
Abstract
Background:
Children who participate in sports have reduced cardiovascular risk, obesity, and type 2 diabetes. However, sports participation also comes with an inherent risk of sports-related injuries.
Purpose:
To examine the efficacy of a school-based neuromuscular warm-up program (NWP) in reducing the risk of school sports injury (SSI) in children and the impact of different levels of compliance on the effectiveness of the program.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 421 students from grades 4 to 6 at a single school (age range, 9-14 years) were randomized by grade to an intervention group and a control group. The intervention group participated in a 13-week simplified (8-minute) NWP designed to reduce SSI risk. The control group participated in a standard warm-up of the same length and duration. Exposure, compliance, and injury data were collected via a weekly form. The primary injury outcome was all SSIs. Secondary outcomes included injuries from physical education (PE) and non-PE class, upper and lower extremity injuries, other location injuries, and time-loss injuries. A Poisson regression model using an intent-to-treat analysis was performed to estimate the incidence rate ratio (IRR) for all injuries in the intervention group compared with the control group. To examine the influence of level of compliance, we divided the intervention group into low compliance (participation 1-2 times/wk) and high compliance (participation >2 times/wk) then compared the difference on injury rates (IRs) between these groups and the control group.
Results:
There were significant differences between the intervention and control groups regarding all SSIs (IRR, 0.47; 95% CI, 0.23-0.96; P = .038), PE class injuries (IRR, 0.37; 95% CI, 0.14-0.99; P = .048), and other location injuries (IRR, 0.20; 95% CI, 0.05-0.82; P = .025). The compliance analysis revealed that although the low-compliance group was able to reduce the risk of SSIs (IR, 4.43; 95% CI, 2.49-6.37) compared with the control group (IR, 7.60; 95% CI, 5.61-9.59), the high-compliance group produced a better effect in reducing the SSI risk (IR, 1.80; 95% CI, 0.04-3.56).
Conclusion:
The simplified NWP used in this study was efficacious in the reduction of SSIs in children.
Registration:
ChiCTR2100043875 (Chinese Clinical Trial Registry; http://www.chictr.org.cn).
Participation in sports has many advantages for children and adolescents, including reducing cardiovascular risk factors, enhancing bone health, elevating mental health, 20 and reducing obesity and type 2 diabetes.9,18 However, participation in sports also comes with an inherent risk of sports-related injuries. 6 Although most sports injuries in children and adolescents are not life-threatening, they may result in direct pain, short-term disability, school absence, and long-term consequences, such as osteoarthritis in later life, 21 all of which leads to high direct and indirect costs. 1
In recent years, many researchers have found that school sports injury (SSI) is prevalent among children and adolescents.3,4,17,23,31 For example, findings from a survey of 2873 adolescents from 24 high schools in Calgary, Canada, showed that 94% of students participated in sports during the previous year. 12 The authors found that the incidence proportion was 40.2% for injuries requiring medical attention, 8.1% for injuries evaluated at a hospital emergency department, 49.9% for injuries resulting in time loss from sport, and 9.3% for injuries resulting in loss of consciousness. The greatest proportion of injuries occurred in basketball, hockey, soccer, and snowboarding, and the top 5 injury types were sprain, contusion, concussion, fracture, and muscle strain. 12
In December 2020, we investigated the incidence of SSI among children and adolescents from 3 kindergarten through 12th grade (K-12) schools in Shanghai, China. 7 The participating students (N = 1303) were in grades 4 to 5 of elementary school and grades 7 to 9 of middle school. Results calculated using a cluster random sampling method showed that the overall incidence of SSI was 29.5%, which was similar to the findings of investigations on SSI among middle school students in southern China. 5 Surprisingly, however, we found the risk of SSI to be higher among grades 4 to 5 elementary school students in the 3 participating schools (School A, 40.2%; School B, 35.1%; School C, 42.7%). 7 It would therefore be useful to have an effective injury prevention strategy in this population.
In our 2022 meta-analysis, 8 we found that a neuromuscular warm-up program (NWP) had the strongest effect among 3 warm-up programs in reducing SSI (incidence rate ratio [IRR] ranging from 0.30 to 0.54).15,22,26 Given this finding, we decided to adopt the NWP to prevent the occurrence of SSI in the current intervention trial. Typically, in previous studies, the participants in NWPs were mainly junior high/middle school students/athletes.11,15,22 So far, there is scarce research on the prevention of sports injuries among primary school students through an NWP. In addition, previous studies have also shown that compliance with intervention programs 27 is an important factor influencing the preventive effect on SSI. However, the relationship between the intervention and the level of compliance has rarely been discussed.
The purpose of this study was to examine the efficacy of a school-based NWP in reducing the risk of SSI in children and the impact of different compliance levels on the effect of the program.
Methods
Study Design and Participants
The study complied with ethical standards and the Declaration of Helsinki. The study protocol received ethics committee approval, and all participating children and their parents received information about the aim and the methodology of the project before the start of the study and provided written consent/assent. Participation was voluntary. In cases where participation was declined, the parents informed their children's physical education (PE) teachers, and those teachers notified us about the dropouts.
This study was designed as a 2-armed, cluster randomized controlled trial (RCT) according to the CONSORT (Consolidated Standards of Reporting Trials) statement guidelines. A foreign language school was selected from 3 K-12 schools in Shanghai, China (School C from our 2020 study 7 ), and this RCT was registered on the Chinese Clinical Trial Registry. Participating classes were randomized into an intervention and a control group. All students of the same class were randomized into the same group (clustered allocation, with the class serving as a cluster) to minimize the risk of contamination. Computer-generated cluster randomization was conducted by a single researcher (S.L.) who had no direct contact with the school or school officials and who was not involved in the intervention. Grades and number of participating classes per grade served as the strata for the randomization.
The observation period was from March 1 to June 18, 2021, including 2 weeks of preparation and 13 weeks of intervention. According to our 2020 investigation, 7 students in grades 4 to 6 of a single foreign language school in Shanghai sustained more frequent SSIs than their counterparts in grades 7 to 9, so these students were recruited to participate in the study. A total of 421 students from 12 classes in grades 4 to 6 (age range, 9-14 years) were enrolled for this trial by a single author (L.D.). PE classes in Shanghai are compulsory at 120 minutes per week in elementary schools. Classes usually meet 3 times per week, and students are also able to participate in other school sports activities, such as activity class, morning exercise, and recess. Our inclusion criteria for the trial were students who (1) were in good health; (2) did not sustain any SSI in the past month; and (3) had no history of systemic disease (eg, cancer, arthritis, heart disease, etc) or neurologic disorder (eg, head injury, cerebral palsy, etc). Our exclusion criteria were students who (1) were unable to participate in normal sports activities and/or (2) did not agree to engage in the study.
Sample Size Calculation
The sample size calculation was based on an expected difference of 50% in the injury rate (IR)22,26 between the intervention (IR, 4.0) and control groups (IR, 8.0). The total exposure time of every student in the 13-week trial was about 30 hours (PE and non-PE class activities), adjusted by an expected dropout rate of 1% and a coefficient of 1.2 for the cluster RCT design. Assuming a type 1 error of .05 and type 2 error of 0.20, a minimum of 402 students (201 per study group) was calculated to detect a reduction in the risk of injury.
NWP (Intervention)
Our intervention adapted the 15-minute NWP designed by the Sport Injury Prevention Research Center at the University of Calgary, Canada, which has been employed by researchers of school-based sport injury prevention and has produced satisfactory efficacy.14,15,26 However, we had to consider its feasibility when using a foreign intervention program to prevent SSIs in Chinese PE classes. In China, PE classes in elementary or middle schools usually last 35 to 40 minutes. If our NWP were to last 15 minutes, it would be impossible for PE teachers to teach students more skills and complete their teaching tasks in the PE class. Therefore, we decided to shorten the intervention program to 7.5 to 8 minutes at the beginning of the PE classes. We chose to keep its original structure but reduce the movements and repetitions of every component. Our simplified NWP included 13 movements, 8 of which were aerobic exercises, 4 of which were strengthening exercises, and 1 of which was a balance exercise (Table 1).
The control group used a standard warm-up (including running and stretching only) of the same duration. Because there is only 1 PE teacher for each grade, the class content after the warm-up was the same for the intervention group and the control group in each grade. Both the intervention and the control programs lasted 13 weeks.
Simplified Neuromuscular Warm-up Program Used in This Study (7.5-8 min/Session for 13 Weeks)
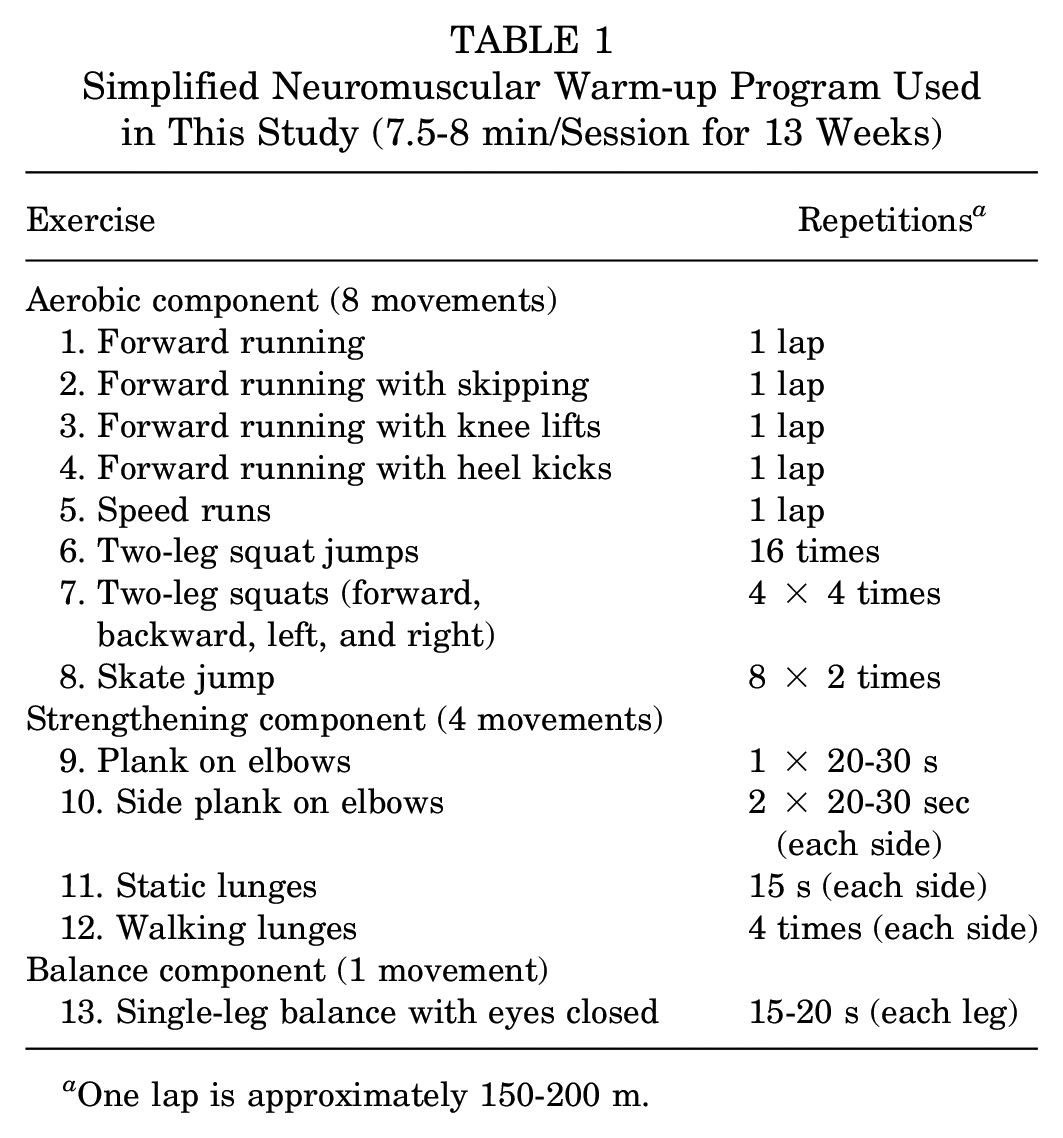
One lap is approximately 150-200 m.
Outcome Measures
The primary injury outcome was all SSIs. Secondary outcomes included PE class injuries, non-PE classes injuries, upper extremity injuries, lower extremity injuries, other location injuries, and time-loss injury. The definition of SSI, adapted from previous studies of sport injuries in children and adolescents,10,26 was any physical injury (eg, contusion, sprain, fracture) sustained during PE class, extracurricular sports activities, extracurricular sport training sessions, or extracurricular sport games at school that resulted in ≥1 of the following conditions: (1) a break in the current activity, (2) inability to (fully) participate in the next planned activity, (3) absence from school the next day, and/or (4) medical attention (ranging from first aid to hospitalization). 24 In addition, if an injury occurred during the NWP, it was reported as an adverse event.
Before the start of the study, a workshop was conducted to inform the PE teachers of both the intervention and the control programs about the aims and procedures of the study, which provided detailed instructions and practical application on the intervention program and the control program. The workshop lasted 2.5 hours and included a video outlining the warm-up components, practice time, and group discussions for action planning to address potential barriers to the program. To achieve blinding, the PE teachers were only told to practice the intervention program or the control program in their classes. At the beginning of the trial, every intervention class selected a student to demonstrate the NWP. All the selected students were trained in how to lead the NWP and rehearsed beforehand to ensure that they executed our intervention programs strictly with no misunderstanding of the program.
Every week, the PE teachers in each class recorded the exposure time of school sports activities, any injuries, and compliance with the intervention or control program for all students on a weekly school sport participation form (Appendix Figure A1). The teachers then completed an injury report form that was available on an online survey platform (Wenjuanxing website; www.wjx.cn) by scanning a QR code on a poster (Appendix Figure A2). A single researcher (L.D.) visited each class weekly to inquire about any injury during the week and to supplement the injury records, thereby minimizing the probability of recall bias and reporting bias.
The intensity of exercise was measured by a Suunto heart rate (HR) monitor (model t6c; Suunto Electro Oy 2) in a subgroup of 42 students (age range, 11-13 years) selected at random from the participants. The students were randomized to an intervention group (n = 19) or a control group (n = 23) and asked to execute either the NWP or the standard warm-up according to their allocation. During the routines, the HR (in beats per minute [bpm]) was recorded by the monitor to measure the intensity of the exercise. Both the maximum and the mean HR and the time spent at >75% maximum HR (in minutes; calculated as 0.75[220 –student age]) were measured during the middle of our cluster RCT.
Statistical Analysis
The maximum and mean HR and time spent at >75% maximum HR were compared as mean differences and related 95% CIs between the intervention and control groups using Student t tests. To determine the efficacy of the simplified NWP in reducing the risk of SSI, a comparison of the IR (number of injuries per 1000 sport participation hours) between the intervention and control groups was conducted based on the IRR. A modified intention-to-treat multivariate Poisson regression analysis (with school sport hours included as an offset and adjustment for clustering by class and important covariates [eg, sex, body mass index) was used to estimate the IRR for all injuries in the intervention group compared with the control group. To examine the influence on SSI of compliance with the intervention program, we divided compliance level into low (participation 1-2 times/wk) and high (participation >2 times/wk), then compared the difference on IRs and related 95% CIs between the control group and the 2 compliance groups. STATA 15.0 (StataCorp) was used to complete all data analyses. The threshold for statistical significance was set at P < .05.
Results
Descriptive Statistics
A total of 421 students from 3 grades and 12 classes participated in this study. Of these participants, 210 students from 6 classes (112 male, 98 female) were in the final intervention group and 209 students from 6 classes (116 male, 93 female) were in the final control group. Figure 1 outlines school recruitment, allocation of participants, and dropouts according to group. The dropout rates were 0.47% (1/211) for the intervention group and 0.48% (1/210) for the control group. Table 2 shows all baseline characteristics, which indicated no significant differences between the intervention and control groups.
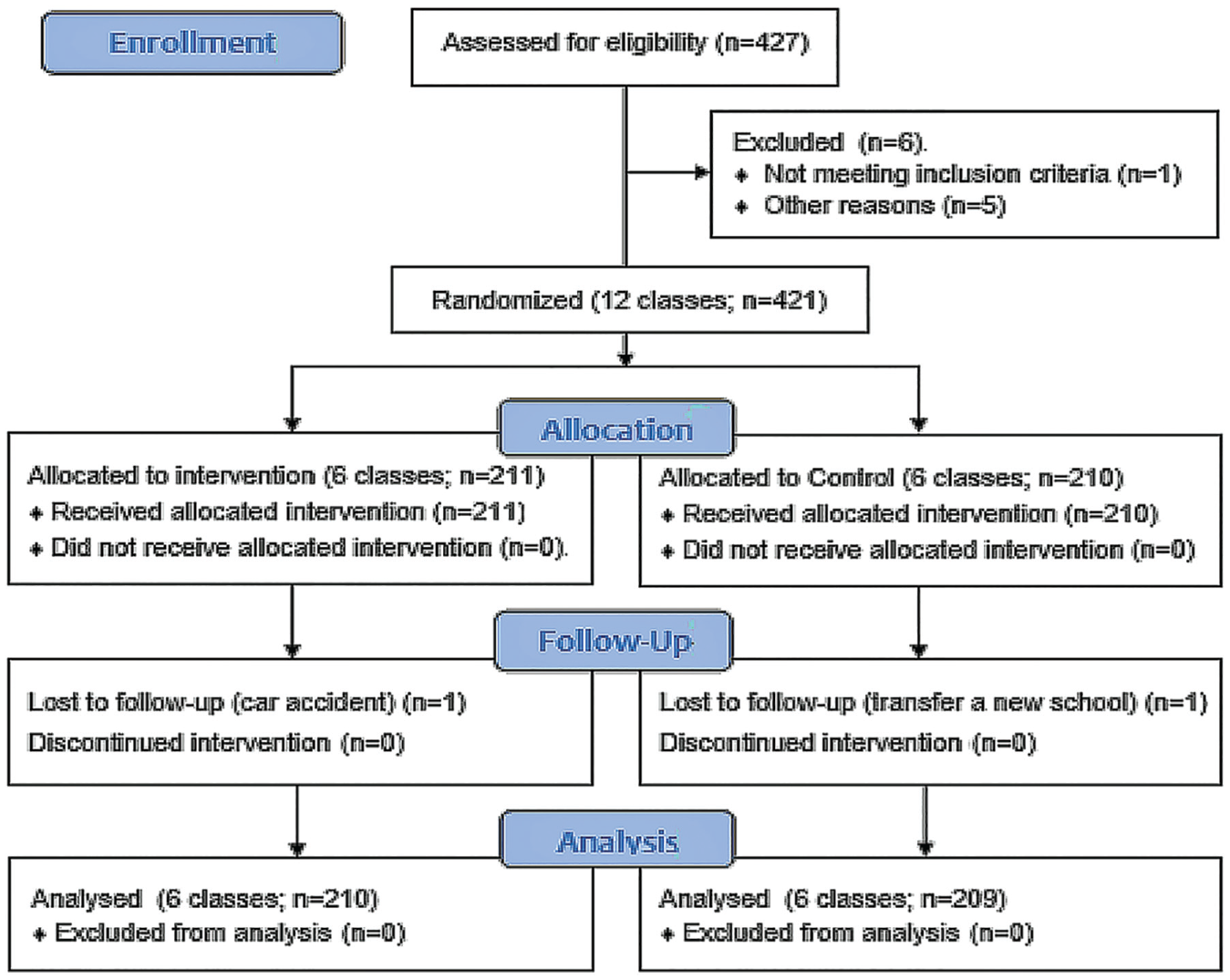
Flowchart of participant enrollment.
Baseline Participant Characteristics Between the Intervention and Control Groups a

Data are shown as n (%) or mean ± SD.
A total of 80 sport-related injuries were reported overall, including multiple injuries (in the intervention group, 1 student had 3 injuries; in the control group, 9 students had 2 injuries and 2 students had 3 injuries). A total of 24 sport injuries (n = 22) occurred in the intervention group and 56 sport injuries (n = 43) occurred in the control group. Compared with the control group, the intervention group demonstrated a significantly higher mean HR (mean difference, 13.4 bpm [95% CI, 4.1-22.6 bpm]; P = .006), and more time spent at >75% maximum HR (mean difference, 2.2 minutes [95% CI, 1.2-3.2 minutes]; P < .001) (Table 3).
Subgroup Comparison of HR Estimates Between the Intervention and Control Groups a
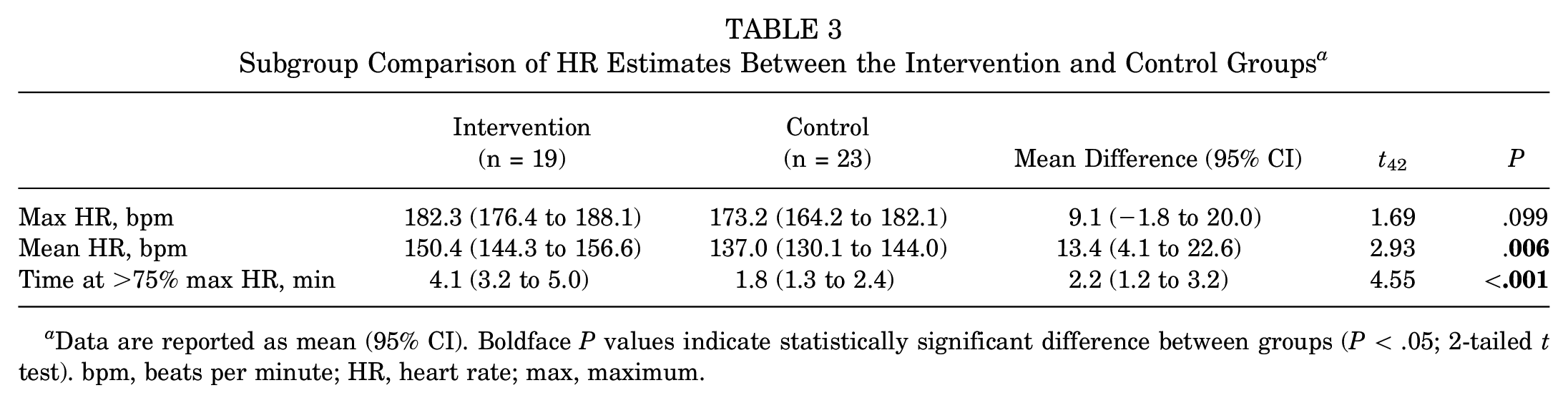
Data are reported as mean (95% CI). Boldface P values indicate statistically significant difference between groups (P < .05; 2-tailed t test). bpm, beats per minute; HR, heart rate; max, maximum.
Analysis of SSIs
Table 4 outlines the number of injuries, total hours of school sports, and IRs in both the intervention and control groups. Lower extremity injuries represented the greatest proportion of injuries occurring in both the intervention group (14/24; 58.3%) and the control group (29/56; 51.8%). The overall IR was 3.56 (95% CI, 2.14-4.99) in the intervention group and 7.60 (95% CI, 5.61-9.59) in the control group. The IR of PE classes in the intervention group was 1.78 (95% CI, 0.77-2.79) and 4.88 (95% CI, 3.29-6.48) in the control group, respectively.
IRRs by Injury Type Based on Poisson Regression Analysis Adjusted for Cluster and Covariate a
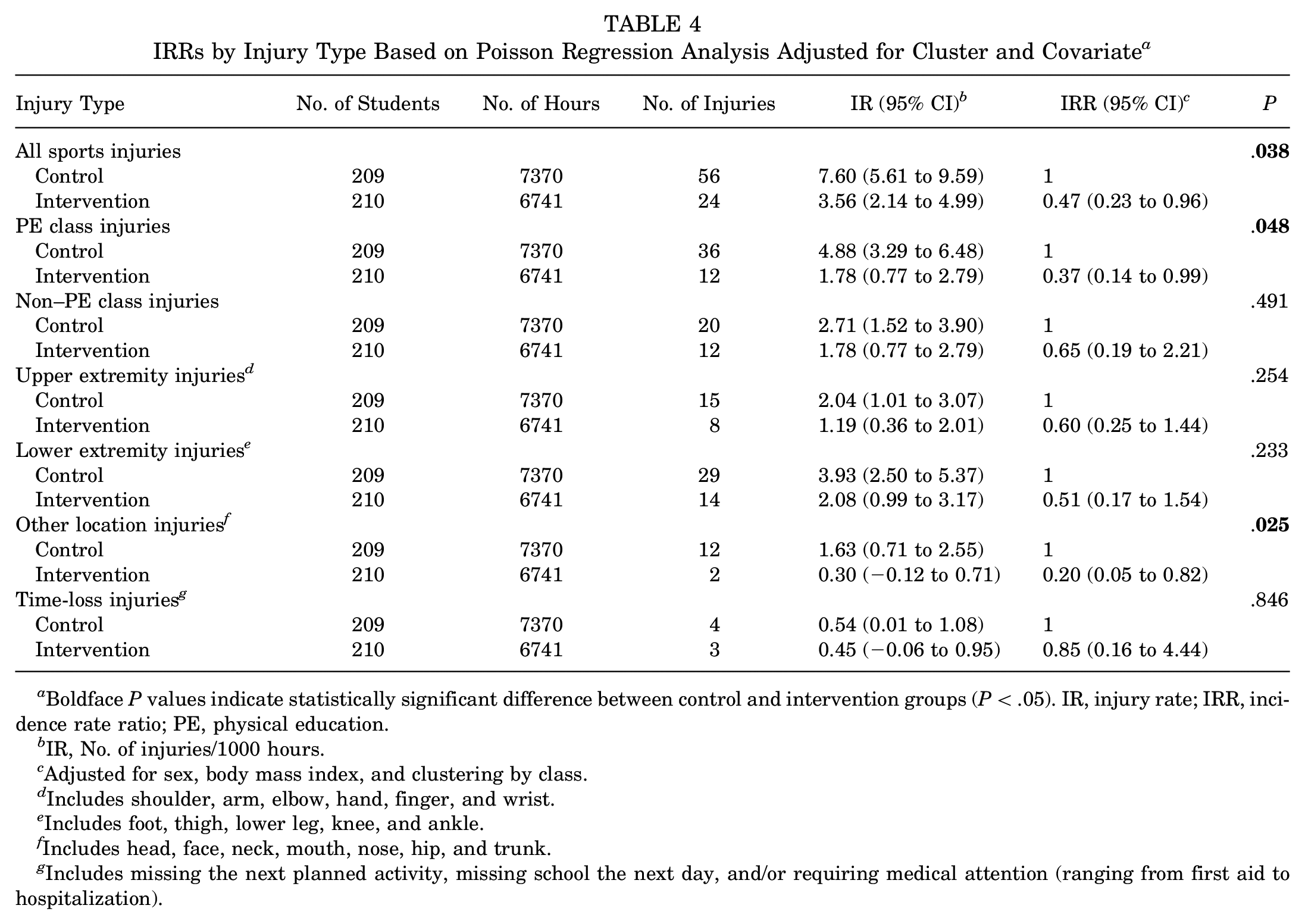
Boldface P values indicate statistically significant difference between control and intervention groups (P < .05). IR, injury rate; IRR, incidence rate ratio; PE, physical education.
IR, No. of injuries/1000 hours.
Adjusted for sex, body mass index, and clustering by class.
Includes shoulder, arm, elbow, hand, finger, and wrist.
Includes foot, thigh, lower leg, knee, and ankle.
Includes head, face, neck, mouth, nose, hip, and trunk.
Includes missing the next planned activity, missing school the next day, and/or requiring medical attention (ranging from first aid to hospitalization).
The Poisson regression model (adjusting for sex, body mass index, and clustering by class using total hours of school sport participation as an offset) demonstrated that the NWP was protective of all sports injuries (IRR, 0.47; 95% CI, 0.23-0.96), PE class injuries (IRR, 0.37; 95% CI, 0.14-0.99), and other location injuries (IRR, 0.20; 95% CI, 0.05-0.82). Though not statistically significant, the point estimate suggested a protective effect of simplified NWP in reducing the risk of non–PE class injuries, upper extremity injuries, lower extremity injuries, and time-loss injuries (IRR, 0.51-0.85).
Compliance Analysis
Injury incidence decreased with the increasing utilization rate of the NWP. The risk of injury was lower in both the high- and the low-compliance groups compared with the control group. The compliance analysis revealed that 1 to 2 times each week of intervention in PE classes was able to reduce the risk of SSI (IR, 4.43; 95% CI, 2.49-6.37) compared with the control group (IR, 7.60; 95% CI, 5.61-9.59), but only >2 times each week of intervention in PE classes produced a better effect in reducing the SSI (IR, 1.80; 95% CI, 0.04-3.56). The risk of injury in the high-compliance group was lower by more than half compared with the low-compliance group (Table 5).
Comparison of IR in the Low- and High-Compliance Groups Versus the Control Group a

The low-compliance group followed the NWP a mean 1 to 2 times per week, and the high-compliance group followed the NWP a mean of >2 times per week. IR, injury rate (No. of injuries/1000 hours); NWP, neuromuscular warm-up program; NA, not applicable.
Discussion
This study demonstrated a decreased risk of SSI in the intervention group, compared with controls, over a 13-week study period. For our intervention, we adapted an NWP that targeted modifiable intrinsic risk factors (eg, strength, endurance, and balance) to achieve the purpose of decreasing the risk of SSI.13,29 This is our first pilot RCT to examine the efficacy of a simplified NWP in elementary school students.
Sport Injury Prevention
The study indicated that the NWP could reduce the risk of all SSIs by 53%, PE class injuries by 63%, and other location injuries by 80%. The reduced risk of all SSIs found in this study is consistent with that in other studies examining similar prevention programs.16,22,26 In the previous studies, researchers found that the NWPs including strength, balance, aerobic, and agility components can reduce the risk of musculoskeletal injuries ≥35% in team sport and other youth sport settings. 13
However, the previous school-based intervention studies of sport injuries did not demonstrate the specific effect on PE classes.15,26 In addition, little research exists on the intervention effect of upper extremities and other locations (eg, head, face, neck, mouth, nose, etc) sport injuries resulting from the NWP.11,15,22,26 In the previous studies, the NWP was usually used to reduce the incidence of lower extremity injuries.22,25,30,32 Findings from a systematic review and meta-analysis showed that NWP can reduce the risk of lower extremity injuries by 36% (IRR, 0.64; 95% CI, 0.49-0.84; P < .01) and the risk of knee injuries by 24% (IRR, 0.74; 95% CI, 0.51-1.07; P > .05). In contrast, our trial indicates that the NWP has the same protective effect on lower extremity injuries (IRR, 0.51; 95% CI, 0.17-1.54), although this finding was not statistically significant (P = .233).
This study demonstrated that the warm-up program is effective in preventing injuries for the PE session right after the warm-up. This study does not serve to indicate the 8-minute warm-up program significantly affected exercise sessions performed after a certain time interval from the warm-up. Further research is needed to address the effectiveness in injury prevention when there is a measured time gap between the warm-up and the physical activity.
Intervention Effects and Compliance
Warm-up is a series of physical exercises performed before a more vigorous exercise. 2 From the perspective of our trial result, there is no doubt that the school-based NWP is an effective warm-up, which can increase participants’ HR and sweat with ease. Some research has indicated that the ideal intensity of the warm-up is debatable, but the consensus seems to lie with a mild sweat without fatigue. 28
Our trial results showed that NWP interventions were also protective against non–PE class injuries, upper extremity injuries, lower extremity injuries, and time-loss injuries (IRR, 0.51-0.85); however, the difference between the intervention and control groups was not significant, and the 95% CIs of the IRR for those injuries exceeded 1. This result showed that the mean value of the intervention effect of the neuromuscular warm-up on these types of sports injuries had decreased significantly, but the variance was large, so the difference between 2 groups did not meet conventional levels of statistical significance. There are 2 possible reasons for this result: insufficient sample size and unstable intervention effect. Therefore, in future studies it is necessary to collect more samples and to improve the stability of the intervention effect through the improvement of compliance, so as to further verify the effect of the intervention program.
In addition, time-loss injuries reflect the severity of the injury. From the results of the study, there were only 7 cases of children's time-loss injuries (3 cases in the intervention group and 4 cases in the control group), which were mainly abrasions, bruises, and sprains but no strains, fractures, and dislocations, and so forth. This was mainly related to the age (range: 8-13 years) of primary school students. Usually, the sports that primary school students participate in are much less intense and dangerous than those of middle school students, and dangerous apparatus sports (such as parallel bars and horizontal bar) are rarely practiced among primary school students, so the proportion of time-loss injuries we observed in this trial was lower than in the middle school student population in related studies. 26
The compliance analysis demonstrated that compared with the controls, NWP intervention once or twice a week was able to decrease the IR to 4.43 (95% CI, 2.49-6.37), while compliance of >2 times of NWP intervention per week decreased the IR significantly (IR, 1.80; 95% CI, 0.04-3.56). Hislop et al found a similar result, demonstrating a protective effect of the intervention program in youth rugby players when exercises were performed ≥3 times per week (IRR, 0.28; 95% CI, 0.14-0.51). 19 Both studies showed that with the increase of weekly intervention frequency, the incidence of sports injury continues to decrease. In general, >2 times of intervention per week can achieve the desirable effects in sports injury prevention.
Strengths and Limitations
The strengths of our study are that (1) the participants in this trial were students in grades 4 to 6 of primary school, of a younger age than participants of previous studies (junior high/middle school students); (2) in this trial, no adverse events occurred because of students’ participation in the NWP, which demonstrated that the simplified NWP is safe as well as feasible; and (3) we used prospective longitudinal data in the cluster RCT to analyze the effect from the intervention of NWP, compensating for the shortcomings in our previous observational research. 7
There also exist several limitations in this trial. First, due to the limited scientific research funds, the researchers were unable to buy enough HR monitors. Therefore, 42 students (22 boys and 20 girls) were randomly selected from the total participants and divided into an intervention group and a control group to test the difference in exercise intensity between the NWP and standard warm-up groups through limited HR monitors. Second, our NWP had not been included in the school PE curriculum, so the compliance of the NWPs cannot be guaranteed, which also weakens the intervention effect of NWP on the reduction of SSI. Third, due to limited time and research funding, the present study focused on the school with the highest injury proportion and primary school students at higher risk of SSI among those schools and participants in the previous investigation in our cluster RCT. Fourth, we found that the protective effect of simplified NWP in reducing the risk of non–PE class injuries, upper extremity injuries, lower extremity injuries, and time-loss injuries might be influenced by our small sample size, which resulted in a non–statistically significant intervention effect (P > .05). Future studies should adopt a multicenter trial design to further validate the intervention effect of the simplified NWP through a larger sample trial. Finally, in the section of sample size calculation in this paper, we only calculated the power between the intervention group and control group. We did not separate the intervention group into high-compliance and low-compliance groups because we were not sure about the status of participants’ compliance in the intervention group at the beginning of the trial.
Conclusion
Although the NWP in the study was shortened into a half duration compared with its original one, the simplified NWP was still efficacious in the reduction of SSI among children, and it is suggested to utilize the NWP >2 times per week to achieve the desirable effects in sports injury prevention.
Footnotes
Appendix
Acknowledgements
The authors thank all students, parents, teachers, and officials at School C of Shanghai for participating in this research. The authors appreciate Professor Ping Xiang at Texas A&M University for her feedback and suggestions for the revision of the manuscript. In addition, the authors appreciate the Physical Education College of Shanghai Normal University for providing them with the Suunto heart rate monitors used in the study.
Final revision submitted April 3, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was provided by the Educational Science Planning Office of Shanghai (research funds C2-2020050). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Shanghai Normal University (approval No. [2020] 35).