
Abstract
Background:
Quadriceps tendon soft tissue autograft represents an increasingly popular graft option for anterior cruciate ligament reconstruction (ACLR), particularly for adolescents, some of whom have an open physis, precluding use of graft options with bone plugs.
Purpose/Hypothesis:
The purpose of this study was to quantify return-to-sport performance assessments in adolescents at 6 months after ACLR with all–soft tissue quadriceps tendon autograft (ACLR-Q) versus hamstring tendon autograft (ACLR-HS). It was hypothesized that ACLR-Q would be associated with improved hamstring strength and hamstring-to-quadriceps (HS:Q) ratios compared with ACLR-HS, albeit with decreased quadriceps strength.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were patients aged 12 to 19 years who underwent primary ACLR by a single surgeon and who completed a return-to-sport performance assessment between 5 and 9 months postoperatively. The performance assessment included manual muscle strength tests (hamstring, quadriceps, hip abductor and adductor), dynamic balance test (Y-balance), and functional hop tests (single hop, triple hop, crossover hop, 6-m timed hop). Data were converted to limb symmetry indices, and limb symmetry index deficits were compared between the ACLR-Q and ACLR-HS cohorts using the Student t test or Wilcoxon-Mann-Whitney test.
Results:
An initial cohort of 90 ACLR-Q patients was compared with 54 ACLR-HS patients, with no significant differences in patient characteristics. Differences in meniscal repair rates, however, prompted use of propensity score matching on age, sex, body mass index, meniscectomy, and meniscal repair to produce comparable subcohorts. The matching resulted in 67 ACLR-Q and 52 ACLR-HS patients. Hamstring strength deficits were significantly greater in ACLR-HS versus ACLR-Q patients (−40.5% vs −5.7%; P < .001). Quadriceps strength deficits were significantly greater in ACLR-Q versus ACLR-HS patients (−12.8% vs −0.4%; P < .001). ACLR-Q patients had a significantly greater HS:Q ratio on the operative knee (P < .001) and significantly higher Y-balance composite score deficits (−2.9% vs −0.4%; P = .01) than ACLR-HS patients. There were no significant differences in hop test performance between groups.
Conclusion:
Adolescent athletes who underwent ACLR-Q showed significantly greater quadriceps strength deficits but significantly smaller hamstring strength deficits than those who underwent ACLR-HS, leading to more favorable HS:Q ratios in ACLR-Q patients at 6 months postoperatively.
Keywords
Anterior cruciate ligament (ACL) injury is an increasingly common injury in the pediatric and adolescent age groups, 49 owing in part to increasing competitive sport participation by younger athletes. 15 Currently, ACL reconstruction (ACLR) is recommended as the treatment of choice, as ACL deficiency is associated with secondary chondral and meniscal injuries.28,31 Although adolescents generally demonstrate good clinical results after ACLR with a high rate of return to sport (RTS), 30 subsequent graft rupture rates between 10% and 20% have been reported in the literature.25,54 Graft type, 25 timing of RTS, 12 hamstring strength, and hamstring-to-quadriceps (HS:Q) ratio have been shown to be risk factors for ACL graft failure.33,41
The 2 traditional graft choices for ACLR are hamstring and bone–patellar tendon–bone (BTB) autograft,2,6 with the quadriceps tendon autograft growing in popularity as an alternative soft tissue graft choice, particularly in the adolescent population. 17 However, soft tissue autografts may be preferable to autografts that involve harvesting of bone plugs. Grafts with bone plugs often cause greater donor-site morbidity, such as anterior knee pain and kneeling pain, 37 introduce risk of patellar fracture, and may not be a safe option in the adolescent population with open physes and significant growth remaining. 14 The quadriceps tendon soft tissue autograft has the benefit of minimal risk of growth disturbance using transphyseal or physeal-respecting techniques, 10 while providing advantages over hamstring tendon autografts, which may include larger, more consistent graft dimensions 11 and improved knee flexor strength postoperatively. 34 Clinically, ACLR with quadriceps tendon autograft (ACLR-Q) has been shown to have equivalent or better functional outcomes in comparison with ACLR with hamstring tendon autograft (ACLR-HS).8,34 In the adolescent population specifically, ACLR-Q has demonstrated strong functional outcomes with lower rates of graft failure compared with hamstring tendon autografts.17,42
Most patients expect to continue their athletic careers at their preinjury level after ACLR. 53 Therefore, graft choice may be influenced by patients’ likelihood of returning to sport. RTS performance assessments help to determine where a patient is in one’s rehabilitation and whether one is ready to RTS or not. These RTS assessments often include quadriceps and hamstring strength, functional assessments including hop tests, and measures involving quality of movement. 52 Postoperative hamstring and quadriceps strength is often compared with the opposite limb using a limb symmetry index (LSI), which is expressed as a percentage and calculated as ([involved limb/uninvolved limb] − 1) × 100%.9,18 Commonly cited benchmarks used to determine readiness to RTS include hamstring and quadriceps LSIs within −10% before RTS, while LSIs within −20% are recommended before return to running.1,26,35,38,50 Quantitative data of the RTS performance assessments have not been well studied in youth athletes, specifically with respect to the quadriceps tendon autograft.
The purpose of this study was to quantify postoperative RTS performance assessments in adolescents 6 months after ACLR-Q versus those with ACLR-HS. Our hypothesis was that ACLR-Q would be associated with improved hamstring strength and HS:Q ratios compared with ACLR-HS, albeit with decreased postoperative quadriceps strength at 6 months.
Methods
Study Design
The institutional review board of the study institution approved the current study protocol, and all included participants or their parent/guardian provided written informed consent. Adolescent patients who underwent primary ACLR using either quadriceps or hamstring tendon autograft routinely underwent RTS strength performance assessments as part of standard postoperative care to assess rehabilitation progress and potential performance deficits 6 months after ACLR. The postoperative rehabilitation protocol for all patients consisted of that published by the Multicenter Orthopaedic Outcomes Network group. 56 The demographic data (age, height, and weight) were obtained from a review of the patient’s electronic medical record. The status and treatment of any meniscal tears, as well as the duration from ACLR to testing, were documented and included in the analysis.
Patient Selection
Included in the study were adolescent athletes who were 12 to 19 years of age, sustained ACL injuries and underwent primary ACLR between 2017 and 2019 with either all–soft tissue ACLR-Q or ACLR-HS by a single surgeon (B.E.H.) at a pediatric tertiary-care hospital. The choice of the all–soft tissue graft that was used (ACLR-Q vs ACLR-HS) was based on patient/family preference after a discussion with the surgical team regarding potential risks and benefits of both graft types including donor-site morbidity. Patients also needed to have completed an RTS performance assessment between 5 and 9 months postoperatively. Exclusion criteria were athletes ≥20 years of age, prior ipsilateral or contralateral knee surgery, use of allograft for the ACLR, and concomitant procedures other than meniscal repair or meniscectomy.
RTS Performance Assessments and Follow-up
The RTS performance assessments were completed by health care practitioners (board-certified athletic trainers) as part of the standard rehabilitation care at approximately 6 months postoperatively (between 5 and 9 months). The RTS performance assessments included strength testing (hip abductor, hip adductor, quadriceps, hamstring), HS:Q ratios, balance testing (Y-balance composite score), and functional hop testing (single hop, triple hop, crossover hop, 6-m timed hop).
Muscle Strength Tests
Quadriceps strength was assessed with patients seated at the edge of the treatment table with their knees at 90° of flexion. A handheld dynamometer (Hoggan Scientific LLC) was then applied to the anterior aspect of the distal tibia above the dome of the talus, and patients were asked to extend their knees with maximum effort. For hamstrings strength, patients were in a prone position with 90° of knee flexion, and a handheld dynamometer was applied at the posterior side (Achilles tendon side) of the distal tibia. Patients were then asked to further flex their knees toward the hip with maximum effort. For hip abductor strength testing, patients lay on their side; a handheld dynamometer was applied above the lateral malleolus, and patients were asked to move their legs toward the ceiling with maximum effort (direction of hip abduction).46-48
Dynamic Balance Test
Dynamic balance was measured using a commercially available Y-balance assessment system (Functional Movement System). Participants were allowed to practice several times after instructions were provided then were asked to stand at the center of the equipment and push a plastic piece to anterior, posteromedial, and posterolateral directions, respectively. 45 This was performed 3 times in each direction for both limbs. The mean distance for each direction was used for the analysis with the composite score calculated by taking the sum of the 3 distances and dividing by 3 times the limb length, multiplied by 100.19,45
Functional Hop Tests
Four types of hop tests were performed: the single hop, triple hop, crossover hop, and 6-m timed hop. Instructions were given before each hop test, and participants practiced each hop task several times. During the single-hop test, participants hopped 1 time with a single leg and were asked to maintain balance in landing for approximately 3 seconds. For the triple-hop test, participants hopped 3 times consecutively with a single leg and were asked to maintain balance in landing for 3 seconds on the final landing. In the crossover hop, participants hopped 3 times with zigzag figures (medial, lateral, and medial sequences) using a single leg. Participants were asked to maintain balance for 3 seconds at the landing of the final hop. For single hop and crossover hop, if participants could not maintain their balance for 3 seconds, a retest was performed. For the 6-m timed hop, participants were asked to hop a 6-m distance as fast as possible. Tape measures and stopwatches were used to perform the test. 45
Strength and functional deficits were reported as LSIs of the ACLR limb compared with the uninvolved limb, subtracting 100% from the scores.
Statistical Analysis
Patient characteristics, meniscal treatment, and RTS performance assessment outcomes were summarized for both the ACLR-Q and the ACLR-HS groups. Continuous variables were summarized using means and standard deviations, with median and interquartile range (IQR) values used where appropriate. Counts and percentages were used for categorical variables. LSI deficits were compared between the ACLR-Q group and the ACLR-HS group using the Student t test or the Wilcoxon-Mann-Whitney test depending on normality of the data. Propensity score matching was conducted to create matched subcohorts and remove meniscal repair rates as a confounder. The IBM SPSS statistical software (Version 21; SPSS Inc) was used for all analyses, and P < .05 was used as the threshold for statistical significance.
Results
Of 181 possible patients, 144 patients (90 ACLR-Q and 54 ACLR-HS patients) were initially identified as meeting the inclusion criteria for the study. There were no significant differences in demographic characteristics between the 2 groups. Differences in meniscal repair rates, however, prompted use of propensity score matching on age, sex, body mass index, meniscectomy, and meniscal repair to produce comparable subcohorts. After the propensity score matching, 119 patients were included in the study (67 ACLR-Q and 52 ACLR-HS patients) (Figure 1). The mean age of these patients was 15.7 ± 1.68 years, and 61% were female. The characteristics of the final study participants are shown in Table 1.
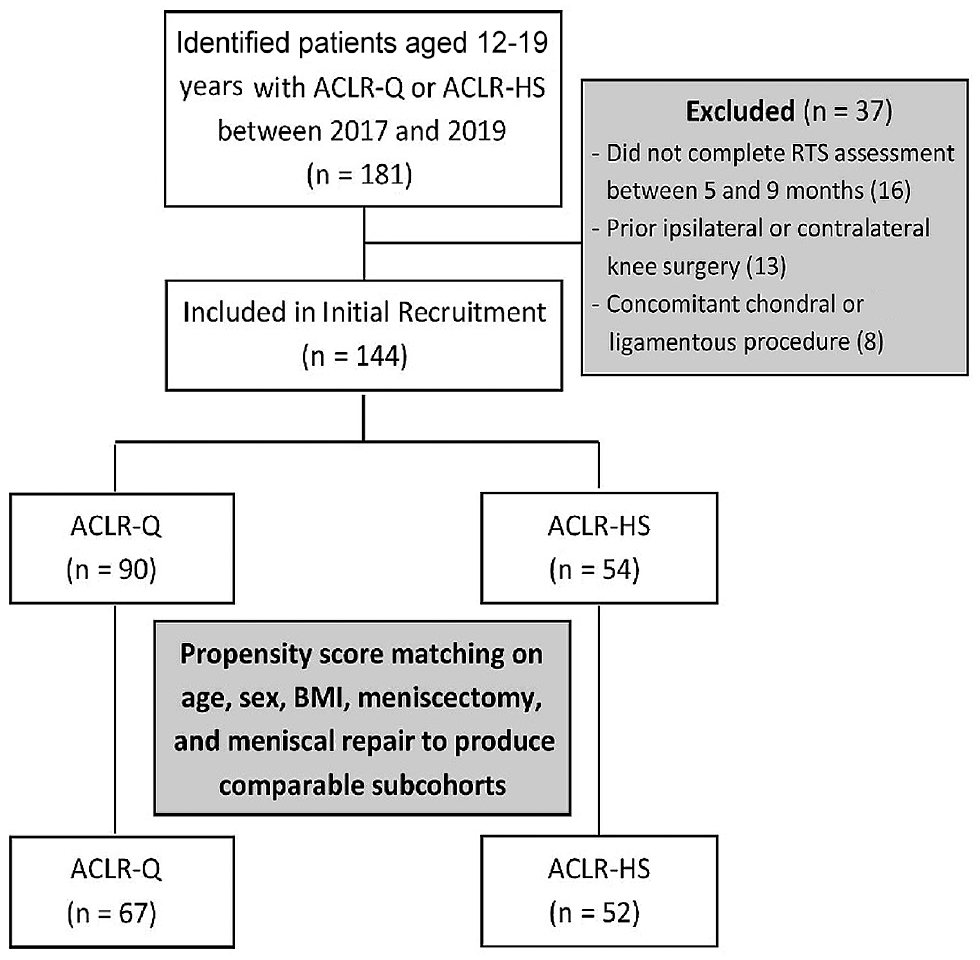
Flow diagram depicting the ACLR patients included in the study along with reasons for exclusion at each stage. ACLR, anterior cruciate ligament reconstruction; ACLR-HS, ACLR with hamstring tendon autograft; ACLR-Q, ACLR with quadriceps tendon autograft; BMI, body mass index; RTS, return to sport.
Characteristics of the Matched Cohort Overall and by Autograft Type a

Data are reported as mean ± SD or n (%). ACLR-Q, anterior cruciate ligament reconstruction with quadriceps tendon autograft; ACLR-HS, anterior cruciate ligament reconstruction with hamstring tendon autograft.
Within the ACLR-Q group, the median time to RTS performance assessment was 6.3 months (IQR, 5.98-6.70 months), and it was 6.1 months (IQR, 6.0-6.47 months) within the ACLR-HS group. Concomitant meniscal pathology was addressed with meniscectomy in 30% of patients and with meniscal repair in 43% within the ACLR-Q group. In the ACLR-HS group, 33% underwent meniscectomy and 52% underwent a meniscal repair.
When comparing the ACLR-Q and ACLR-HS groups, there was no significant difference in mean hip abductor strength LSI (2.8% ± 22.68% vs 4.7% ± 20.04%; P = .62) or adductor strength LSI (−0.4% ± 12.14% vs −1.3% ± 13.00%; P = .71). However, mean hamstring strength LSI deficits were significantly greater in ACLR-HS patients than ACLR-Q patients (−40.5% vs −5.7%; P < .001). Conversely, mean quadriceps strength LSI deficits were significantly greater in ACLR-Q patients versus ACLR-HS patients, who did not on average demonstrate deficits (−12.8% vs −0.4%; P < .001). ACLR-Q patients had a significantly greater mean HS:Q ratio for the operative knee (0.6 ± 0.19 vs 0.3 ± 0.10; P < .001).
There was no significant difference in mean single-leg hop LSI deficits (−10.1% ± 14.07% vs −9.1% ± 15.13%; P = .76), mean crossover-hop LSI deficits (−8.1% ± 11.30% vs −2.0% ± 17.66%; P = .09), or mean 6-m timed hop LSI, in which there was not a deficit in either group (6.0% ± 10.66% vs 4.1% ± 11.71%; P = .43). ACLR-Q patients demonstrated significantly larger Y-balance mean composite score deficits than ACLR-HS patients (−2.9% vs −0.4%; P = .01) (Table 2).
RTS Performance by Matched-Patient Autograft Type a

Data are reported as median [IQR], mean ± SD, or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ACLR-HS, anterior cruciate ligament reconstruction with hamstring tendon autograft; ACLR-Q, anterior cruciate ligament reconstruction with quadriceps tendon autograft; HS:Q, hamstring-to-quadriceps; LSI, limb symmetry index; RTS, return to sport.
The number in parentheses represents the number of patients with available data for the given characteristic.
Discussion
The current study demonstrated that adolescent athletes who underwent ACLR-HS showed significantly greater mean hamstring strength deficits of 40.5% compared with those who underwent ACLR-Q. Furthermore, ACLR-HS patients demonstrated a significantly reduced mean HS:Q ratio, thus supporting the study hypothesis. Given that the hamstring muscles and other knee flexor muscle groups may be considered the most important functional or dynamic knee stabilizers,5,33,41 the sequelae of such severe weakness may be considered clinically significant deficits, particularly as they relate to risk of ACL retear and graft rupture. Notably, patients who underwent ACLR-Q had significantly greater mean quadriceps strength deficits—12.8% at 6 months postoperatively—compared with patients who underwent ACLR-HS. However, these differences did not seem to have a substantial functional influence, as there was no significant difference in functional hop test performances between the 2 groups. While the difference in Y-balance composite score deficit between the ACLR-Q (−2.9%) and the ACLR-HS groups (−0.4%) also met the threshold for statistical significance, there may be minimal clinical significance to such a difference, as both deficits were quite small and well within the commonly accepted threshold of 10% deficit,1,26,35,38,50 or a more strict 6% deficit,7,36,43 that may be used to gauge what is safe or reasonable for clearing patients to RTS.
The magnitude of quadriceps weakness at 6 months after ACLR-Q (mean LSI: −12.8%) in this study is somewhat expected, based on results from previous studies after ACLR with both quadriceps or BTB autograft harvest,22,27,47 both of which represent disruptions to the normal function or integrity of the extensor mechanism, simply at different points along the length of the entire muscle-tendon unit. A recent study assessing muscle strength in adolescents 6 to 9 months post-ACLR using BTB autografts reported a mean 12.2% deficit in quadriceps strength. 47 Similarly, Hunnicutt et al 27 assessed 30 patients undergoing ACLR with either quadriceps tendon or BTB autograft and found similar quadriceps strength LSIs between the 2 groups at a mean of 8 months postoperatively. Additionally, Han et al 22 studied 144 patients and found no significant difference in quadriceps isokinetic strength after ACLR with either quadriceps tendon autograft or BTB autograft at 1 year postoperatively. While Hughes et al 26 found that patients who had undergone ACLR with quadriceps tendon autografts had significantly greater quadriceps isokinetic strength deficits compared to those with BTB autografts at 5 to 8 months postoperatively, there was no significant difference between the groups at the 9- to 15-month follow-up.
The adolescent athletes in this study with ACLR-HS demonstrated severe hamstring deficits with mean LSI values of −40.5%, as well as a significantly reduced HS:Q ratio of 0.3. Commonly cited benchmarks used to determine readiness to RTS include hamstring and quadriceps LSIs within −10% before RTS, while LSIs within −20% are recommended before return to running.1,26,35,38,50 Fischer et al 16 compared mostly adult patients who had undergone ACLR with either hamstring or quadriceps tendon autograft and similarly found that the hamstring tendon autograft group had significantly reduced HS:Q ratios at both 5.5 and 7.6 months postoperatively. Higher HS:Q ratios may be clinically important, as a study by Kyritsis et al 33 in professional athletes found that hamstring strength deficits were associated with an increased risk of graft failure. Specifically, the study found that for each 10% decrease in HS:Q ratio there was a >10-fold increase in risk of graft failure. Furthermore, Palmieri-Smith et al 41 found that in patients who previously had ACLR, those who did not sustain reinjury had higher levels of hamstring activity before landing, further substantiating the importance of hamstring strength in preventing reinjury. In 2 previous studies, the magnitude of the hamstring deficit was not as severe, with mean LSIs of −20.5% at 5 to 8 months 26 and −13.7% at 5.5 months, 16 respectively. However, the patients in these studies were not exclusively adolescents. In a previous study of adolescent patients ≤21 years of age, a mean hamstring strength deficit of 31.7% was reported when hamstring tendon autografts were used. 47 Given that only patients ≤19 years of age were included in the current study, the magnitude and, in kind, the clinical impact of hamstring deficits after ACLR-HS may be higher in younger populations.
Importantly, the adolescent athletes in the ACLR-Q group in the current study underwent RTS performance assessments at a median of 6.3 months postoperatively. Considering the commonly used benchmark of 10% deficits in LSIs,1,26,35,38,50 the only RTS performance assessment for which these patients, on average, did not meet the benchmark was the quadriceps strength LSI (mean: −12.8%). However, a 10% quadriceps deficit may not be as important as a definitive threshold for RTS, as Novaretti et al 39 found that there was no significant difference in the rate of return to preinjury level of sport at 6 months using either a 10% or a 20% quadriceps strength deficit threshold. In other words, a 6-month time frame may be too early to use for RTS criteria, given that 9-month testing may show adequate RTS performance for the quadriceps autograft group. A recent study evaluating RTS assessments in adolescents after ACLR-Q found a similar quadriceps LSI deficit of 15% at 6 months. 44 However, the authors found that at 9 months there was significant improvement in the quadriceps strength LSI deficits, to a magnitude of 7.5%. 44
Although the current study demonstrated a statistically significant difference in Y-balance composite scores between the ACLR-Q (−2.9%) and ACLR-HS (−0.4%) groups, this difference does not likely represent a clinically important difference. In previous studies examining the relationship between the Y-balance test in athletes and risk of future lower extremity injuries, a threshold of 6% deficit on the composite test has been reported to represent a clinically important value.7,36,43
Finally, there was no significant difference in functional hop test performance between the ACLR-Q and ACLR-HS groups in the current study. Moreover, the magnitude of LSI deficits for each of the functional hop tests was either close to, or met the established criteria of, <10% deficit for safely returning to sport, which has been previously established.21,33 Quadriceps strength and function have been shown to play a vital role in functional performance and hop tests.23,40,57 Therefore, the functional hop test results from the current study suggest that the patients in this study may have a promising ability to achieve quadriceps recovery among adolescent ACLR-Q patients. However, it is interesting to note that crossover/ 6-m timed hop test and Y-balance deficits were <10% for both groups despite a mean quadriceps deficit of 12.8% and a mean hamstring deficit of 40.5%. Several previous studies have similarly found a lack of association between strength deficits and hop test performance after ACLR.3,24,29 Some have suggested that this lack of correlation relates to patients’ ability to compensate for strength deficits with strong hip or trunk muscles.3,24,29 While it has been previously reported that quadriceps deficit at 6 months postoperatively does not affect the probability of returning to sport, 32 others have found that quadriceps strength deficits increase the risk of ACL reinjury. 20 Future studies assessing the longer term impacts of strength deficits, functional hop test results, and Y-balance composite scores on patient-reported outcomes, functional outcomes, and rerupture rates will help to better discern the clinical implications of the deficits identified in the present study. A better understanding of the future clinical implications of the 6-month strength deficits identified in the present study may help us understand whether consideration of changes to the postoperative rehabilitation protocol for these patients might be important.
Limitations
Limitations of this investigation include the study design, which was a retrospective rather than prospective cohort study or randomized controlled trial. However, in order to mitigate effects from confounding variables, propensity-matched scoring was used to create comparable subgroups. We also did not collect race- and ethnicity-related information. Several recent studies have suggested that racial and ethnic parameters influence the care and outcomes of ACLR patients, and the absence of these variables may have affected the results of the current study.4,13 Furthermore, the RTS testing was performed at a median of 6.2 months from surgery. Repeat RTS performance assessments at a later time point may have further demonstrated the readiness of the adolescent athletes to RTS after ACLR with either of the soft tissue autograft options. The contralateral limb was used for comparison to determine the strength and functional deficits of the operative limb. Because patients can experience detraining and possibly atrophy of the uninvolved limb after ACLR, these LSI values could overestimate the strength and function of the operative limb compared with the true preinjury capacity level. 55 Conversely, the contralateral limb could experience gains in strength throughout rehabilitation, which can cause LSI values to underestimate the absolute strength of the operative limb relative to baseline.
Furthermore, isometric measures were used to quantify strength in this study. Isokinetic strength measures might have provided more reliable measures of strength. Preoperative testing was not performed in this study and may have served as a useful comparison, particularly of the uninvolved limb. In addition, we did not assess whether the adolescent athletes included were ultimately able to RTS or if they were able to do so at their preinjury level. Although a proper assessment of other RTS outcomes would not have been possible given the timeline of the study, it remains an important consideration for future investigation. Moreover, it is important to note that there are a number of other important factors that play a role in the ability to RTS, rather than simple performance benchmarks, such as an adolescent’s psychological readiness. 51 Therefore, the results of this study should be taken in context of the larger RTS considerations that include an athlete’s mental and physical readiness as well as the level and type of sport participation.
Conclusion
Adolescent athletes who underwent ACLR-Q showed significantly greater quadriceps strength deficits (mean LSI: −12.8%), but significantly smaller hamstring strength deficits, than those who underwent ACLR-HS (mean LSI: −40.5%), leading to more favorable HS:Q ratios in ACLR-Q patients 6 months postoperatively. While Y-balance composite score deficits were smaller in ACLR-HS patients than ACLR-Q patients, no differences were detected in hop test performance. The degree to which these performance metrics influence eventual athletic performance and ACL graft-tear risk remains a critical area of continued investigation.
Footnotes
Final revision submitted April 18, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.H. has received nonconsulting fees from Arthrex; education payments from Arthrex, Kairos Surgical, and Pylant Medical; consulting fees from Imagen Technologies; and royalties from Springer Science & Business Media; B.E.H. also has stock/stock options in Imagen Technologies. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (reference No. IRB-P00032638).