pain (10 cm) was used to assess the pain at rest, in motion, at night, and at its worst. The mean pain scores were the mean of the pain scores at rest, during motion, and at night. A goniometer was used to measure ROM during active forward flexion, abduction, external rotation with the arm at the side, and internal rotation. Internal rotation was measured at vertebral levels and transformed into numbers from 1 for the buttocks to 17 for T2. The cutoff value for limitation of motion was defined as 120° for forward flexion and abduction, 30° for external rotation, and L3 for internal rotation. The strength of the supraspinatus, infraspinatus, and subscapularis muscles was measured in pounds (lb) using a handheld electronic device (CHS; CAS). The functional scores used included the American Shoulder and Elbow Surgeons (ASES) score, Constant score, University of California at Los Angeles (UCLA) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, Simple Shoulder Test (SST), and Shoulder Pain and Disability Index (SPADI).
Assessment of Synovitis and RCT With Arthroscopy
All arthroscopic surgeries were performed with the patients in the lateral decubitus position under general anesthesia, as described previously.17,20 In each case, systematic GH joint, SA space, and rotator cuff exploration were performed to document the synovitis, anteroposterior and mediolateral RCT sizes, involved tendons, tendon grades, tendon excursions, subscapularis tears, and biceps tears. Synovitis was assessed by an experienced shoulder surgeon (C.H.J.) in 3 and 4 regions of interest (ROIs) of the GH joint (anterior, inferior, and posterior) and the SA space (anterior, posterior, medial, and lateral), respectively, according to the macroscopic grading system proposed by our author group in a previous study 18 (Table 1). This grading system has been shown to have excellent inter- and intraobserver reliability, with an intraclass correlation coefficient of >0.8.
Macroscopic Grading System of Synovitis a
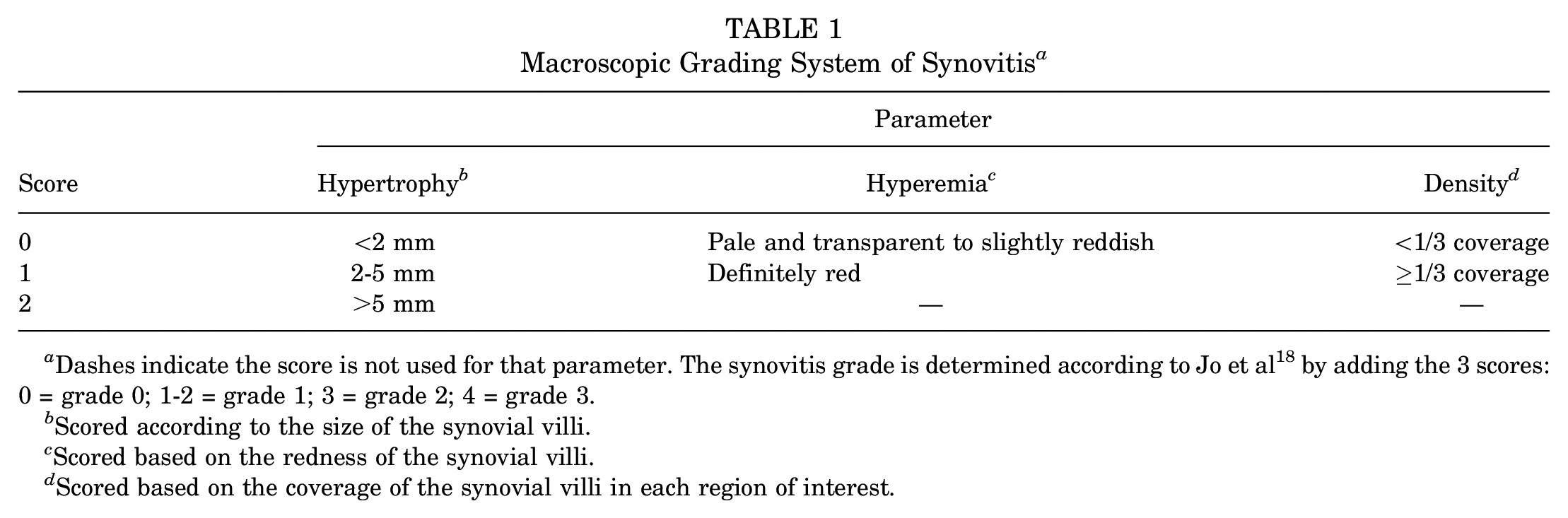
Dashes indicate the score is not used for that parameter. The synovitis grade is determined according to Jo et al 18 by adding the 3 scores: 0 = grade 0; 1-2 = grade 1; 3 = grade 2; 4 = grade 3.
Scored according to the size of the synovial villi.
Scored based on the redness of the synovial villi.
Scored based on the coverage of the synovial villi in each region of interest.
The 3 ROIs of the GH joint and 4 ROIs of the SA space were defined as previously described. 18 Tendon grade assesses rotator cuff quality using 3 gross tendon criteria 19 : (1) fraying over half of the tendon thickness; (2) delamination of the supraspinatus tendon; and (3) thinning of less than half of the normal thickness (graded as A, none of these criteria were met; B, fraying or delamination was identified; or C, both fraying and delamination or thinning regardless of the other criteria). Excursion evaluates the lateral displacement of the tear end by manual pulling 19 (graded as A, over the ridge of the greater tuberosity; B, within the original footprint in the greater tuberosity; or C, cannot be reduced to the original footprint). Rotator cuff repair and postoperative rehabilitation were performed as previously described.19,31
Statistical Analysis
All analyses were performed using IBM SPSS Statistics Version 27 (IBM Corp). Continuous variables were recorded as means and standard deviations. The associations between distribution and severity of synovitis in each ROI of the GH joint and the SA space and variables—including baseline characteristics and clinical parameters—were evaluated using the Spearman correlation coefficient (r) for continuous variables, the Student t test or the Mann-Whitney test for dichotomous variables, and the Kruskal-Wallis test or 1-way analysis of variance for polytomous variables. Values of |r| > 0.2 were considered to be associated. 9 A stepwise backward logistic regression analyses, with adjustments for covariates, was performed to confirm the risk factor of limitation of motion. There were no missing data. Statistical significance was set at P < .05.
Results
Baseline Characteristics
The baseline characteristics of the patients included in this study are summarized in Table 2. The study included 76 men (36.7%) and 131 women (63.3%). The mean age was 62.7 ± 7.8 years, with a mean symptom duration of 15.5 months. Pain on the dominant side (75.4%), medium-sized tears (59.4%), and Kellgren-Lawrence grade 0 and 1 (45.4% and 43.5%, respectively) were the most frequent. The mean number of involved tendons was 2.9 ± 1.1, and the most common tendon grade was B (55.6%). Other confounding factors, such as diabetes mellitus and thyroid disease, were also considered.
Baseline Characteristics of the Study Participants (N = 207) a

Data are reported as mean ± SD or n. M, medium; L, large; S, small; MSV, massive.
Prior diagnosis of diabetes mellitus or new findings of serum hemoglobin A1c level >6.4%.
Having a prior diagnosis of hyperthyroidism or hypothyroidism or new findings of free thyroxine (T4) > 1.70 ng/dL or < 0.93 ng/dL.
Subscapularis tear was graded according to the Lafosse classification in Lafosse et al. 24 Grading: 1 = partial lesion of superior one-third; 2 = complete lesion of superior one-third; 3 = complete lesion of superior two-thirds; 4 = complete lesion of the tendon but head centered and fatty degeneration classified as ≤stage 3; 5 = complete lesion of the tendon but eccentric head with coracoid impingement and fatty degeneration classified as ≥stage 3.
Age, sex, dominance, symptom duration, thyroid disease, and Kellgren-Lawrence grade were not associated with synovitis in any ROIs (P > .05 or |r| < 0.2). The presence of diabetes mellitus (P = .013), larger anteroposterior tear size (r = 0.265; P < .001), a larger number of involved tendons (P = .011), shorter excursion (P = .035), and higher grade of subscapularis tear (P = .004) were significantly associated with severe synovitis in the inferior GH joint. Larger Cofield type (posterior GH joint, P = .033; inferior GH joint, P <.001) and higher tendon grade (posterior GH joint, P = .002; inferior GH joint, P < .001) were associated with severe synovitis in the posterior and inferior GH joint (Supplemental Table S1, available separately).
Characteristics of Synovitis in Patients With RCTs
The macroscopic parameter scores—including hypertrophy, hyperemia, and density—were significantly higher in the GH joint than in the SA space (Table 3). The mean macroscopic grade of synovitis was also greater in the GH joint (1.49 ± 0.54) than in the SA space (0.81 ± 0.47) (P < .001).
Macroscopic Evaluation of Synovitis in the Glenohumeral Joint and Subacromial Space a

Dashes indicate areas that are not applicable.
Differences between regions of interest were statistically significant (Kruskal-Wallis test; P < .05).
Differences in mean macroscopic grade between the glenohumeral joint and subacromial space were statistically significant (paired t test; P < .05).
Differences in macroscopic grades among the regions of interest were statistically significant within the glenohumeral joint and the subacromial space (Mann-Whitney test; P < .05 for both), except for the comparison between the anterior subacromial space and the medial subacromial space (Mann-Whitney test; P = .231).
Of the 3 ROIs of the GH joint, the grade of synovitis was most severe in the posterior (1.71 ± 0.73), followed by anterior (1.52 ± 0.68) and inferior (1.25 ± 0.68) (P≤ .004) joint. Specifically, all 3 macroscopic parameters (hypertrophy, hyperemia, and density) were significantly higher in the posterior and anterior GH joint than in the inferior joint. Among the 4 ROIs of the SA space, the grade of the lateral synovitis was the highest (1.07 ± 0.58), whereas the posterior synovitis was the lowest, with all 3 significantly higher macroscopic parameters in the lateral SA space than in the posterior (0.32 ± 0.59) (P < .001).
Clinical Assessments
Pain. Pain in motion (P = .003), at night (P = .004), the mean pain (P = .004), and pain at worst (P < .001) were significantly associated with synovitis in the posterior GH joint (Table 4). VAS pain scores were significantly different between synovitis grades 1 and 3 in the posterior GH joint; pain during motion (4.4 ± 2.7 vs 6 ± 2.8; P = .045), pain at night (4.5 ± 2.9 vs 6.5 ± 3.1; P = .004), the mean pain (4 ± 2.4 vs 5.4 ± 2.3; P = .034), and worst pain (7 ± 2.4 vs 9 ± 1.9; P = .001). The difference in VAS scores between grades 2 and 3 were significant for pain at night (4.9 ± 2.6 vs 6.5 ± 3.1; P = .027) and the worst pain (7.3 ± 2.4 vs 9 ± 1.9; P = .006) (Figure 1A). The minimal clinically important difference (MCID) for the VAS pain score in rotator cuff disease as previously determined was 1.4 points, 39 and each significant difference in the VAS pain score between synovitis grades was found to be clinically significant.
Association Between Synovitis in the 7 Regions of Interest and Pain, ROM, Strength, and Functional Scores a
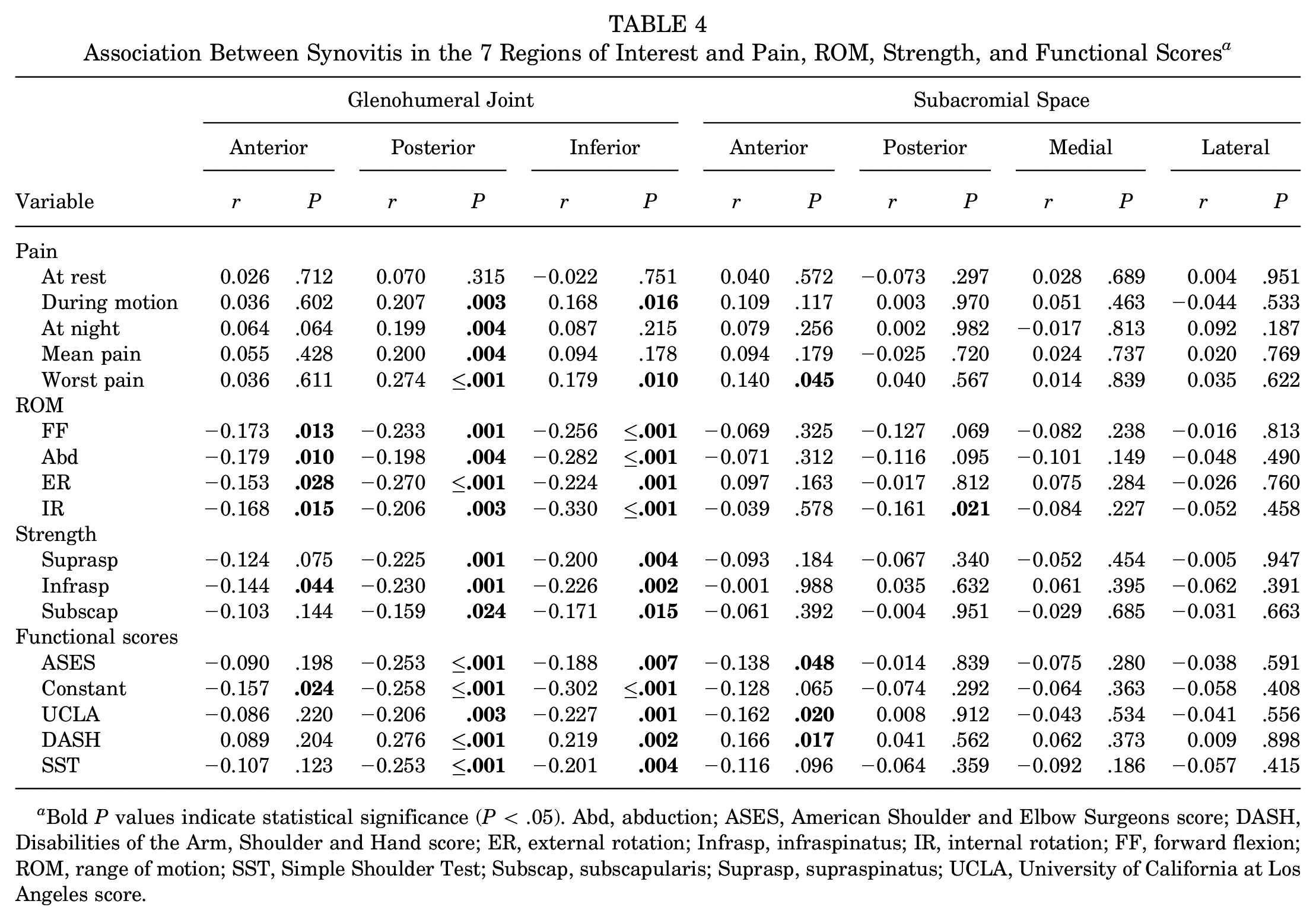
Bold P values indicate statistical significance (P < .05). Abd, abduction; ASES, American Shoulder and Elbow Surgeons score; DASH, Disabilities of the Arm, Shoulder and Hand score; ER, external rotation; Infrasp, infraspinatus; IR, internal rotation; FF, forward flexion; ROM, range of motion; SST, Simple Shoulder Test; Subscap, subscapularis; Suprasp, supraspinatus; UCLA, University of California at Los Angeles score.
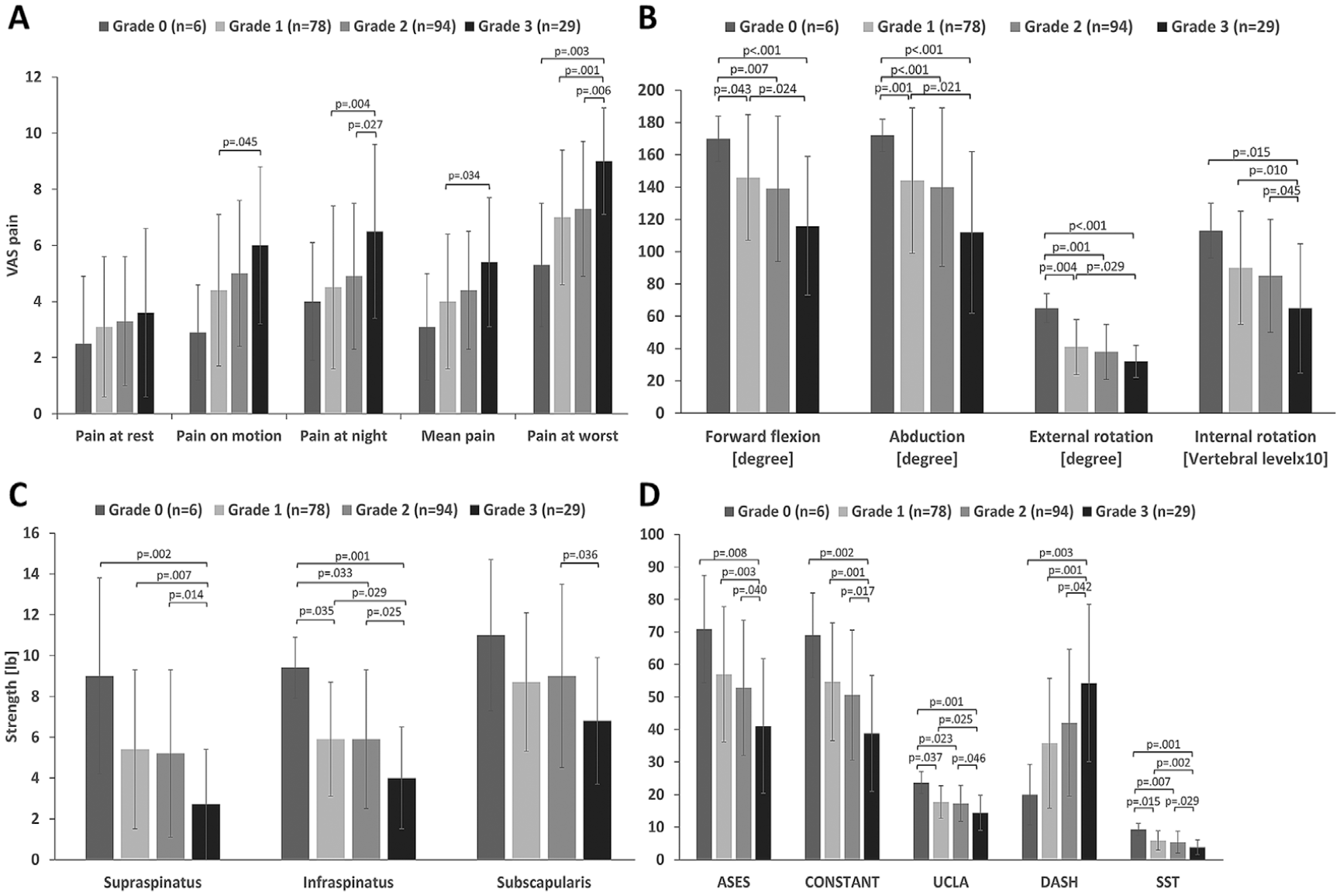
Comparison of (A) pain, (B) range of motion, (C) rotator cuff muscle strength, and (D) functional scores according to synovitis severity grade in the posterior glenohumeral joint. The bars indicate the mean value, and the error bars indicate the standard deviation. ASES, American Shoulder and Elbow Surgeons score; DASH, Disabilities of the Arm, Shoulder and Hand score; SST, Simple Shoulder Test; UCLA, University of California at Los Angeles score; VAS, visual analog scale.
There were no significant differences in VAS pain scores between grades 0, 1, and 2 of synovitis in the posterior GH joint for any pain. As the grade of synovitis in the posterior GH joint increased by 1, the score for pain during motion increased by 0.70 (P = .011), the score for pain at night increased by 0.80 (P = .006), the mean pain score increased by 0.60 (P = .010), and the score for the worst pain increased by 0.87 (P < .001) in the linear regression model.
No pain was associated with synovitis in the anterior and inferior GH joint or the SA space (Table 4 and Figure 2A).

Comparison of (A) pain, (B) range of motion, (C) rotator cuff muscle strength, and (D) functional scores according to synovitis severity grade in the inferior glenohumeral joint. The bars indicate the mean value, and the error bars indicate the standard deviation.
Range of Motion. Forward flexion, abduction, external rotation, and internal rotation were significantly associated with synovitis in the posterior and inferior GH joint (|r| > 0.2; P < .05) (Table 4). ROM in all planes decreased as the synovitis grade in the posterior and inferior GH joint increased (Figure 1B, 2B). ROM in all planes, except for internal rotation, decreased significantly in grade 1 synovitis of the posterior GH joint. Internal rotation decreased significantly in grade 3 synovitis of the posterior GH joint (Figure 1B). The ROM in all planes decreased significantly in grade 2 synovitis of the inferior GH joint, except for external rotation. External rotation did not differ between synovitis grades of the inferior GH joint (Figure 2B).
Using the definition of limitation of motion in this study, synovitis in the posterior GH joint was estimated to be a significant risk factor for limitation of forward flexion (P = .026), and synovitis in the inferior GH joint was estimated to be a significant risk factor for limitation of abduction (P = .016) (Supplemental Table S2, available separately).
Strength. The strength of the supraspinatus (r = −0.23; P = .001) and the infraspinatus (r = −0.23; P = .001) was associated with synovitis in the posterior GH joint (Table 4). As the grade of synovitis in the posterior GH joint increased, the strength of the supraspinatus, infraspinatus, and subscapularis decreased, particularly in grade 3 synovitis (Figure 1C). Although the strength of the supraspinatus (r = −0.20; P =.004) and the infraspinatus (r = −0.23; P = .002) was associated with synovitis in the inferior GH joint, there were no significant differences in strength between the grades of synovitis (Figure 2C). Synovitis in the anterior GH joint and the SA space was not associated with muscle strength.
Functional Scores. All 5 commonly used shoulder functional scores (ASES, Constant, UCLA, DASH, SST, and SPADI) were significantly associated with synovitis in the posterior and inferior GH joint (Table 4). As the grades of synovitis in the posterior GH joint increased by 2 or more, all 5 functional scores with known MCIDs worsened significantly (P < .05) and beyond the MCIDs: ASES (6.4-27.1); Constant (8-10.3); UCLA (3.0); DASH (10.2); SST (4.3); and SPADI (8-13) (Figure 1D).5,21,23,33,40,43 Only 3 functional scores (Constant, UCLA, and DASH) worsened significantly (P < .05) beyond the MCIDs as the grade of synovitis in the inferior GH joint increased by 2 or more (Figure 2D).
Discussion
The most important findings of this study were as follows: (1) synovitis in patients with a full-thickness RCT was more severe in all regions of the GH joint than in any of the regions of the SA space. The most severe location of synovitis in each area was the posterior GH joint and the lateral SA space, which are generally located near the tear; (2) all types of pain except pain at rest were significantly associated with synovitis in the posterior GH joint; (3) all measures of ROM were significantly associated with synovitis in the posterior and inferior GH joint, which were risk factors for limitation of forward flexion and abduction, respectively; (4) the strengths of the supraspinatus and the infraspinatus were significantly associated with synovitis in the posterior GH joint; (5) all 6 functional scores were significantly associated with synovitis in the posterior and inferior GH joint; and (6) synovitis in the SA space was not associated with any of the studied clinical parameters. Taken together, synovitis in the GH joint, especially the posterior GH joint, is clinically important, suggesting that any treatment strategy for synovitis should be directed first to the posterior GH joint.
Little data have been available regarding the association between baseline characteristics and synovitis. In our previous study on synovitis in patients with full-thickness RCT, we described the baseline characteristics of the patients in detail. Still, we did not evaluate the association between these characteristics and synovitis. 18 Kim et al 22 showed that longer symptom duration, diabetes mellitus, and larger tear size were associated with severe GH joint synovitis. However, the distribution of synovitis in the GH joint was not considered because of the limitation of the grading system. In this study, the presence of diabetes mellitus, larger anteroposterior tear size, a larger number of involved tendons, shorter excursion, higher grade of subscapularis tear, and higher tendon grade were associated with severe GH joint synovitis, especially the inferior GH joint. These findings are consistent with those of previous reports except for symptom duration. As symptom duration was marginally associated only with anterior synovitis in the GH joint in this study (r = −0.137; P =.05), reporting the distribution of synovitis would be as important as reporting the severity for the investigation of the implication of synovitis in rotator cuff disease. There has been debate as to whether knee osteoarthritis was associated with synovitis.7,16 In this study, shoulder osteoarthritis was not associated with synovitis.
Few studies have investigated the distribution and severity of synovitis in the GH joint and the SA space, as adequate macroscopic grading systems for shoulder synovitis were only recently available.6,18,22,25 In our previous study, 18 the severity of synovitis was significantly greater in the GH joint than in the SA space (1.54 ± 0.61 vs 0.94 ± 0.56; P < .001) and was most severe near the tear (ie, the posterior and anterior aspects of the GH joint and lateral and anterior aspects of the SA space). The findings of the present study, comprising a larger patient cohort, were consistent with those of our previous study, suggesting the reliability and reproducibility of the synovitis assessment system in the previous study and the credibility of the findings in this study. Lee et al 25 also showed that synovitis was more severe in the superior half and superoposterior and superoanterior aspects of the GH joint with their grading system in which 4 quarters of division in the GH joint with 2 parameters of vascularity and hypertrophy were used. Meanwhile, some studies only described the distribution of synovitis in the GH joint,3,6 and another has adopted different grading systems for the GH joint and the SA space. 22 Since the rotator cuff disease affects the GH joint and the SA space, a reproducible system that can assess both locations would be more useful for investigating and communicating the clinical implications of synovitis.
Generally, inflammation in the SA space has been considered one of the origins of shoulder pain in rotator cuff disease, a basis for performing SA decompression.2,4,13,26,37,42 Gotoh et al10,11,13 showed a significant association between inflammation in the SA space and pain in a series of studies investigating synovitis using molecular research methods or limited immunohistochemistry methods. One of the limitations of these previous studies was the absence of information regarding the precise origin and content of the samples— that is whether they came from the fibrous bursa near the greater tuberosity or were synovitis samples. Although most of their studies focused on the bursa and synovitis in the SA space, 1 study 12 investigated synovitis in the GH joint. In that study, Gotoh et al 12 reported that messenger ribonucleic acid (mRNA) expression of interleukin (IL)-1β and intracellular IL-1 receptor antagonist in the synovium of the GH joint was detected in rotator cuff disease but was inversely associated with shoulder pain. They concluded that synovitis in the GH joint appears to contribute less to shoulder pain in rotator cuff disease. These findings may contradict the results of this study. However, Gotoh et al 12 did not describe the distribution and severity of synovitis in the GH joint or investigate the association between synovitis and mRNA expression. Furthermore, synovium samples were harvested from the surrounding tissues through the rotator interval to the subscapularis bursa in the anterior region, in which synovitis was not associated with pain in the present study. Another study reported that cytokine mRNA and proteins from synovitis of the GH joint in patients with full-thickness RCT were more significantly expressed than in patients with a partial-thickness tear, suggesting more severe synovitis in the GH joint than in the SA space. 11 Therefore, the results of their studies may not necessarily contradict the findings of this study but would demonstrate that the distribution and severity of synovitis in the GH joint is clinically important rather than just its presence or absence.
On the other hand, Kim et al 22 showed that synovitis in the GH joint was associated with clinical parameters, including preoperative VAS pain scores. In contrast, synovitis in the SA space was not associated with clinical parameters. Candela et al 3 also reported that synovitis in the GH joint could be considered a cause of shoulder pain. However, neither of these studies investigated the association between clinical parameters and the distribution and severity of synovitis. This study investigated the clinical implications of synovitis in the GH joint and the SA space with regard to its distribution and severity and observed that posterior and inferior synovitis in the GH joint were most significantly associated with various clinical parameters. Controversy regarding whether the pain source is synovitis in the SA space or the GH joint might result from the absence of adequate communication tools—such as a macroscopic grading system, precise localization of harvesting site based on the recognition of synovitis distribution, and common approaches for both the GH joint and the SA space. Therefore, our results might provide a useful foundation for further investigations of synovitis in rotator cuff disease.
In this study, forward flexion, abduction, external rotation, and internal rotation were associated with posterior and inferior GH joint synovitis. Kim et al 22 reported that forward flexion, external rotation, and internal rotation were associated with synovitis in the GH joint but not in the SA space. Lee et al 25 showed that forward flexion and abduction, not external or internal rotation, were associated with vascularity and hypertrophy of the synovium in the anterosuperior, anteroinferior, and posteroinferior GH joint. In this study, synovitis in the posterior and inferior GH joint was a significant risk factor for forward flexion and abduction limitation, not external or internal rotation. These findings are supported by the chief complaints commonly presented in clinical settings. Forward flexion and abduction are motions that patients with RCTs commonly complain about, while external and internal rotations are motions that patients with frozen shoulders complain about. One study reported an association between synovitis and stiffness after a rotator cuff repair. 38 However, these results would be confounded by significant differences in the preoperative limitation of motion in external rotation (38.3° in the postoperative stiffness group vs 51.3° in the postoperative no-stiffness group; P < .001). Furthermore, that study used a scoring system to evaluate synovitis that did not differentiate between the locations of synovitis within the joint, which the authors also described as a study limitation. Taken together, the results showed that synovitis would not be related to external and internal rotation of the shoulder joint. They suggested that synovectomy in the posterior and inferior regions would not result in improvement.
The results of the present study demonstrated that the strength of the supraspinatus and the infraspinatus is associated with synovitis in the posterior GH joint, probably because the insertion of the supraspinatus and the infraspinatus is very close to the posterior GH joint, in which synovitis was the most severe. In contrast, the insertion of the subscapularis is not. In addition, strength may be affected by combined factors, including muscle atrophy, tendon tear, and pain. 41 More synovitis in the posterior GH joint may induce more pain in motion and lead to muscle atrophy and weakness. Similarly, functional scores also comprehensively measure the pain, ROM, and strength of the muscles necessary for daily living. Thus, functional scores may be affected by synovitis in the posterior and inferior GH joint, which is associated with pain, ROM, and strength. Functional scores may be more associated with synovitis in the posterior GH joint since synovitis in the posterior GH joint was associated with pain, ROM, and strength. In contrast, synovitis grade in the inferior GH joint was only associated with ROM. These deductions are consistent with the results of this study.
In a randomized controlled trial comparing extensive bursectomy and limited bursectomy for SA bursitis during arthroscopic rotator cuff repair, it was found that extensive bursectomy did not offer any advantages in terms of pain reduction or tendon integrity after surgery. 28 In fact, it delayed recovery of external rotation, potentially because of adhesion formation after extensive bursectomy, and increased bursal thickening. The present study's results align with these findings, as no association was observed between SA synovitis and clinical parameters. Consequently, it is advisable to avoid performing extensive bursectomy in the SA space during rotator cuff repair. To our knowledge, no studies have investigated the treatment of synovitis in the GH joint in patients with RCTs, except for those related to rheumatic diseases or pigmented villonodular synovitis. This suggests that treating synovitis, particularly in the posterior and inferior GH joint, may reduce pain and improve function after rotator cuff repair or even include nonsurgical treatment options for patients who do not undergo surgery. However, since synovitis in the GH joint is associated with the tear, 18 treatment of synovitis alone without addressing the RCT may not yield favorable outcomes in mid- to long-term follow-up. Well-designed, prospective studies are needed to further explore the clinical implications of synovitis in the context of RCTs and repair.
Limitations
This study had several limitations. First, this study only included patients who underwent surgery for RCTs and did not include patients with partial-thickness RCTs or those who did not undergo surgery because of mild symptoms. Second, the effect of painkillers was not considered when assessing clinical parameters. However, patients with more pain would tend to take more analgesics, and the VAS pain score would decrease, reinforcing our results. Our routine prescription of painkillers did not include nonsteroidal anti-inflammatory drugs; hence, the anti-inflammatory effect of painkillers on synovitis would not be dominant. Third, the present study did not include how synovitis affects surgical outcomes, as it focused on the preoperative clinical implications of synovitis. Future studies will address surgical outcomes. Additional prospective studies are also necessary to determine whether treating synovitis in the posterior and inferior GH joint, as proposed above, leads to better surgical outcomes.
Conclusion
Synovitis distribution and severity varied in the GH joint and the SA space and had different clinical implications in patients with an RCT. Synovitis in the posterior GH joint was the most severe form of synovitis and was closely associated with increased pain and decreased ROM, muscle strength, and functional score. Synovitis in the SA space was milder and not associated with any clinical parameters.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231207818 – Supplemental material for Clinical Implication of Glenohumeral and Subacromial Synovitis in Rotator Cuff Tears
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231207818 for Clinical Implication of Glenohumeral and Subacromial Synovitis in Rotator Cuff Tears by Geunwu Gimm, Jeong Yong Yoon, Eunmi Ahn, Sohee Oh and Chris Hyunchul Jo in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank all the participants for their support of this study and are also appreciative of the assistance provided by HyunJee Lim, Tae Ri Lee, Ji Tae Jeong, Sung Yeon Won, and Sehi Huh, who contributed to the successful completion of this study.
Final revision submitted April 22, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by grants from the Korea Health Industry Development Institute (No. HI20C0386), the National Research Foundation of Korea (No. 2022R1A2C2092854) funded by the Korean government (MSIT), and the Korean Fund for Regenerative Medicine (22C0608L1-11) funded by the Ministry of Science and Information and Communication Technology and the Ministry of Health and Welfare. C.H.J. has stock in Acesostem Biostrategies. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Boramae Medical Center (no. 26-2016-88).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.