
Abstract
Background:
The incidence of anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) tears in children and adolescents has increased over the past decade, with increasing numbers of ACL and PCL reconstructions in this patient population.
Purpose:
To evaluate the size and morphology of both the ACL and the PCL by magnetic resonance imaging (MRI) in different pediatric age groups.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
MRI examinations of 127 knees (67 female, 60 male; aged 0-18 years) were analyzed retrospectively. The cohort was split into 6 age subgroups, 1 subgroup for every 3 years (minimum 8 patients per subgroup). The following parameters were measured by 2 independent raters at 2 different time points: ACL length, anteroposterior and mediolateral ACL width, sagittal and coronal ACL inclination, inclination of the intercondylar notch, bicondylar width, notch width, coronal ACL and PCL width, PCL length, and sagittal width of the lateral femoral condyle. The following indices, areas, and volumes were calculated: sagittal width of the lateral femoral condyle/PCL length, ACL area and volume, notch width index, ACL width/notch width, PCL width/notch width, ACL width/bicondylar width, and PCL width/bicondylar width. A correlation analysis was performed for patient age, height, weight, and body mass index (BMI).
Results:
ACL length was between 18 and 37 mm, and ACL width was between 4 and 6 mm. PCL length ranged between 27 and 43 mm, while PCL width was between 7 and 9 mm. Growth of the cruciate ligaments was the most pronounced between the ages of 4 and 12 years. Correlations with size and weight were strong, while BMI correlated slightly with the measurements. Measurements in female patients were slightly larger than in their male counterparts between the ages of 0 and 6 years, while male patients tended to have larger values starting from ages 7 to 9 years. These values were significantly larger in male patients from the ages of 16 to 18 years (P < .05).
Conclusion:
This study provides normative data on the morphology of pediatric anatomic features in the knee as a basis for age-appropriate and individualized surgical care of ACL and PCL injuries in children and adolescents.
Keywords
Knee ligament injuries are frequent, especially in physically active persons and athletes. High-level, performance-oriented sporting activities are increasingly practiced by children and adolescents. 16 Therefore, an incidence rate increase in ligamentous injuries, in particular anterior cruciate ligament (ACL) tears, was observed in children and adolescents with open growth plates.2,8 Approximately 3% of all ACL tears arise in skeletally immature patients. 13 The majority of ACL injuries in children and adolescents are in those aged 10 to 14 years. 15 Accordingly, increasing numbers of ACL reconstruction (ACLR) and posterior cruciate ligament (PCL) reconstruction (PCLR) are described for the pediatric population. 16
The morphology and anatomy of the cruciate ligaments is well known in adults.6,11 Unfortunately, there is still a lack of scientific studies regarding the size and morphology of these ligaments in children and adolescents. Only a few studies exist to fill this gap. Lima et al 10 analyzed retrospectively by magnetic resonance imaging (MRI) the development of the ACL in the pediatric population, although the PCL morphology was not described. Domzalski et al 4 evaluated the development of intercondylar notch width using MRI. They assessed the relationship between the cruciate ligaments and the width of the intercondylar notch during growth on MRIs of 76 children. Putur et al 14 studied the ACL growth with age in pediatric patients by MRI and described 3 distinct phases of growth with the highest growth rate per year for patients aged 1.5 to 5.75 years. Reliable and precise knowledge of the ACL and PCL morphology is fundamental for surgical reconstruction and its outcome in order to restore the native anatomy and to achieve correct graft positioning.
The aim of this study was to retrospectively evaluate the size and morphology of the ACL and the PCL in different pediatric age groups by MRI and to obtain normative data, which is the basis for age-adapted and individualized ACLR and PCLR in children and adolescents. We set up the hypothesis that ACL and PCL growth shows a varying growth pattern in different pediatric age groups.
Methods
Patient Cohort
A total of 264 MRI data sets were initially screened for eligibility. A final sample size of 127 MRI examinations (67 female and 60 male patients between the ages of 0 and 18 years) was included. Patients with a history of knee trauma, intra-articular pathologies (such as fractures, infectious or neoplastic lesions, dysplasia or aplasia of the ACL/PCL) or previous operations on cruciate ligaments were excluded (Figure 1). The cohort was split into 6 age subgroups, 1 subgroup for every 3 years, with a minimum of 8 patients per subgroup (group 1: 0-3 years, n = 8; group 2: 4-6 years, n = 9; group 3: 7-9 years, n = 20; group 4: 10-12 years, n = 27; group 5: 13-15 years, n = 40; group 6: 16-18 years, n = 23). Demographic data (age, height, weight, body mass index [BMI]) were taken from the medical reports. Written informed consent of the patients or legal guardians was given before inclusion in the study. Ethics committee approval was not required due to the retrospective study design.

Flowchart of patient inclusion and exclusion. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
MRI Data
The MRI data sets originated from 2011 to 2020 and were made available by the Department of Diagnostic and Interventional Radiology, Saarland University Medical Center, Homburg (Germany). MRI examinations were performed using a 3-T device (Magnetom Vida or Aera, Siemens Healtheneers). A Tx/Rx Knee 18 A3 T Tim Coil (Siemens Healtheneers) was used. For patients aged 0 to 3 years, a Body 18 long A3 T Tim Coil (Siemens Healtheneers) was used. The examinations were standardized, and sufficient image quality (image resolution, slice thickness 2.5-4 mm, complete presentation of all landmarks required for the assessment) was obligatory. T1-weighted turbo spin-echo (T1-TSE), T2-weighted TSE (T2-TSE), and short tau inversion recovery (STIR) sequences were obtained.
MRI Assessment
Analysis of the MRI examinations was performed according to previously established methods.4,10 Measurements in the sagittal plane were performed using T1-TSE and STIR sequences, in the transversal plane using T1-TSE/T2-TSE sequences and in the coronal plane using the T1-TSE sequence. The following parameters were determined on standardized sequences by 2 independent examiners (M.B., S.N.) blinded to the age of the patients at 2 different points in time using the Sectra Workstation picture archiving and communication system: ACL length, anteroposterior and mediolateral ACL width, sagittal and coronal ACL inclination, inclination of the intercondylar notch, bicondylar width, notch width, coronal ACL and PCL width, PCL length, and sagittal width of the lateral femoral condyle (Figures 2-6). Each measurement was repeated 3 times, and the mean value was calculated. The following indices, areas, and volumes were calculated: sagittal width of the lateral femoral condyle/PCL length, ACL area and volume, notch width index (NWI), ACL width/notch width, PCL width/notch width, ACL width/bicondylar width, PCL width/bicondylar width. The ACL area was calculated as (0.5 ×sagittal ACL width) × (0.5 ×coronal ACL width) ×π. The ACL volume was calculated as ACL area×sagittal ACL length. The NWI was calculated as intercondylar notch width/bicondylar width.
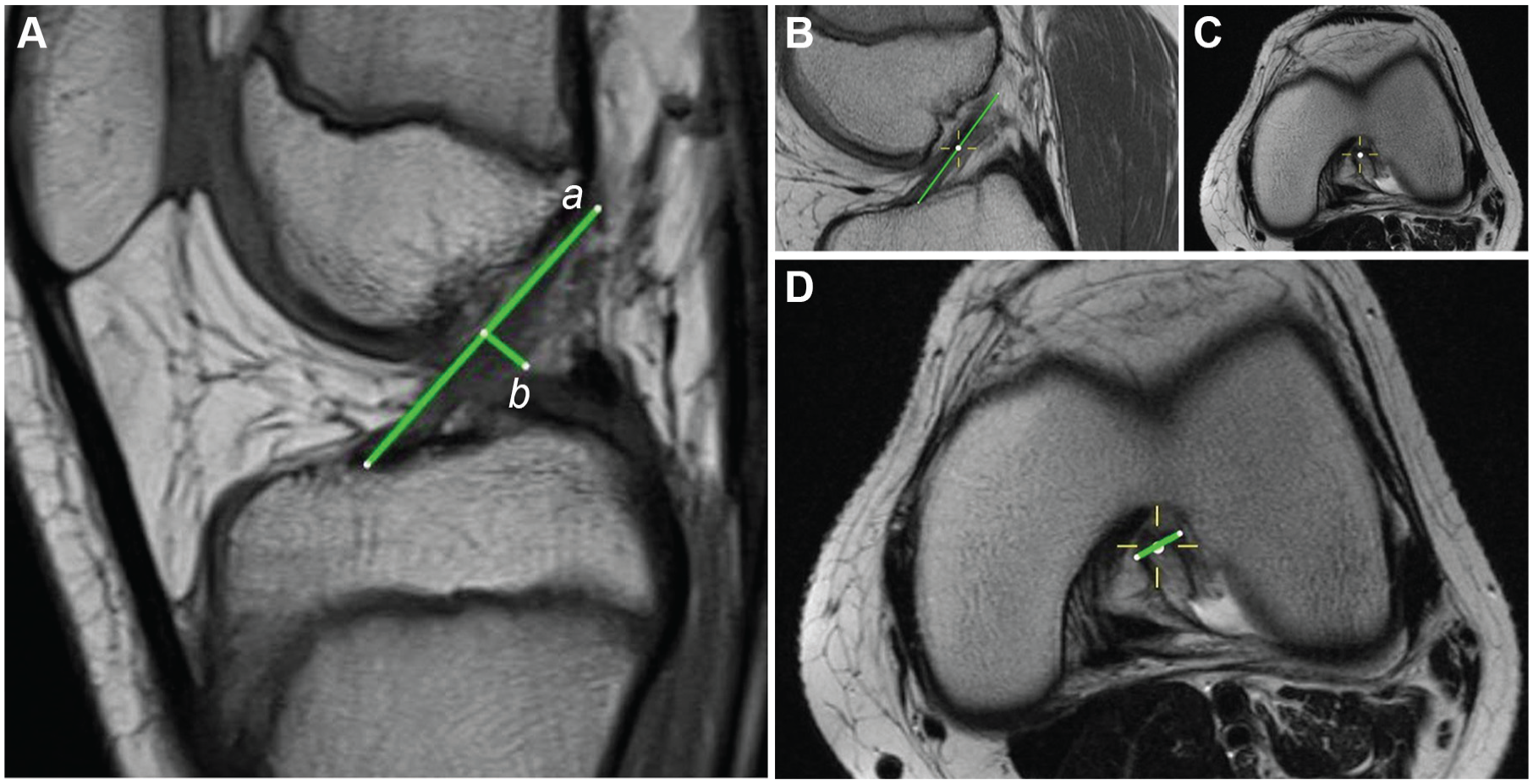
(A) Measurement on sagittal view magnetic resonance imaging of the anterior cruciate ligament (ACL) length (the distance between the most anterior and posterosuperior part of the ACL; a) and the ACL width (the anteroposterior distance of the ACL orthogonal to the midpoint of the ACL length; b). (B-D) Measurement of the ACL mediolateral width in the transversal plane: (B) mark of the midpoint of the ACL length in the sagittal plane; (C) transfer of this point into the corresponding transversal plane; (D) measurement of the mediolateral ACL width.
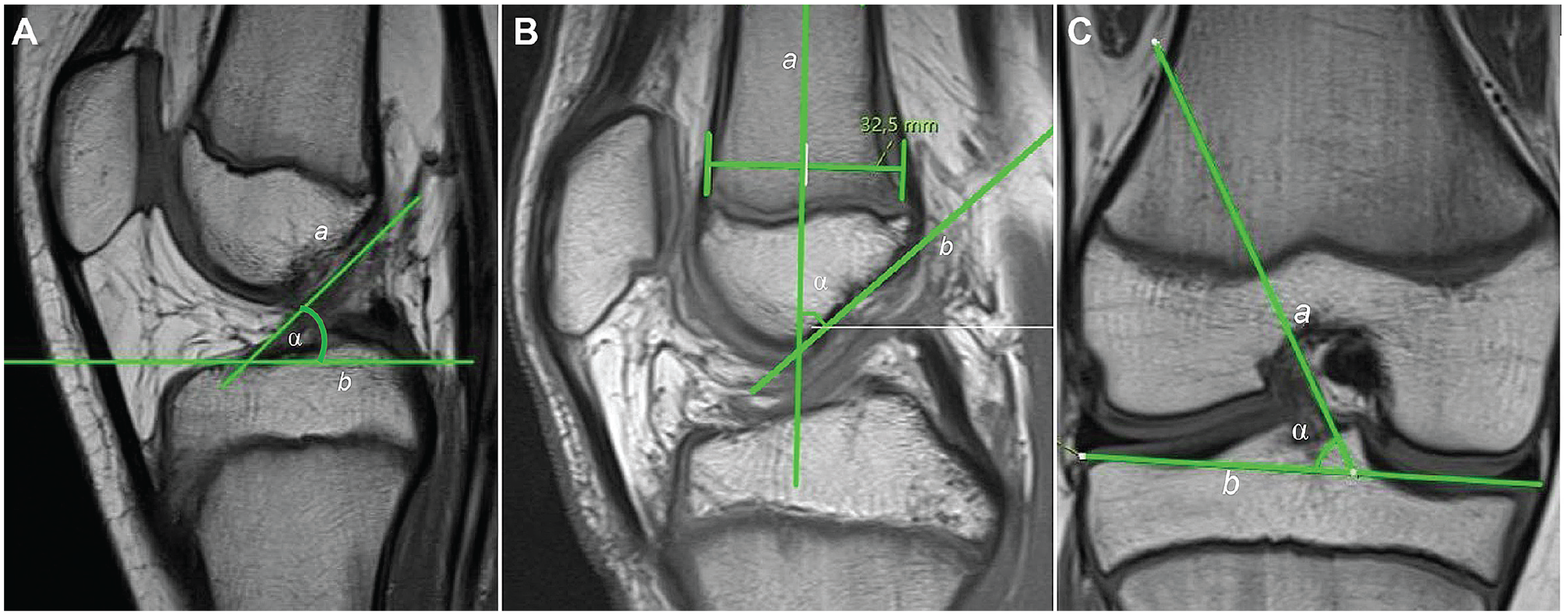
(A) Measurement of the anterior cruciate ligament (ACL) inclination angle in the sagittal plane (α) is formed by a tangent aligned to the anterior border of the ACL (a) and a tangent aligned to the lateral tibial plateau (b). (B) Measurement of the inclination angle of the intercondylar notch in the sagittal plane (α) is formed by the midline through the distal femur (a) and the tangent aligned to the roof of the intercondylar notch (b). (C) Measurement of the ACL inclination angle in the coronal plane (α) is formed by a tangent aligned to the medial border of the ACL (a) and a tangent aligned to the most medial and lateral border of the tibial plateau (b).

(A) Measurement of bicondylar and intercondylar notch width in the coronal plane: creating a tangent aligned to the distal medial and lateral femoral condyles (blue line); creating a second line (green-white-green line [distance AB) parallel to the blue line at the level of the popliteal groove (*); bicondylar width: green-white-green line (distance AB); intercondylar notch width: white line (distance CD). (B) Measurement of ACL and PCL width in the coronal plane: ACL width (blue line), PCL width (red line). ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
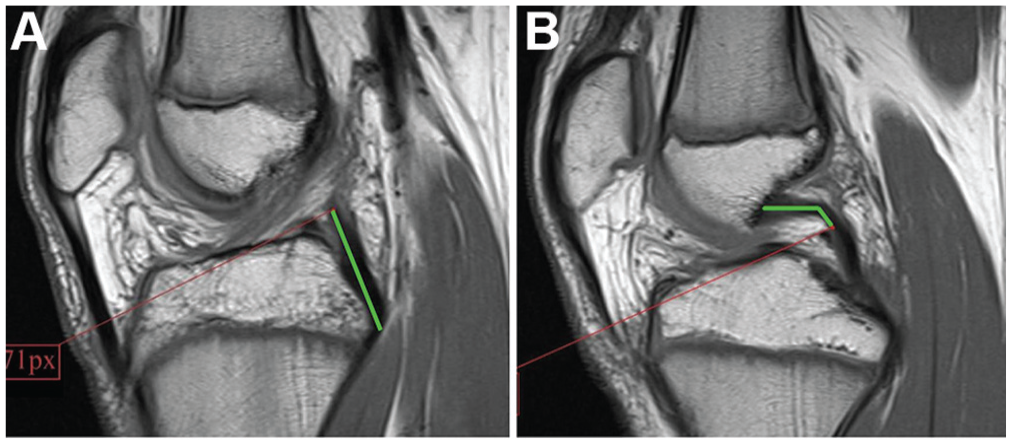
Measurement of posterior cruciate ligament (PCL) length in the sagittal plane in 2 consecutive magnetic resonance imaging slices. (A) Measurement of the distal part of the PCL (green line) and marking of the most proximal point of this measurement by pixel coordinates using Microsoft Paint Version 19H1. (B) Start of the PCL measurement in the next slice from this point (green line).

Measurement of lateral femoral condylar width in the sagittal plane. (A) Creating a tangent to the ventral distal femoral cortex (green line) and (B) transferring this line to the slice showing the lateral femoral condyle and creating an orthogonal line passing through the epiphyses (red line). The distance of the red line is the width of the lateral femoral condyle.
Statistical Analysis
Statistical analyses were performed in IBM SPSS Statistics Version 25. Descriptive statistics are reported as means ± SDs with ranges. The intraobserver reliability of the MRI measurements was determined by Pearson correlation analysis, and the interobserver reliability was determined by the intraclass correlation coefficient (ICC). Pearson correlation analysis was also performed for patient age, height, weight and BMI. All P values are 2-sided, and the level of significance was set at P < .05.
Results
Patient weight, height, and BMI according to age group and stratified by sex are shown in Table 1. Regarding reviewer agreement of the MRI measurements, the Pearson correlation coefficient ranged from 0.70 to 0.98, indicating high intraobserver reliability, and the ICC was between 0.95 and 0.99, underscoring good to very good interobserver reliability.
Patients’ Body Measurements Overall and by Sex a

Data are reported as mean ± SD. BMI, body mass index. Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.
ACL and PCL Morphology
ACL length was found to be between 18 and 37 mm and ACL width between 4 and 6 mm for the full cohort (age, 0-18 years). ACL growth was not constant but always increased from one age group to another. PCL length ranged between 27 and 43 mm, while PCL width ranged between 7 and 9 mm. The PCL showed continuous growth for all age groups. Detailed results for the different age groups are shown in Tables 2 to 4 and Figures 7 to 9 (see Supplemental Material, available separately, for additional boxplots). Growth of the cruciate ligaments and the surrounding osseous tissue was found to be most pronounced between the ages of 4 and 12 years and was slowed down from age group 5 to 6. Correlations with size and weight were strong, while BMI correlated slightly with the measurements. Measurements in female patients were slightly larger on average than in their male counterparts between the ages of 0 and 6 years, while male patients tended to have larger values starting from ages 7 to 9. These values were significantly larger in male patients from the ages of 16 to 18 (P < .05).
ACL and PCL Measurements for the Total Cohort (N = 127) a

Data are reported as mean ± SD. ACL, anterior cruciate ligament; AP, anteroposterior; ML, mediolateral; PCL, posterior cruciate ligament. Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.
ACL and PCL Measurements for Female Patients (n = 67) a
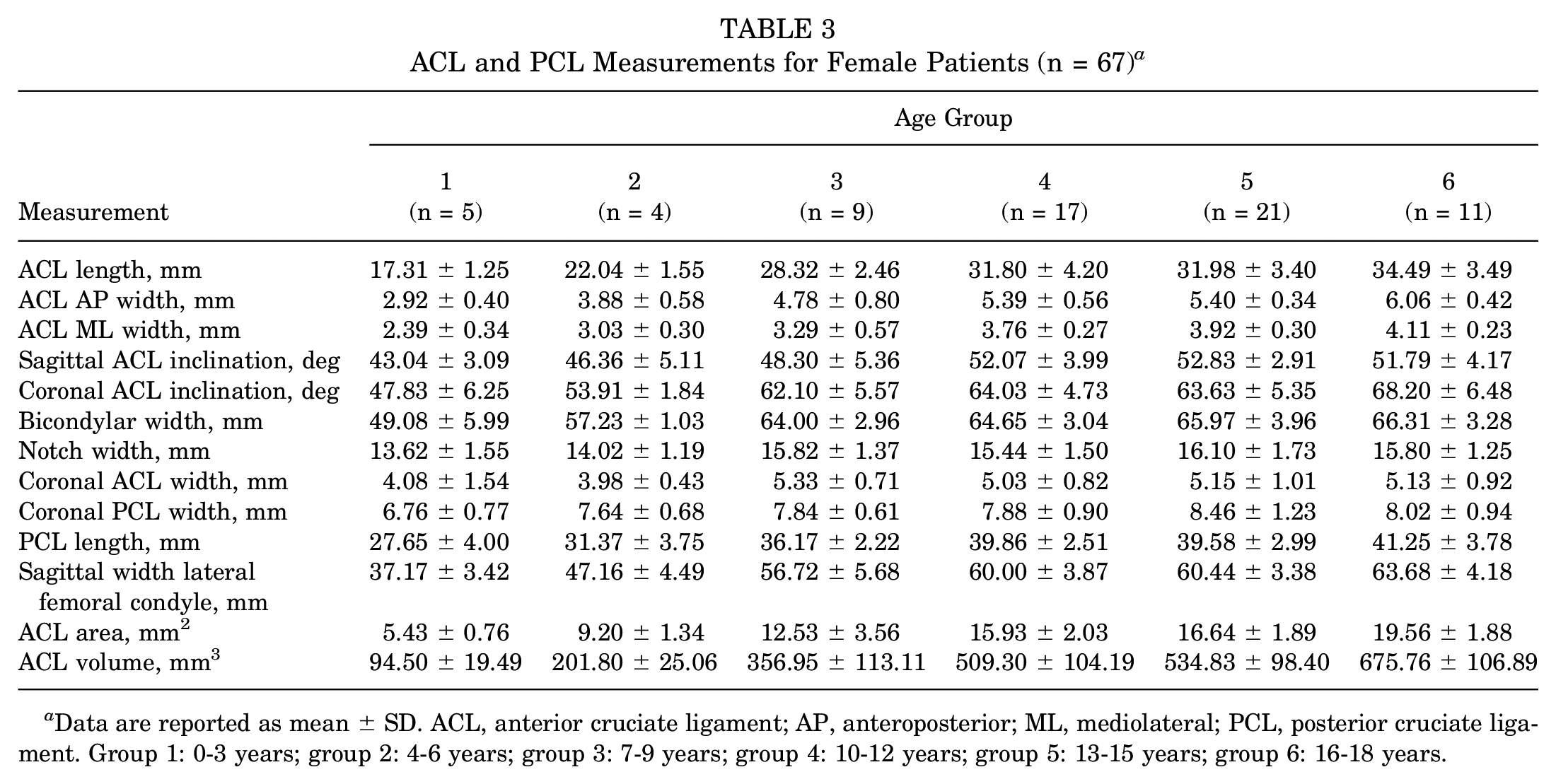
Data are reported as mean ± SD. ACL, anterior cruciate ligament; AP, anteroposterior; ML, mediolateral; PCL, posterior cruciate ligament. Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.
ACL and PCL Measurements for Male Patients (n = 60) a

Data are reported as mean ± SD. ACL, anterior cruciate ligament; AP, anteroposterior; ML, mediolateral; PCL, posterior cruciate ligament. Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.

Mean anterior cruciate ligament (ACL) length and coronal, sagittal, and transversal ACL width for age groups 1 to 6. The top and bottom of the box represent minimum and maximum values. The points represent the mean values. Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.

Mean posterior cruciate ligament (PCL) length and width for age groups 1 to 6 (points: mean value; box: minimum and maximum values). Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.

Mean bicondylar width and notch width for age groups 1 to 6 (points: mean value; box: minimum and maximum values). Group 1: 0-3 years; group 2: 4-6 years; group 3: 7-9 years; group 4: 10-12 years; group 5: 13-15 years; group 6: 16-18 years.
Discussion
This study provides normative data of the ACL and PCL in different age groups in children and adolescents by MRI, which is the basis for age-adapted and individualized ACLR and PCLR. ACL and PCL showed an inhomogeneous growth pattern in different pediatric age groups. Growth of the cruciate ligaments and the surrounding osseous tissue was found to be most pronounced between the ages of 4 and 12 years. Measurements of ACL and PCL morphology in female patients were slightly larger on average than in their male counterparts between the ages of 0 and 6 years, while male patients tended to have larger values starting from ages 7 to 9. The present study newly combines different measurement methods to depict a most precise image of the pediatric ACL and PCL morphology by MRI. Comparable data within the current literature, especially for morphology of the PCL in different age groups, are lacking. This gap is filled by the current study.
The results of this study regarding the ACL morphology were mainly comparable with those of Putur et al. 14 The ACL growth was found to be most distinct between the age groups 2 and 3 as well as 3 and 4 (age, 4-12 years). This is also largely consistent with the findings of Putur et al, but they described the highest growth rate per year as slightly earlier for patients aged 1.5 to 5.75 years, a decelerated growth at 11.75 years, and a growth stop at 18.5 years. This difference may be explained by the different methods used to determine growth. Putur et al analyzed 2 serial MRI examinations of the same knee and used an additional growth model to predict ACL growth over time. The present study found a growth stop in age group 6 (age, 16-18 years). The results in this age group were already comparable with those of adults 21 and, interestingly, they match with the quoted 38 mm for ACL length in the historical evaluation of cruciate sizes by Girgis et al in 1975. 7
Sex differences for ACL and PCL growth were observed in the present analysis. Female patients presented larger cruciate ligaments than male patients between the ages of 0 and 6 years. From ages 7 to 9, male patients had larger measurement values, and after stagnation of growth they presented significantly larger cruciate ligaments than their female counterparts. This was also shown by the results of Anderson et al 1 and Chandrashekar et al. 3 They studied sex-based differences in the geometry of the ACL, its morphologic characteristics, and the intercondylar notch size in adults.
Shaw and Finch 15 described the highest incidence rate for pediatric ACL injuries in children and adolescents as between 10 and 14 years of age. They analyzed a cohort of patients with ACL injury aged between 5 and 14 years. According to the results of this study, this time period partially presents accelerated growth of the ACL and intercondylar notch. It remains unclear if the increased growth rate of these structures implies an increased vulnerability of the ACL in this age group. In contrast, according to the study of Beck et al, 2 peak age of ACL injury is 16 years in female patients and 17 years in male patients. The abovementioned sex differences might be one factor that could explain the higher ACL injury rate in young female adolescents compared with their male counterparts. But as the etiology of ACL tears is mainly multifactorial, further studies are needed to verify this hypothesis.
In establishing individualized ACLR techniques in the pediatric population, the length and diameter of the ACL and its course through the intercondylar notch is crucial. Therefore, the ACL and notch inclination angles as well as the notch width might provide further information. The results of the present study showed an increasing ACL inclination angle and a progressively steeper notch ascent with age. This is in conformity with the findings of Lima et al 10 and Kim et al 9 and endorses the theory that an increase in verticalization of the ACL and intercondylar notch arises with age. Higher notch inclination angles were found to be a risk factor for ACL injuries in adults. 5 Although these findings cannot be directly transferred to the pediatric population, it might be a contributing co-factor for ACL injuries in adolescents. ACLR techniques that do not respect the physiological age-appropriate ACL inclination and notch inclination, due to imprecise femoral and/or tibial tunnel placement, might have an increased risk of graft failure. A recent meta-analysis of complications after pediatric ACLR showed a high retear rate of 8.7%. 20
Several studies have shown that narrow notch widths are associated with an increased risk of ACL injuries18,19 and that women have statistically significantly narrower notches than men. 17 In the current study, the notch width progressively enlarged with age and was correlated with weight and height of the patients but not with sex. Its greatest growth was found between age groups 2 and 3. The NWI was higher in male compared with female adolescents, especially in age group 6. Further studies are needed to properly analyze potentially pathological mismatches in ACL/PCL size and notch width in certain age groups that are correlated with an increased risk of ACL/PCL injuries. Normative values for intact knees of children and adolescents as seen in this paper may serve as a basis for these studies.
In addition, the results of this study might be clinically relevant as well as helpful for orthopaedic surgeons in choosing the appropriate ACL or PCL graft with suitable length and diameter for children and adolescents with ACL or PCL injuries or in revision cases depending on the planned reconstruction technique (transphyseal, all epiphyseal, or extraphyseal). The aim of all techniques is to avoid postoperative malalignment and leg-length discrepancy. 12
The clinical reality of ACLR and PCLR in children and adolescents is serious such that as growth takes over in a cruciate-reconstructed knee, the implanted graft grows along with the individual. In this context, a further clinical benefit might be to compare this normative data of ACL and PCL dimensions with postoperative MRI values of graft size and graft inclination in the same age group. This would allow for an evaluation of long-term consequences.
Limitations and Strengths
There are several limitations to this study. First, it was a retrospective analysis of preexisting MRI data sets. The results were limited to 127 MRI examinations. A larger number of MRI examinations for each age group might have enhanced the reliability of the results, especially for age group 1. Different MRI coils were used for this age group compared with the other age groups. This may have influenced the MRI image quality and limited the comparability of the measurements. The calculation of ACL area and volume was limited to a mathematical computation of simplified geometrical shapes that are not directly comparable with the complex anatomic ACL morphology. Furthermore, the MRI results cannot be directly transferred to the exact anatomic size in vivo. The MRI measurements might over- or underestimate the true anatomic structure size. Nonetheless, the MRI is routinely used in clinical practice to detect knee injuries and is the most reasonable option to measure the ACL and PCL size in children and adolescents due to the absence of radiation and the strictly limited feasibility of anatomic studies. The skeletal maturity of the patients was not gauged and the location of ACL and PCL attachments relative to other structures (eg, position of the center of the ACL footprint in the sagittal plane) were not measured.
The strength of this study is in creation of an extensive analysis of the ACL and PCL morphology by MRI in different pediatric age groups, adding relevant data to existing literature, especially with regard to the PCL of skeletally immature patients. The study combined several reliable MRI measurements of the ACL, PCL, and distal femur to depict a most precise image of the pediatric knee anatomy and its development.
Conclusion
This study provides normative MRI data on the morphology of pediatric anatomic features in the knee as a basis for age-appropriate and individualized surgical care of ACL and PCL injuries in children and adolescents.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231201642 – Supplemental material for Size and Morphology of the Anterior and Posterior Cruciate Ligaments at Different Pediatric Age Intervals: An MRI Analysis
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231201642 for Size and Morphology of the Anterior and Posterior Cruciate Ligaments at Different Pediatric Age Intervals: An MRI Analysis by Matthias Brockmeyer, Swen Norrick, Gudrun Wagenpfeil, Jonas Stroeder and Stefan Landgraeber in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted April 27, 2023; accepted May 19, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.