
Abstract
Background:
Identifying risk factors for an infection after anterior cruciate ligament reconstruction (ACLR) and following targeted preventive strategies can effectively reduce this potentially serious complication.
Purpose:
To perform a systematic review and meta-analysis to identify the risk factors for an infection after ACLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PubMed, Embase, and Web of Science databases were searched from inception to September 1, 2022, for prospective and retrospective studies investigating risk factors for any type of infection after ACLR. Odds ratios (ORs) or mean differences were calculated for potential risk factors if ≥2 studies assessed the same risk factor. A qualitative analysis of variables was performed if a meta-analysis could not be conducted.
Results:
A total of 17 studies with 141,991 patients were included in this review. The overall pooled infection rate was 0.86% (range, 0.24%-5.50%). There were 20 risk factors identified for analysis. Of these, 7 variables independently increased the odds of an infection after ACLR: (1) male sex (OR, 1.90 [95% CI, 1.33-2.73]), (2) diabetes (OR, 2.69 [95% CI, 1.66-4.35]), (3) hamstring tendon autograft (OR, 2.51 [95% CI, 2.03-3.10]), (4) revision ACLR (OR, 2.31 [95% CI, 1.22-4.37]), (5) professional athlete status (OR, 6.21 [95% CI, 1.03-37.38]), (6) lateral tenodesis (OR, 3.45 [95% CI, 1.63-7.28]), and (7) corticosteroid use (OR, 7.83 [95% CI, 3.68-16.63]). No significant associations were found between postoperative infections and age, body mass index, smoking, meniscal repair, or outpatient surgery.
Conclusion:
This review revealed that an increased risk of infections after ACLR was associated with male sex, diabetes, hamstring tendon autograft, revision surgery, professional athlete status, lateral tenodesis, and steroid use. Knowledge of the risk factors associated with an infection after ACLR may facilitate the identification of high-risk cases and the implementation of preventive measures to mitigate the serious consequences of this complication.
An infection (including superficial wound infections and septic arthritis) after anterior cruciate ligament reconstruction (ACLR) is a rare but devastating complication, with a reported incidence of 0.28% to 1%.7,9,51 It can result in prolonged rehabilitation, functional deficits, arthrofibrosis, and often the need for repeated surgery.37,42,59 The treatment of joint infections after ACLR usually requires arthroscopic debridement combined with intravenous antibiotics and on occasion requires graft removal.11,63 Infection-induced prolongation of an illness and escalation of treatment costs not only impose a significant burden on patients and their families but also exert additional pressure on the health care system. Therefore, it is critical to determine which factors put patients at a greater risk of a postoperative infection, especially those that can be modified to minimize the hazard of such serious events.
Numerous previous studies have investigated the risk factors associated with an infection after ACLR, such as sex,44,51 high body mass index (BMI), 29 diabetes, 9 tobacco use,12,51 being a professional athlete, 57 and hamstring tendon (HT) autografts.6,31 However, some studies have also found that smoking, diabetes, and being a professional athlete do not increase the risk of infections in patients after ACLR.8,9,64 Given the range of risk factors, inconsistent findings, limited sample sizes, and single institution–based cohorts in numerous studies, further research is warranted.
The purpose of the current study was to perform a systematic review and meta-analysis of risk factors associated with an infection after ACLR and to help develop effective preventive management strategies for this complication.
Methods
We performed and conducted this review with a meta-analysis according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 41 The study protocol was preregistered at PROSPERO before starting this review (registration No. CRD42022360506).
Literature Search
PubMed, Embase, and Web of Science were searched for any relevant studies published before September 1, 2022. The following terms were used for the search: “risk,”“associated with,”“anterior cruciate ligament,”“infection,” and “septic arthritis.”Appendix Table A1 shows the search strategy for each database. In addition, the gray literature and databases of unpublished studies were also examined, and the reference lists of all included studies were hand searched for potentially eligible studies. There was no restriction on the publication date. Overall, 2 reviewers (L.Z. and R.Y.) independently screened the studies identified in the search. Any discrepancies were resolved by a consensus between the reviewers.
Inclusion criteria were as follows: (1) cohort studies, case-control studies, or cross-sectional studies; (2) cases and controls defined according to the presence or absence of infections after ACLR, respectively; (3) studies that reported at least 1 risk factor for any type of infection (superficial wound infection, septic arthritis, etc) after ACLR; and (4) valid data presented to estimate odds ratios (ORs) or mean differences (MDs) with 95% confidence intervals (CIs). Exclusion criteria were as follows: (1) case reports, conferences, commentaries, and reviews; (2) articles written in a language other than English; (3) nonclinical studies (eg, cadaveric studies, animal studies, and basic science articles); and (4) patients undergoing ACLR with concomitant open surgery or an additional ligament reconstruction procedure (eg, medial collateral ligament, lateral collateral ligament). There was no minimum follow-up time limit because an infection could theoretically occur at any time after ACLR. If several studies focused on the same group of patients, the most recent data containing more samples were used for analysis. Risk factors were defined as any variables potentially associated with an infection after ACLR, including sociodemographic factors, intraoperative factors, and activity level.
Quality Assessment
The Methodological Index for Non-Randomized Studies (MINORS) 23 checklist was used to evaluate the quality of all included studies. The 12 items of the MINORS questionnaire were scored as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with a maximum score of 16 for noncomparative studies and 24 for comparative studies. The methodological quality was assessed according to the MINORS score for noncomparative studies as very low (0-5), low (6-10), fair (11-15), and good (16). Again, 2 reviewers (L.Z. and R.Y.) independently evaluated the included studies, and any discrepancies between the reviewers were resolved by a consensus.
Data Extraction and Synthesis
After identifying all eligible studies, the same 2 reviewers independently evaluated each study, extracted data, and cross-checked the data. The country, number of cases and controls, and risk factors evaluated were extracted from the studies. Any disagreements were resolved by a discussion between the 2 reviewers. We synthesized the risk factors associated with an infection after ACLR as examined in the enrolled studies, conducting a meta-analysis when ≥2 studies reported on a given risk factor and performing a qualitative analysis when only 1 study addressed a particular risk factor. If risk factors were used to match cohorts in a 1-to-1 ratio by exact values, they were not included in the meta-analysis. In addition, considering the many risk factors that may affect the incidence of infections after ACLR, adjusted effect estimates in multivariate analyses were preferred over unadjusted effect estimates because they were closer to the actual effects. In multivariate analyses, adjusting for other variables can help to reduce bias and confounding in estimating the effect of a particular variable on the outcome of interest.
Statistical Analysis
Dichotomous outcomes were reported as ORs with 95% CIs, while continuous outcomes were reported as MDs with 95% CIs. The I2 statistic was used to estimate heterogeneity. I2 > 50% indicated high heterogeneity; a random-effects model was then used. Otherwise, a fixed-effects model was applied. P < .05 was considered statistically significant. If there was high heterogeneity between studies, we conducted a sensitivity analysis by removing individual studies one by one to explore the source of heterogeneity. Review Manager (Version 5.3; Cochrane Collaboration) was used to analyze all extracted data.
We classified the risk factors according to the OR as having strong, moderate, minimal, or marginal to no evidence. Risk factors with strong evidence doubled the risk for an infection after ACLR compared with baseline (OR > 2.0), or had a strong protective effect (OR < 0.8), and were significant. Risk factors with moderate evidence had an OR between 1.5 and 2.0, or between 0.8 and 0.9 if protective, and were significant (P < .05). Risk factors with minimal evidence had an OR between 1.0 and 1.5, or between 0.9 and 1.0 if protective, and were significant. Risk factors with marginal to no evidence had a nonsignificant OR (P > .05) or presented no plausible explanation for being a risk factor for infections after ACLR. These criteria have been used in previously published studies.33,55
Results
The initial search strategy generated a total of 834 studies across PubMed, Embase, and Web of Science. Another study 32 was found through a manual search of the reference lists of the included studies. After removing 249 duplicate studies, the remaining studies were screened according to their titles and abstracts. The full text of 55 studies was considered for screening, 38 studies that did not meet the inclusion criteria were excluded, and 17 studies ‡ were ultimately included in the meta-analysis (Figure 1).

Flowchart of the study inclusion process.
Characteristics of Included Studies
The 17 eligible studies involved a total of 141,991 patients, consisting of 1223 cases and 140,768 controls (overall incidence of 0.86%). Table 1 shows the characteristics of all included studies. There were 8 case-control studies (47.1%), 1 case series (5.9%), and 8 retrospective cohort studies (47.1%). There were 11 studies that were conducted in the United States, 5 in Europe, and 1 in Japan. The infection rate after ACLR in this review was similar to rates previously reported in the literature.54,58,62 Additionally, 4 studies27,29,39,64 reported all types of infections but with deep surgical site infections (SSIs) and superficial SSIs described separately, 10 studies § only included septic arthritis, and 3 studies9,12,16 reported all types of infections together. The publication year of the included articles ranged from 2005 to 2022.
Characteristics of Included Studies a
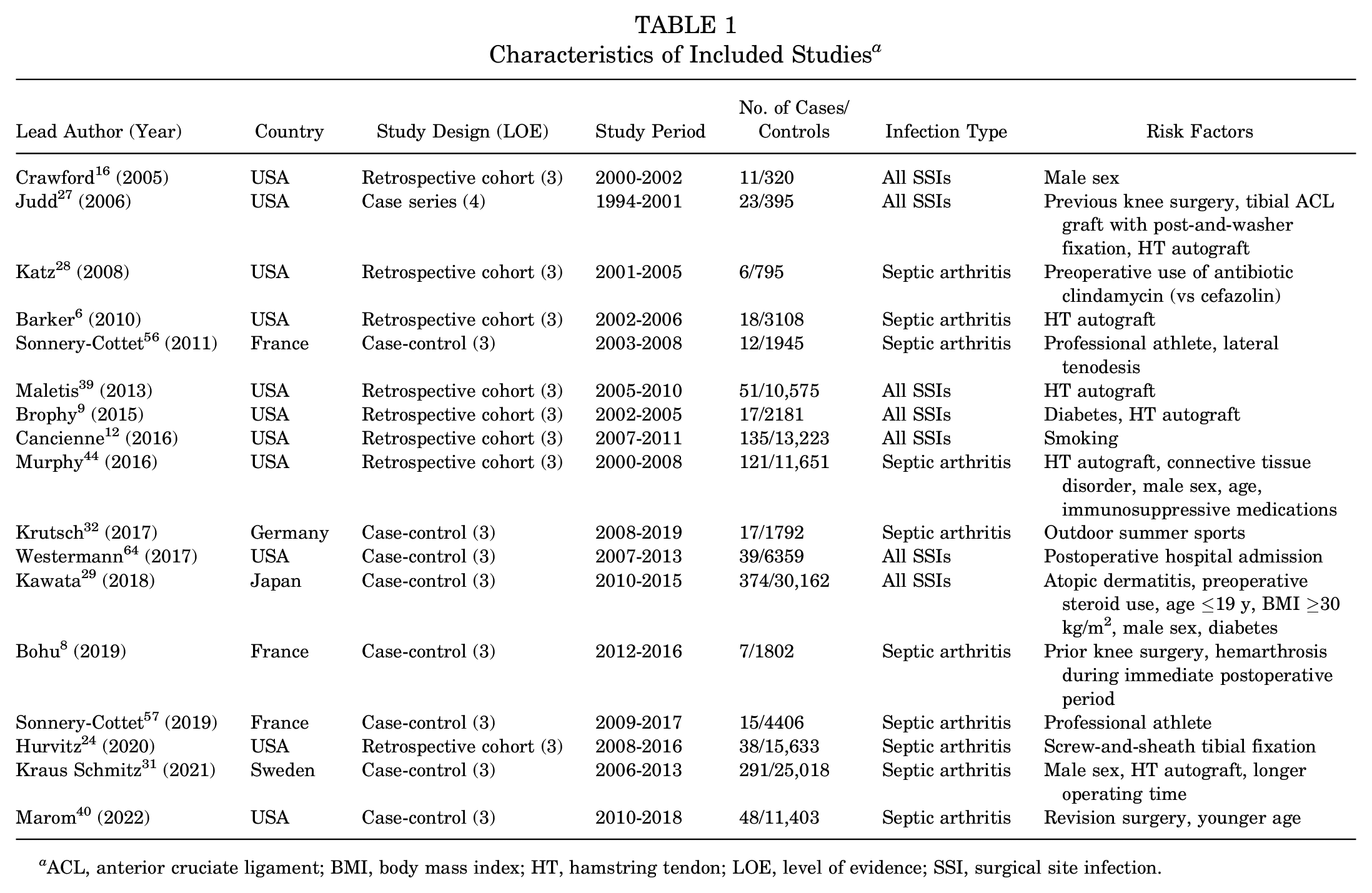
ACL, anterior cruciate ligament; BMI, body mass index; HT, hamstring tendon; LOE, level of evidence; SSI, surgical site infection.
Quality Assessment
The results of the methodological quality assessment using the MINORS score are summarized in Appendix Table A2. The mean MINORS score was 17.29 ± 2.11 among all studies. The mean MINORS score of the 16 comparative studies was 17.75 ± 1.10 of 24, and the mean MINORS score for the 1 noncomparative study 27 was 10 of 16.
Risk Factors for Infection After ACLR
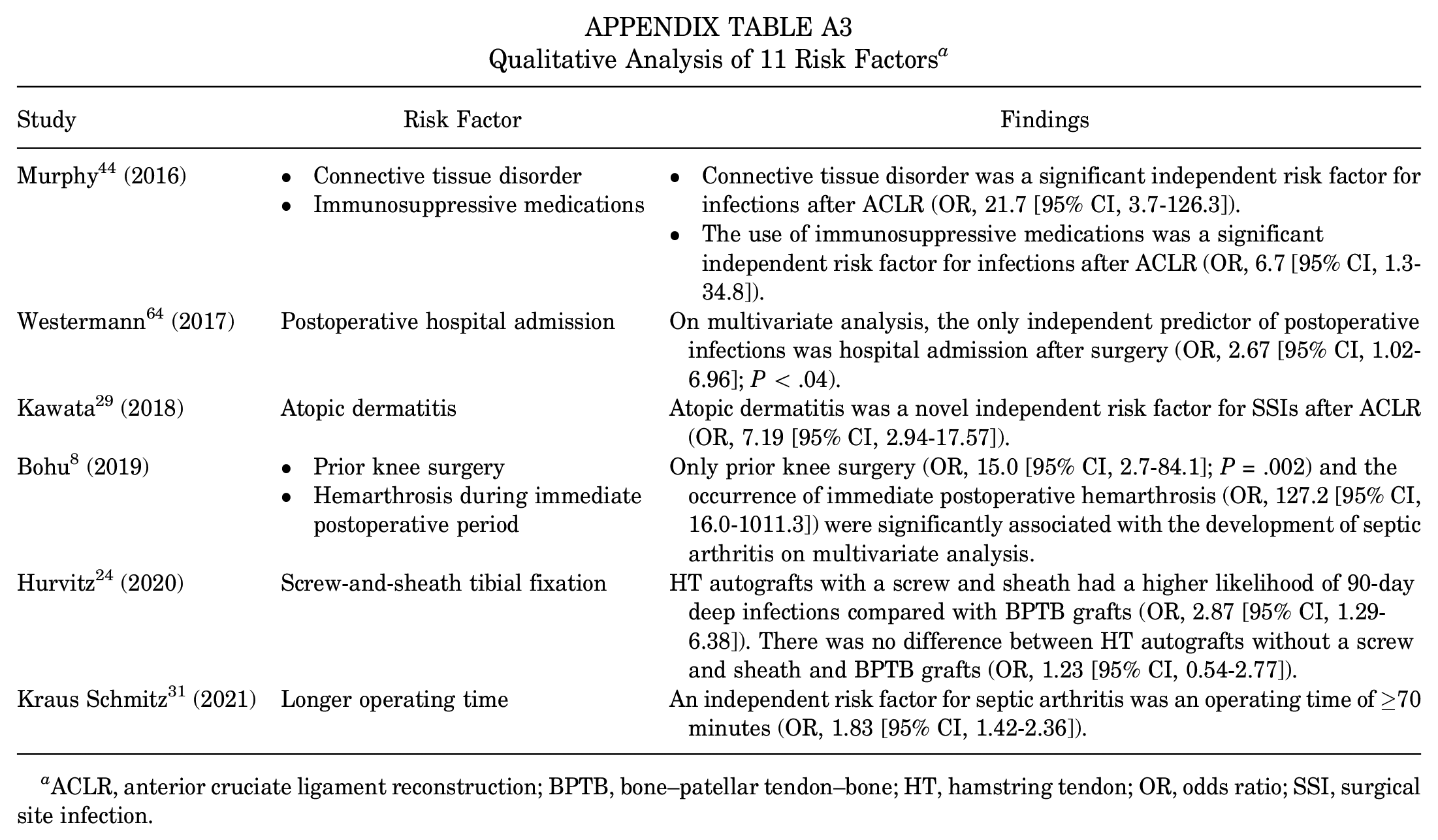
Our analysis ultimately comprised 20 risk factors, with 12 subjected to a meta-analysis: sex, age, BMI, diabetes, smoking, meniscal repair, HT autograft, revision surgery, professional athlete status, lateral tenodesis, steroid use, and outpatient surgery (Table 2). The remaining 8 risk factors (connective tissue disorder, immunosuppressive medications, postoperative hospital admission, atopic dermatitis, prior knee surgery, hemarthrosis during the immediate postoperative period, screw-and-sheath tibial fixation, longer operating time) underwent a qualitative analysis (Appendix Table A3).
Meta-analysis of Risk Factors for Postoperative Infection a
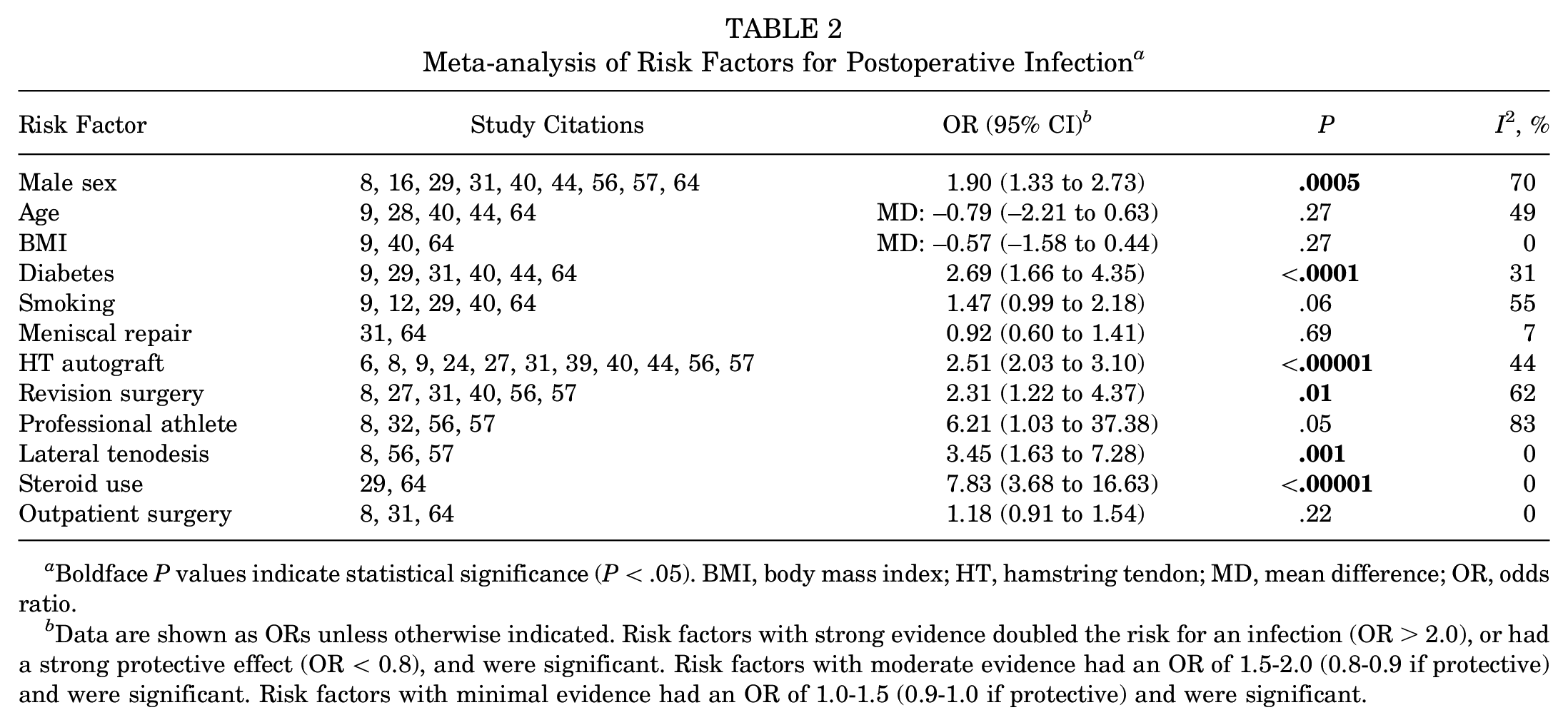
Boldface P values indicate statistical significance (P < .05). BMI, body mass index; HT, hamstring tendon; MD, mean difference; OR, odds ratio.
Data are shown as ORs unless otherwise indicated. Risk factors with strong evidence doubled the risk for an infection (OR > 2.0), or had a strong protective effect (OR < 0.8), and were significant. Risk factors with moderate evidence had an OR of 1.5-2.0 (0.8-0.9 if protective) and were significant. Risk factors with minimal evidence had an OR of 1.0-1.5 (0.9-1.0 if protective) and were significant.
Male Sex
A total of 9 studies investigated the association between male sex and infections after ACLR, including 918 patients in the case group and 93,066 patients in the control group. The pooled results showed that male patients were more likely to develop infections after ACLR than female patients (OR, 1.90 [95% CI, 1.33-2.73]; P = .0005; I2 = 70%) (Figure 2A). Based on the statistical results, there was moderate evidence to suggest that male sex was a risk factor for infections after ACLR. High heterogeneity was also observed. Sensitivity analysis found that the study by Kawata et al 29 was the main source of heterogeneity. After removing this study, I2 was reduced to 48%, and pooled analysis of the remaining studies still showed significant differences and no significant change from the original result (OR, 1.73 [95% CI, 1.44-2.08]; P < .00001), indicating the robustness of the final finding. Based on the study characteristics, we speculated that the main source of heterogeneity is likely to be population differences. The patients in the Kawata et al 29 study were all from Japan, whereas the remaining studies included populations mainly from the United States or France.

Forest plots showing the association of infections after anterior cruciate ligament reconstruction with patient characteristics: (A) sex, (B) age, (C) body mass index, (D) diabetes, and (E) smoking. IV, inverse variance; M-H, Mantel-Haenszel.
Age
A total of 5 studies investigated the association between age and infections after ACLR, including 231 patients in the case group and 32,389 patients in the control group. The pooled results showed that age was not significantly associated with infections after ACLR (MD, –0.79 [95% CI, –2.21 to 0.63]; P = .27; I2 = 49%) (Figure 2B). Based on the statistical results, age was not a risk factor for infections after ACLR.
Body Mass Index
A total of 3 studies investigated the association between higher BMI and infections after ACLR, including 104 patients in the case group and 19,943 patients in the control group. The pooled results demonstrated that BMI was not significantly associated with infections after ACLR (MD, –0.57 [95% CI, –1.58 to 0.44]; P = .27; I2 = 0%) (Figure 2C). Based on the statistical results, BMI was not a risk factor for infections after ACLR.
Diabetes
A total of 6 studies investigated the association between diabetes and infections after ACLR, including 890 patients in the case group and 86,774 patients in the control group. The pooled results showed that diabetes was significantly associated with infections after ACLR (OR, 2.69 [95% CI, 1.66-4.35]; P < .0001; I2 = 31%) (Figure 2D). Based on the statistical results, there was strong evidence to suggest that diabetes was a risk factor for infections after ACLR.
Smoking
A total of 5 studies investigated the association between smoking and infections after ACLR, including 613 patients in the case group and 63,328 patients in the control group. The pooled results showed that smoking was not significantly associated with infections after ACLR (OR, 1.47 [95% CI, 0.99-2.18]; P = .06; I2 = 55%) (Figure 2E). Based on the statistical results, smoking was not a risk factor for infections after ACLR. High heterogeneity was also observed. Sensitivity analysis found that the study of Cancienne et al 12 was the main source of heterogeneity. After this study was removed, I2 was reduced to 0%, and pooled analysis of the remaining studies still demonstrated no significant differences and no significant change from the original result (OR, 1.23 [95% CI, 1.00-1.52]; P = .05), indicating the robustness of the final finding.
Meniscal Repair
A total of 2 studies investigated the association between meniscal repair and infections after ACLR, including 330 patients in the case group and 31,377 patients in the control group. The pooled results showed that meniscal repair was not significantly associated with infections after ACLR (OR, 0.98 [95% CI, 0.64-1.50]; P = .91; I2 = 23%) (Figure 3A). Based on the statistical results, meniscal repair was not a risk factor for infections after ACLR.

Forest plots showing the association of infections after anterior cruciate ligament reconstruction (ACLR) with (A) meniscal repair, (B) hamstring tendon autograft, and (C) revision ACLR. M-H, Mantel-Haenszel.
HT Autograft
A total of 11 studies investigated the association between HT autografts and infections after ACLR, including 641 patients in the case group and 88,117 patients in the control group. The pooled results showed that ACLR with HT autografts was more likely to lead to postoperative infections than ACLR with other types of grafts (OR, 2.51 [95% CI, 2.03-3.10]; P < .00001; I2 = 44%) (Figure 3B). Based on the statistical results, there was strong evidence to suggest that an HT autograft was a risk factor for infections after ACLR.
Revision Surgery
A total of 6 studies investigated the association between revision surgery and infections after ACLR, including 396 patients in the case group and 44,969 patients in the control group. The pooled results showed that patients undergoing revision were more likely to develop postoperative infections than those undergoing primary ACLR (OR, 2.31 [95% CI, 1.22-4.37]; P = .01; I2 = 62%) (Figure 3C). Based on the statistical results, there was strong evidence to suggest that revision surgery was a risk factor for infections after ACLR. High heterogeneity was also observed. Sensitivity analysis found that the study by Kraus Schmitz et al 31 was the main source of heterogeneity. After removing this study, I2 was reduced to 0%, and pooled analysis of the remaining studies still showed a significant difference and no significant change from the original result (OR, 3.13 [95% CI, 1.98-4.96]; P < .00001), indicating the robustness of the final finding.
Professional Athlete
A total of 4 studies investigated the association between professional athlete status and infections after ACLR, including 51 patients in the case group and 9945 patients in the control group. The pooled results showed that professional athletes were significantly associated with infections after ACLR (OR, 6.21 [95% CI, 1.03-37.38]; P = .05; I2 = 83%) (Figure 4A). Based on the statistical results, there was strong evidence to suggest that professional athlete status was a risk factor for infections after ACLR. High heterogeneity was also observed. Sensitivity analysis found that the studies of Krutsch et al 32 and Bohu et al 8 were the main sources of heterogeneity. I2 was reduced to 0% after these studies were removed; however, pooled analysis of the remaining studies still showed significant differences and no significant change from the original result (OR, 23.48 [95% CI, 10.62-51.91]; P < .00001), indicating the robustness of the final finding. Based on the study characteristics, we found that the type of sports in which athletes participated varied across studies, which may be the source of heterogeneity.

Forest plots showing the association of infections after anterior cruciate ligament reconstruction with (A) professional athlete status, (B) lateral tenodesis, (C) corticosteroid use, and (D) outpatient surgery. M-H, Mantel-Haenszel.
Lateral Tenodesis
A total of 3 studies investigated the association between lateral tenodesis and infections after ACLR, including 34 patients in the case group and 8153 patients in the control group. The pooled results showed that lateral tenodesis was significantly associated with infections after ACLR (OR, 3.45 [95% CI, 1.63-7.28]; P = .001; I2 = 0%) (Figure 4B). Based on the statistical results, there was strong evidence to suggest that lateral tenodesis was a risk factor for infections after ACLR.
Corticosteroid Use
A total of 2 studies investigated the association between steroid use and infections after ACLR, including 413 patients in the case group and 36,521 patients in the control group. The pooled results showed that steroid use was significantly associated with infections after ACLR (OR, 7.83 [95% CI, 3.68-16.63]; P < .00001; I2 = 0%) (Figure 4C). Based on the statistical results, there was strong evidence to suggest that steroid use was a risk factor for infections after ACLR.
Outpatient Surgery
A total of 3 studies investigated the association between outpatient surgery and infections after ACLR, including 337 patients in the case group and 33,179 patients in the control group. The pooled results showed that outpatient surgery was not significantly associated with infections after ACLR (OR, 1.18 [95% CI, 0.91-1.54]; P = .22; I2 = 0%) (Figure 4D). Based on the statistical results, outpatient surgery was not a risk factor for infections after ACLR.
Subgroup Analysis of Infection Type
Overall, 10 of the 17 included studies reported only septic arthritis, while the remaining 7 studies included cases of all SSIs. As mixing them together for pooled analysis may lead to confounding bias, we performed a further meta-analysis of studies that reported only septic arthritis. The new pooled results analyzing 11 risk factors showed that the statistical results did not change significantly, except for the factor of diabetes. Subgroup analysis results suggested that diabetes was not a risk factor for septic arthritis (OR, 1.56 [95% CI, 0.61-3.98]; P = .35; I2 = 19%). The results are shown in Table 3.
Meta-analysis of Risk Factors for Septic Arthritis a
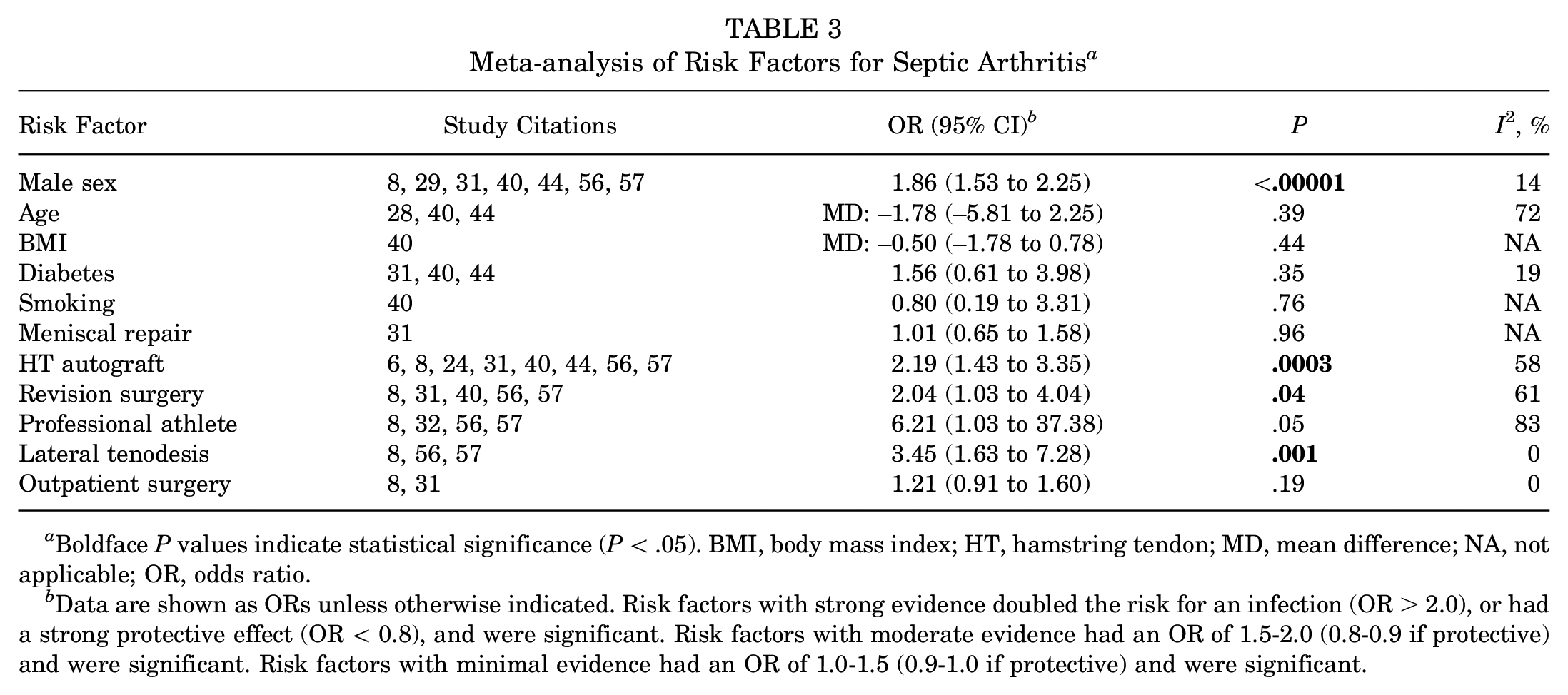
Boldface P values indicate statistical significance (P < .05). BMI, body mass index; HT, hamstring tendon; MD, mean difference; NA, not applicable; OR, odds ratio.
Data are shown as ORs unless otherwise indicated. Risk factors with strong evidence doubled the risk for an infection (OR > 2.0), or had a strong protective effect (OR < 0.8), and were significant. Risk factors with moderate evidence had an OR of 1.5-2.0 (0.8-0.9 if protective) and were significant. Risk factors with minimal evidence had an OR of 1.0-1.5 (0.9-1.0 if protective) and were significant.
Discussion
In this systematic review and meta-analysis, the main findings were that diabetes, revision ACLR, HT autograft, professional athlete status, lateral tenodesis, and steroid use provided strong evidence for the occurrence of infections after ACLR. There was moderate evidence to suggest that male sex was an important risk factor for infections after ACLR, while age, BMI, smoking, meniscal repair, and outpatient surgery were not associated with an increased risk of infections after ACLR. The results of the subgroup analysis suggested that diabetes was a risk factor for overall infections but not specifically for septic arthritis.
Our study demonstrated that male patients exhibited 90% higher odds (OR, 1.90) of experiencing an infection after ACLR compared to their female counterparts. A couple of investigations conducted by Roecker et al 51 and Kraus Schmitz et al 31 on 217,541 and 25,309 patients, respectively, further bolster our findings, with male patients displaying a greater susceptibility to infections (OR, 1.58 and 1.65, respectively). Sex-related differences in daily life and sports intensity likely account for our findings. 60 This is also similar to the findings on risk factors for a periprosthetic infection after total knee arthroplasty14,25,26,46 in which male sex has been demonstrated to be an independent risk factor for infections. However, based on the present data, we cannot explain whether this difference is because of the sex itself or as a proxy for some risk factors. Although we cannot speculate on causation from systematic reviews, our conclusions highlight that orthopaedic surgeons should recognize that male patients are an at-risk population for infections after ACLR.
The outcomes of our meta-analysis indicated a 2.69-fold elevated risk of infections after ACLR among patients with diabetes. Patients with diabetes, especially those with suboptimal glycemic control, have been well established to be associated with an increased risk of SSIs after multiple orthopaedic procedures, including total joint arthroplasty,2,30 spinal surgery,18,35 and ankle surgery. 47 Diabetes-increased susceptibility to infections is related to impaired immune responses within the hyperglycemic environment and microvascular complications. In addition, microvascular lesions leading to local tissue ischemia and factors associated with diabetes, including hypertension, increased oxidative stress, and inflammatory responses, also impede wound healing.17,49 It is intriguing that when only cases of septic arthritis were included, diabetes appeared not to be significantly associated with septic arthritis after ACLR. This may be because of the lack of sufficient data, with only 3 studies included in this comparison. Alternatively, diabetes may primarily impair the healing of superficial surgical incisions, and its effect on infections within the joint is not significant. However, the lack of descriptions for the type of diabetes in the included studies limited further discussions.
The use of HT autografts compared with other grafts (bone–patellar tendon–bone autografts or allografts) increased the risk of infections after ACLR (OR, 2.51). Because a possible source of septic arthritis after ACLR is contaminated grafts, several studies have investigated the infection rate depending on the choice of grafts. The contamination rate during autograft preparation was found to be higher for HT autografts compared to bone–patellar tendon–bone autografts (13% vs 10%, respectively). 22 The sources of graft contamination, either during the harvest process or the preparation phase on the back table, remain indeterminate. It is worth noting that the preparation time for HT autografts exceeds that of other grafts, consequently augmenting the window for potential contamination during graft preparation.19,21 The utilization of multifilament suture during the preparation of HT grafts is commonplace, despite its proclivity to serve as a vector for bacterial colonization. Additionally, bacterial contamination may ensue during the graft implantation phase, particularly if the graft or hardware is in proximity with the skin. 39 Bacterial cultures were performed in 8 of the 17 included studies, and the most common pathogen was Staphylococcus epidermidis8,27,56 or S. aureus.6,24,39,57 This finding also confirms the conclusions of the previous literature.1,5 Given recent evidence supporting a significant reduction in the incidence of infections after ACLR by soaking grafts in vancomycin,13,45 surgeons may consider using this prophylactic measure, especially for high-risk grafts. We acknowledge the fact that the use of specific grafts increases the risk of infections, but given the very low overall infection rate, the choice of grafts still requires a comprehensive evaluation.
Revision ACLR was found to be associated with an increased risk of infections after ACLR. Specifically, the OR was 2.31, suggesting that revision ACLR was 131% more likely to result in infections compared with primary ACLR. This is consistent with the results previously reported by Schuster et al 54 in that the ratio of revision to primary reconstruction for postoperative septic arthritis was 2.5. An analysis of 16,192 ACLR procedures by Maletis et al 38 found that a deep SSI developed in 0.3% of primary ACLR cases versus 0.9% of revision cases. This may be caused by the longer operative time and more complex procedures for revision surgery compared with primary ACLR.15,20 Recently, some strategies to prevent infections after revision ACLR have been explored, including the use of quadriceps tendon 53 and vancomycin-soaked grafts. 52
Our results showed that patients who were professional athletes were at a higher risk of infections after ACLR (OR, 6.21). This finding corroborates data reported in the previous literature that explored whether professional athletes are susceptible to infections. Sonnery-Cottet et al 57 found that being a professional player was associated with a significantly increased risk of infections after ACLR (OR, 21.0). Ristić et al 50 also reported a higher rate of infections in professional athletes (1.9%) than in nonprofessional athletes (0.8%). Conversely, Bohu et al 8 reported no significant difference in infection rates between the 2 groups, and no special precautions were required in professional athletes. However, this conclusion must be interpreted with caution, as the post hoc calculation suggested that the power of their study was close to zero. Krutsch et al 32 also found that the difference in postoperative infection rates did not depend on whether the athletes were professional but rather on the type of sports. Athletes who participate in summer outdoor sports (eg, football) have a significantly higher risk of infections after ACLR than athletes in winter sports. Possible reasons include external risk factors such as protective clothing at the time of the injury 10 or higher infection rates in athletes injured by frequent skin-to-skin contact. 60 Another explanation could be differences in skin bacterial colonization due to variations in temperature and sweat excretion depending on participation in different sports. 32
Patients who underwent combined lateral tenodesis at the time of ACLR were 3.45 times more likely to develop infections after ACLR than patients without lateral tenodesis. Potential explanations for the higher infection rate include increased operating time, the size of skin incisions, and the number of implants. However, several studies have reported opposite results, indicating that the infection rate for combined intra- and extra-articular reconstruction is not higher than that for isolated intra-articular ACLR.36,48 Our finding should be interpreted with caution because in the study by Sonnery-Cottet et al, 56 only 9% of nonprofessional athletes underwent lateral tenodesis, whereas 23% of professional athletes did. In the nonprofessional group, no patients had an infection after undergoing ACLR with combined lateral tenodesis. The strong correlation between lateral tenodesis and professional athletes suggests that one of the variables is a confounding factor. Sonnery-Cottet et al 56 speculated that it is this variable in professional athletes that plays a major role, conferring a higher infection rate. This is in accordance with the results of the current meta-analysis.
Our results showed that patients with corticosteroid use were more likely to develop infections after ACLR (OR, 7.83). However, only 2 studies29,64 were included in this meta-analysis, with a relatively small number of patients with postoperative infections. Considerable caution is needed when interpreting the results for steroid use. Kawata et al 29 focused on patients with regular preoperative steroid use, while Westermann et al 64 did not elucidate the administration of steroids. Neither mentioned the dose of steroid use. Steroids are frequently used to prevent postoperative nausea and vomiting. 43 They also confer other benefits, including postoperative pain relief 34 and reduced postoperative postural hypotension. 3 Previous studies have shown that intraoperative steroid injections increase the risk of SSIs after arthroscopic surgery, 4 but there is a paucity of literature on the systemic administration of steroids in the perioperative period of ACLR. However, the lack of specification on the mode of steroid administration in the included studies limited further discussions.
Limitations
The current study has some limitations that need to be noted. First, different study designs, included populations, and types of infections contributed to the heterogeneity of the review, but we conducted sensitivity and subgroup analyses to explore the sources of heterogeneity as much as possible. Second, most of the included studies identified cases of infections after ACLR based on disease diagnosis codes rather than clinical assessments. Possible coding errors, in addition to the fact that patients may not return to their original institution for treatment of the infection, can lead us to underestimate the incidence of infections. Third, the different techniques used to perform the procedure, the various surgeons, and the antibiotic regimen to treat infections have not been discussed, creating confounding bias and limiting the generalizability of this study. In addition, many studies have shown a significant reduction in infection rates with vancomycin-soaked grafts,13,45,65 but this factor was not analyzed in the studies that we included. Because the earliest study using vancomycin-soaked grafts was conducted in approximately 2012 61 and most of our included studies were performed earlier than this time point, none of them routinely applied this new technique. Future studies with more recent data will hopefully shed light on this issue. Fourth, some of the included studies provided only univariate rather than multivariate statistics, which may lead to some bias in our analysis. An infection after ACLR is caused by multiple factors that are interrelated and interdependent, and it cannot be explained by every single factor.
Conclusion
Our study revealed an increased risk of infections after ACLR associated with male sex, diabetes, HT autograft, revision surgery, professional athlete status, lateral tenodesis, and corticosteroid use. There was no significant association between age, BMI, smoking, meniscal repair, and outpatient surgery with infections after ACLR. Knowledge of the risk factors associated with an infection after ACLR may facilitate the identification of high-risk cases and the implementation of preventive measures to mitigate the serious consequences of this complication.
Footnotes
Appendix
Qualitative Analysis of 11 Risk Factors a
| Study | Risk Factor | Findings |
|---|---|---|
| Murphy 44 (2016) | • Connective tissue disorder • Immunosuppressive medications |
• Connective tissue disorder was a significant independent risk factor for infections after ACLR (OR, 21.7 [95% CI, 3.7-126.3]). • The use of immunosuppressive medications was a significant independent risk factor for infections after ACLR (OR, 6.7 [95% CI, 1.3-34.8]). |
| Westermann 64 (2017) | Postoperative hospital admission | On multivariate analysis, the only independent predictor of postoperative infections was hospital admission after surgery (OR, 2.67 [95% CI, 1.02-6.96]; P < .04). |
| Kawata 29 (2018) | Atopic dermatitis | Atopic dermatitis was a novel independent risk factor for SSIs after ACLR (OR, 7.19 [95% CI, 2.94-17.57]). |
| Bohu 8 (2019) | • Prior knee surgery • Hemarthrosis during immediate postoperative period |
Only prior knee surgery (OR, 15.0 [95% CI, 2.7-84.1]; P = .002) and the occurrence of immediate postoperative hemarthrosis (OR, 127.2 [95% CI, 16.0-1011.3]) were significantly associated with the development of septic arthritis on multivariate analysis. |
| Hurvitz 24 (2020) | Screw-and-sheath tibial fixation | HT autografts with a screw and sheath had a higher likelihood of 90-day deep infections compared with BPTB grafts (OR, 2.87 [95% CI, 1.29-6.38]). There was no difference between HT autografts without a screw and sheath and BPTB grafts (OR, 1.23 [95% CI, 0.54-2.77]). |
| Kraus Schmitz 31 (2021) | Longer operating time | An independent risk factor for septic arthritis was an operating time of ≥70 minutes (OR, 1.83 [95% CI, 1.42-2.36]). |
ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; OR, odds ratio; SSI, surgical site infection.
Final revision submitted May 9, 2023; accepted May 19, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.