
Abstract
Background:
Osteochondral allograft transplantation (OCA) treats symptomatic focal cartilage defects with satisfactory clinical results.
Purpose:
To comprehensively analyze the characteristics and clinical outcomes of OCA for treating articular cartilage defects.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
We searched Embase, PubMed, Cochrane Database, and Web of Science for studies published between January 1, 2001, and December 31, 2020, on OCA for treating articular cartilage defects. Publication information, patient data, osteochondral allograft storage details, and clinical outcomes were extracted to conduct a comprehensive summative analysis.
Results:
In total, 105 studies involving 5952 patients were included. The annual reported number of patients treated with OCA increased from 69 in 2001 to 1065 in 2020, peaking at 1504 cases in 2018. Most studies (90.1%) were performed in the United States. The mean age at surgery was 34.2 years, and 60.8% of patients were male and had a mean body mass index of 26.7 kg/m2. The mean lesion area was 5.05 cm2, the mean follow-up duration was 54.39 months, the mean graft size was 6.85 cm2, and the number of grafts per patient was 54.7. The failure rate after OCA was 18.8%, and 83.1% of patients reported satisfactory results. Allograft survival rates at 2, 5, 10, 15, 20, and 25 years were 94%, 87.9%, 80%, 73%, 55%, and 59.4%, respectively. OCA was mainly performed on the knee (88.9%). The most common diagnosis in the knee was osteochondritis dissecans (37.9%), and the most common defect location was the medial femoral condyle (52%). The most common concomitant procedures were high tibial osteotomy (28.4%) and meniscal allograft transplantation (24.7%). After OCA failure, 54.7% of patients underwent revision with primary total knee arthroplasty.
Conclusion:
The annual reported number of patients who underwent OCA showed a significant upward trend, especially from 2016 to 2020. Patients receiving OCA were predominantly young male adults with a high body mass index. OCA was more established for knee cartilage than an injury at other sites, and its best indication was osteochondritis dissecans. This analysis demonstrated satisfactory long-term postoperative outcomes.
Keywords
Articular cartilage covers the ends of the connected bones in joints. It lubricates the joint surface, reducing the joint surface friction and buffering against shocks and impacts during movement. 23 Articular cartilage lacks nerves and a vascular supply; therefore, its nutrition is supplied by the synovial fluid and arterial branches around the synovial membrane layer of the articular capsule.31,33,106 Once the articular cartilage is damaged or degraded, its capacity to repair and heal is limited.114,120,121 Articular cartilage defects can be caused by various causes, such as trauma, degeneration, avascular necrosis, osteochondritis dissecans, or osteoarthritis. 86 Studies have shown the prevalence of cartilage damage to be as high as 66%, 123 leading to a range of symptoms including swelling, pain, and limited mobility.28,94 Cartilage damage may eventually lead to accelerated cartilage wear, increased pain, impaired joint stability, and further development into diffuse osteoarthritis, with ultimate loss of joint function.46,62,86,99 At the same time, unstable injuries may cause progressive degeneration of the surrounding normal cartilage due to load transfer. 28 Since articular cartilage has limited inherent capacity for spontaneous healing after injury, symptomatic articular cartilage defects benefit from cartilage repair treatment. Therefore, it is necessary to study patients undergoing cartilage repair therapy with symptomatic articular cartilage injuries.
To delay the progression of osteoarthritis and obviate the implementation of arthroplasty, an appropriate cartilage repair protocol can be selected according to the characteristics of the cartilage injury. 94 Traditionally, surgical methods for treating cartilage injuries can be divided into palliative, reparative, and restorative treatments. Palliative treatments include chondral debridement and chondroplasty. Reparative and restorative treatments include marrow stimulation techniques (MSTs; subchondral drilling and microfracture), autologous chondrocyte implantation (ACI), osteochondral autograft transfer (OAT), and osteochondral allograft transplantation (OCA).46,62,86 Although many factors should be considered in selecting appropriate cartilage repair surgery, research has shown that a small area of cartilage damage is more suitable for MST and OAT. In addition, the treatment effect was even more satisfactory than that of other cartilage repair surgery. In contrast, large cartilage defects >4 cm2 are more suitable for ACI or OCA treatment.86,94
OCA is a restorative cartilage procedure for symptomatic focal cartilage defects that involves transplanting surviving mature hyaline cartilage and supporting subchondral bone into the area of the cartilage defect.20,75,93,108 As a well-developed, single-stage restorative cartilage procedure, OCA has increasingly become the preferred treatment after cartilage repair surgery failures. OCA has many advantages compared with other cartilage repair techniques, such as simultaneously repairing the cartilage and subchondral bone, treating large or multisite cartilage defects, and supporting early weightbearing.46,108 Two studies have shown satisfactory long-term clinical results after OCA, with allograft survival rates at 10 to 25 years postoperatively as high as 59% to 91%.86,136
The extensive application of OCA has rendered it 1 of the most common cartilage repair procedures in the United States. 75 However, the availability of allograft is limited because of the scarcity of donor grafts and duration of graft preservation.48,116,119 Furthermore, there have not been any studies describing the use of OCA at different locations and the demographic data of patients undergoing this procedure. Therefore, we aimed to conduct a comprehensive systematic review and single-arm meta-analysis of the characteristics and clinical outcomes of OCA in treating articular cartilage defects over the past 2 decades (2001-2020) to better understand its research status in different countries, clarify the trends and clinical results of OCA in different sites, and provide clarification and data support for the clinical application of OCA.
Methods
Search Strategy
A comprehensive systematic literature search was completed per the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 105 The literature retrieval was conducted in October 2021 using the Embase, PubMed, Cochrane Database, and Web of Science databases for all the relevant English articles. The following search terms were used: (“osteochondral” or “cartilage” or “cartilages”) and (“allograft” or “allogeneic transplants” or “allogeneic transplant” or “transplant, allogeneic” or “transplants, allogeneic” or “allogeneic grafts” or “allogeneic graft” or “graft, allogeneic” or “grafts, allogeneic” or “homografts” or “homograft” or “homologous transplants” or “homologous transplant” or “transplant, homologous” or “transplants, homologous”). We searched the publication date range from January 1, 2001, to December 31, 2020.
Study Selection
The obtained studies were screened and selected using the following inclusion criteria: (1) the participants included were patients of all ages with a definite diagnosis of osteochondral injury, (2) all publicly published clinical studies were written in English and involved OCA for cartilage defects, and (3) the patients were evaluated at minimum 2-year follow-up. The exclusion criteria were as follows: (1) revision OCA procedures; (2) chondral defects treated with particulate juvenile articular allograft cartilage; and; (3) duplicate articles, literature reviews, meta-analyses, case reports, technical notes, editorial commentaries, expert consensus statements, conference abstracts and presentations, animal studies, biomechanical studies, and other nonclinical studies.
The references for all included studies were assessed and screened to ensure integrity and thoroughness. Two authors (X.W. and Z.R.) independently reviewed the literature to determine the final inclusion criteria, and any disagreements were resolved between them or discussed with a third author (W.D.).
Data Extraction
All relevant study data were extracted by 2 independent reviewers (X.W. and Y.L.). The extracted data included publication information, sample size, patient characteristics (mean age, sex, mean body mass index (BMI), smoking, mean symptom duration, mean follow-up time), defect size and location, size and number of grafts, storage details of osteochondral allografts, mechanism of injury, previous and concomitant surgeries, failures, reoperations, survival of grafts, and satisfaction. Allograft failure was defined as the removal or revision of the primary OCA, conversion to any arthroplasty, or gross appearance of graft failure on second-look arthroscopy.39,46,91,93 Any inconsistencies were discussed or resolved with a third author (W.D.).
Statistical Analysis
All extracted data were analyzed using SPSS (Version 19.0; IBM) and Stata/SE 12.0 (StataCorp). Continuous variable data were reported as means and standard deviations, whereas categorical variable data were reported as frequencies and percentages. If partial continuous variables were raw data, the calculation was converted into means and standard deviations to summarize the results consistently. If the mean or standard deviation was not given, it was calculated from the median, minimum, and maximum values.64,134 Continuous variables were pooled by calculating the mean and 95% CIs, and dichotomous variables were pooled by calculating the proportion and 95% CI. The I2 statistic was used to measure the heterogeneity among the included studies. The statistical heterogeneity between the studies was considered low, medium, and high when the I2 thresholds were <25%, 25-75%, and >75%, respectively. The pooled analysis results were deemed statistically significant at P < .05.
Results
Search Results
A total of 1389 relevant articles were identified using the electronic database and search strategy. Of these, 798 were excluded after removing duplicates, and 591 articles remained for screening. Of these, 469 were excluded based on the exclusion criteria. We closely reviewed the full texts of the remaining 122 articles, of which 17 were excluded, leaving 105 studies § included in this review (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study inclusion.
Overall Characteristics and Clinical Outcomes of OCA
Temporal Trends and Country and Injury Site Distributions
The 105 studies included a total of 5952 patients. The annual reported number of patients treated with OCA showed a significant upward trend, from 69 patients in 2001 to 1065 cases in 2020, peaking in 2018 with 1504 cases. No cases were reported in 2002, 2003, and 2006 (Figure 2A). The country distribution of OCA procedures is summarized in Figure 2B. These studies were conducted in 8 countries, the majority of which were performed in the United States (90.12%), followed by Canada (6.23%). The most common location OCA was performed was the knee (88.9%), followed by the ankle (9.73%), shoulder (0.66%), hip (0.59%), and elbow (0.15%) (Figure 2C).
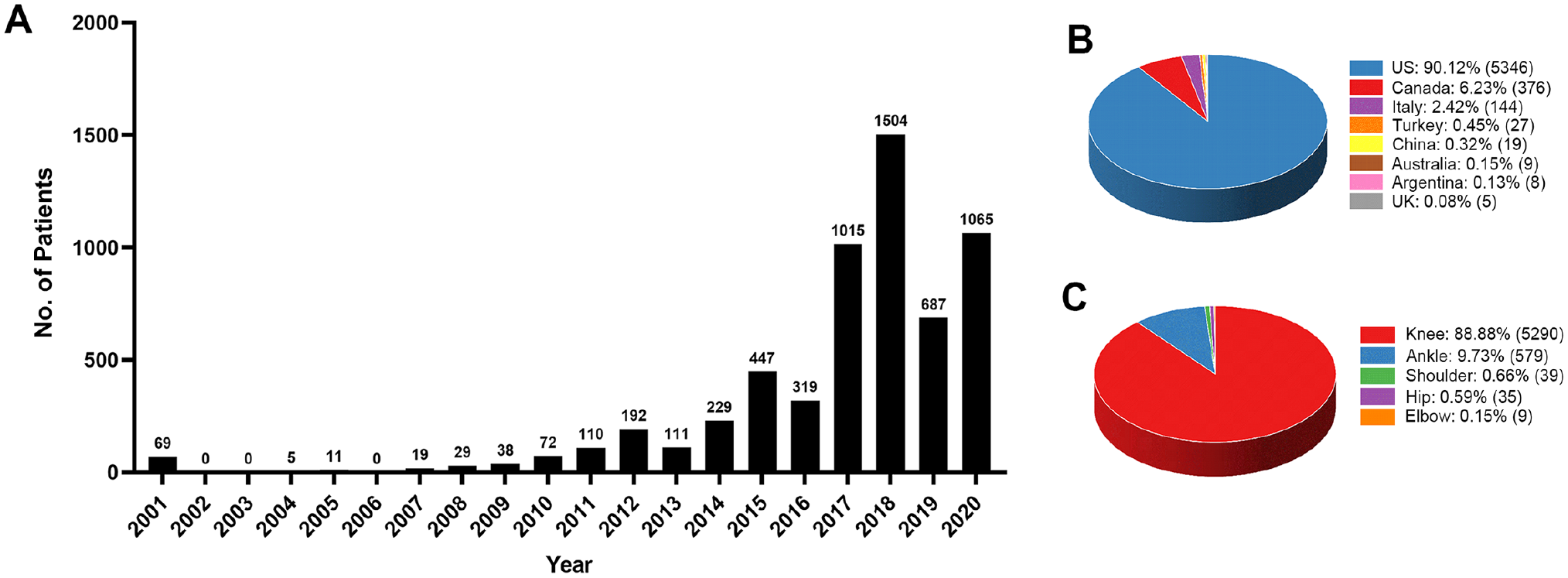
Overall temporal trends, country and injury site distribution of osteochondral allograft transplantation. (A) Annual number of cases reported in studies. (B) The proportion and number of cases reported in studies in different countries. (C) The proportion and number of cases reported in studies in different injury sites.
Patient Characteristics
The characteristics of the patients are summarized in Table 1. The mean age of the patients at the time of surgery was 34.2 years. Most of the patients were male (60.8%). The mean BMI was 26.7 kg/m2, and 21.1% of the patients were smokers. Right-sided surgery accounted for 53% of all patients. The mean lesion area was estimated at 5.05 cm2. The mean symptom duration was 38.0 months, and the mean follow-up duration was 54.4 months. Most patients (77.4%) underwent ≥1 operation at the same surgical site before OCA surgery. The affected joints underwent a mean of 1.93 procedures before OCA surgery. OCA was performed alone in most patients (60.1%).
Characteristics of the Patients in the Included Studies (N = 5952)

Allograft Characteristics
The graft size was reported in 27 studies
‖
(n = 2244), with a mean graft size of 6.85 cm2 (95% CI, 6.16-7.54 cm2). The mean number of grafts used per patient was 1.49 (95% CI, 1.41-1.57) in the 2655 patients reported. Additionally, 57 studies
¶
(n = 2648) mentioned allograft storage temperatures; 40 studies
#
(n = 2026) indicated a preservation temperature of 4°C, 4 studies6,7,57,103 (n = 47) mentioned temperatures between 2°C and 4°C, and 9 studies12,104,109,135,137-141 (n = 524) described cold storage. Only 3 studies63,144,145 (n = 36) used freezing for osteochondral allograft preservation. Furthermore, the details of the storage solution and type of media were examined in 18 studies.
**
Seven studies1,11,55,72,73,78,110 (n = 325) from Canada reported that osteochondral allografts were stored in Ringer’s lactate solution containing 1 g cefazoline and 50,000 units bacitracin per liter. Four studies15,79,88,115 (n = 238) from the United States reported that grafts were stored in Ringer’s lactate solution containing 1 g/L cefazolin and 10 g/mL gentamicin. Four studies42-45 (n = 113) from Italy reported that grafts were immersed in a solution containing
Overall Clinical Outcomes of OCA
In 68 studies ‡‡ (n = 4355) that discussed failure rates, 18.8% of patients had a failed OCA. In total, 35.5% of 3094 patients returned to the operating room at least once for further treatment. The mean time to failure was 4.48 years (Table 2). The Kaplan-Meier survival analysis demonstrated an allograft survival rate of 94% (95% CI, 90.4%-97.5%) of 259 patients 2 years post-transplantation, 87.9% (95% CI, 85.4%-90.5%) of 2114 patients at 5 years, 80% (95% CI, 75.4%-84.6%) of 1860 patients at 10 years, 73% (95% CI, 68.1%-77.9%) of 639 patients at 15 years, 55% (95% CI, 41.3%-68.7%) of 387 patients at 20 years, and 59.4% (95% CI, 50.5%-68.3%) of 118 patients at 25 years (Figure 3A). A total of 33 studies §§ (n = 2355) had available data regarding patient satisfaction with the results of the OCA procedure. Overall, 83.1% of patients reported being somewhat satisfied with the OCA results (Table 2). Overall trends for annual failures, reoperations, and satisfaction of patients treated with OCA showed no significant trend from 2001 to 2020 (Figure 3, B-D).
Overall Clinical Outcomes of OCA a

OCA, osteochondral allograft transplantation.

Annual clinical outcomes and variation trends of osteochondral allograft transplantation. (A) Trends in graft survival at 2, 5, 10, 15, 20, and 25 years after transplantation. (B) Annual failure rate and its trends after transplantation. (C) Annual reoperation rate and its trends after transplantation. (D) Annual satisfaction rate and its trends after transplantation. The value of 0 only represents that no relevant study reported the result in that year.
OCA of the Knee
Patient Characteristics and Allograft Details of Knee OCA
Overall, 74 studies ‖ ‖ reported 5290 patients who underwent knee OCA surgery. The mean age of the patients at the time of surgery was 33.7 years. Most patients were male (60.6%). The patients’ mean BMI was 26.7 kg/m2, and the mean lesion area was estimated at 4.81 mm2. The mean symptom duration was 28.2 months, and the mean follow-up duration was 58.4 months. Graft size was reported in 25 studies ¶¶ (n = 2213), with a mean graft size of 7.07 cm2. The mean number of grafts per patient was 1.51 in 2630 patients (Table 3). The most common diagnosis that led to OCA treatment was osteochondral dissecans (37.9%), followed by focal degeneration (22.7%) and acute trauma (20.7%) (Figure 4A).
Patient Characteristics and Allograft Details of Knee OCA a

OCA, osteochondral allograft transplantation.
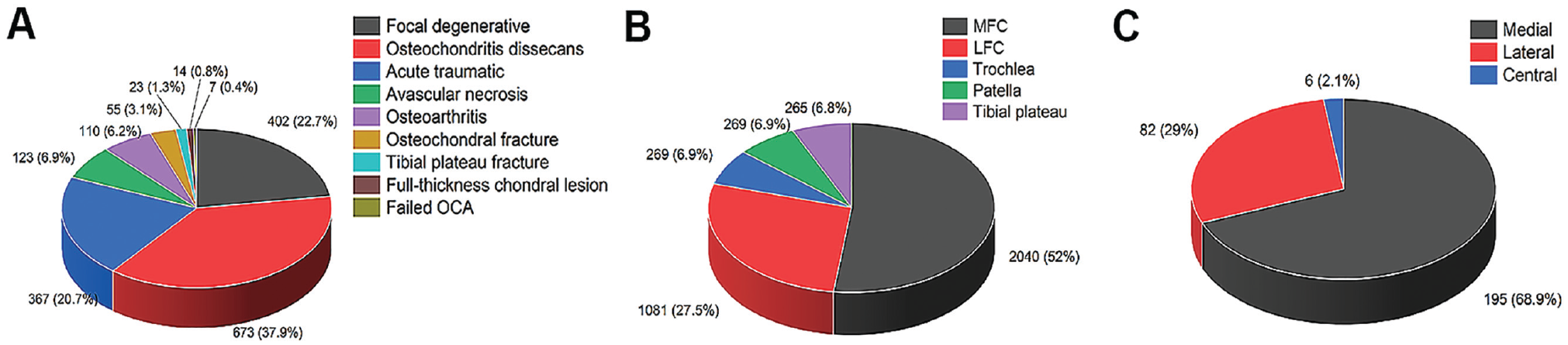
Classifications of knee surgery and specific defect sites in the knee and ankle. (A) The proportion and number of cases reported in studies for etiology of osteochondral allograft transplantation (OCA) performed on the knee. (B) The distribution and number of cases reported in studies for defect location in the knee. (C) The distribution and number of cases reported in studies for defect location in the ankle. LFC, lateral femoral condyle; MFC, medial femoral condyle.
The most common defect location was the medial femoral condyle (52%), followed by the lateral femoral condyle (27.5%), trochlea (6.9%), patella (6.9%), and tibial plateau (6.8%) (Figure 4B). Most patients (77.3%) underwent a mean of 1.96 procedures on the same knee before OCA surgery (Table 3). The surgical procedures included MST (27%), chondral debridement (17.1%), open reduction and internal fixation (12.2%), loose body removal (9.5%), meniscectomy (7.8%), ligament reconstruction (4.1%), osteotomy (3.9%), meniscal repair (2.9%), chondroplasty (2.4%), ACI (2.2%), OAT (1.7%), OCA (1.7%), hardware removal (1.7%), and others (5.8%) (Table 4).
Types of Operations Performed Before Knee OCA (n = 1784) a

ACI, autologous chondrocyte implantation; MST, marrow stimulation technique; OAT, osteochondral autograft transfer; OCA, osteochondral allograft transplantation; ORIF, open reduction and internal fixation.
Irrigation and debridement, n = 2; cartilage biopsy, 3; trochleoplasty, 1; arthroplasty, 1; bone allograft, 5; mosaicplasty, 2; synthetic scaffold, 12; meniscal allograft transplantation, 26; ligament repair, 6; lateral release, 9; lysis of adhesions, 7; bone grafting, 10; extensor mechanism surgery, 15; external fixation, 1; external fixation and fasciotomy, 1; incision and drainage, 1; incision and drainage of abscess, 1; partial patellectomy, 1.
The most common concomitant procedures were high tibial osteotomy (HTO; 29.4%) and meniscal allograft transplantation (MAT; 25.6%), followed by distal femoral osteotomy (7.9%), tibial tubercle osteotomy (7.0%), ligament reconstruction (7.7%), meniscectomy (6.2%), hardware removal (3.4%), lateral release (3.0%), loose body removal (2.6%), arthroscopy (2.6%), and others (5.7%) (Table 5).
Procedures Concomitant to Knee OCA (n = 1048) a

DFO, distal femoral osteotomy; HTO, high tibial osteotomy; MAT, meniscal allograft transplantation; OCA, osteochondral allograft transplantation; TTO, tibial tubercle osteotomy.
microfracture, n = 19; realignment osteotomy, 11; anteromedialization, 6; meniscal repair, 5; trochleoplasty, 5; marrow stimulation technique, 3; proximal patellofemoral realignment, 3; anterior release, 2; epiphysiodesis, 2; debridement, 1; posterolateral corner reconstruction, 1; synovectomy, 1; lateral imbrication, 1.
Clinical Outcomes of Knee OCA
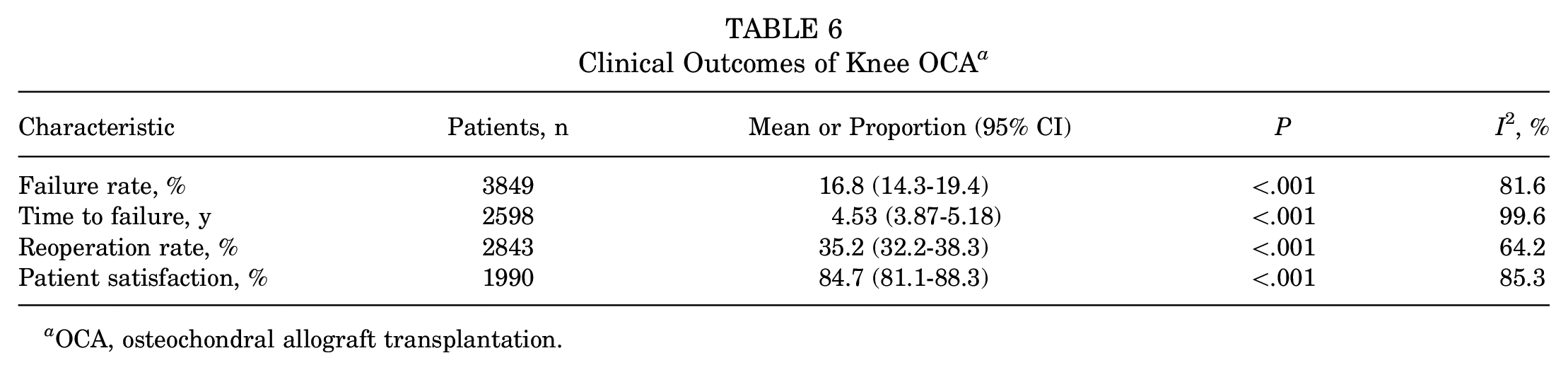
According to our analysis, 16.8% of patients failed after OCA of the knee in the 49 included studies (n = 3849); the mean time to failure was 4.53 years (Table 6). Of all failures (n = 472), 258 patients (54.7%) underwent total knee arthroplasty, 133 (28.2%) underwent revision OCA, and 39 (8.3%) underwent unicompartmental knee arthroplasty (Table 7). In total, 35.2% of 2843 patients returned to the operating room at least once. The Kaplan-Meier survival analysis demonstrated an allograft survivorship of 94% (95% CI, 90.4%-97.5%) of 259 patients at 2 years after transplantation, 89% of 1923 patients at 5 years (95% CI, 86.6%-91.5%), 83.4% of 1621 patients at 10 years (95% CI, 79.6%-87.2%), 73% of 639 patients at 15 years (95% CI, 68.1%-77.9%), 55% of 387 patients at 20 years (95% CI, 41.3%-68.7%), and 59.4% of 118 patients at 25 years (95% CI, 50.5%-68.3%). A total of 23 studies (n = 1990) had patient satisfaction data regarding the results of the knee OCA procedure; 84.7% of patients reported being at least somewhat satisfied with the results of knee OCA (Table 6).
Clinical Outcomes of Knee OCA a
OCA, osteochondral allograft transplantation.
Reoperations in Knee After OCA Failure (n = 472) a

OCA, osteochondral allograft transplantation; PKA, partial knee arthroplasty; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
OCA of the Ankle
Patient Characteristics and Allograft Details of Ankle OCA
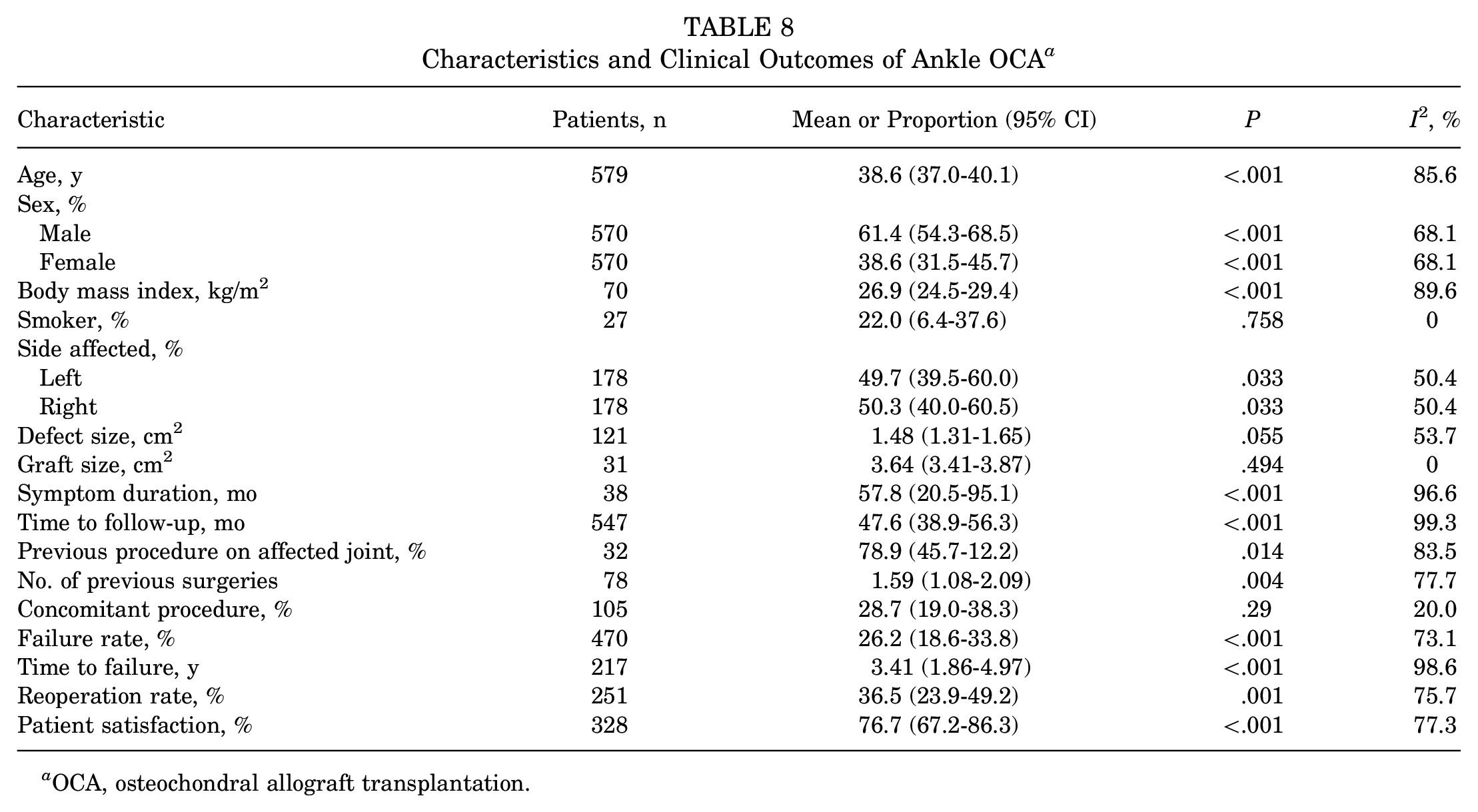
A total of 25 studies ## reported 579 patients who underwent ankle OCA. The mean age of the patients at the time of surgery was 38.6 years. Most patients were men (61.4%). The mean BMI was 26.9 kg/m2, and the mean lesion area was 1.48 mm2. The mean symptom duration was 57.8 months, and the mean follow-up duration was 47.6 months. Graft size was reported in 2 studies40,49 (n = 31), with a mean graft size of 3.64 cm2. The most common defect location was the medial talus (68.9%), followed by the lateral (29%) and central talus (2.1%) (Figure 4C). Most patients (78.9%) underwent ≥1 operation on the same ankle. The affected joints underwent a mean of 1.59 procedures before OCA surgery. OCA was performed alone in most patients (71.3%), and other concomitant procedures were performed in 28.7% of patients (Table 8).
Characteristics and Clinical Outcomes of Ankle OCA a
OCA, osteochondral allograft transplantation.
Clinical Outcomes of Ankle OCA
According to this analysis, 26.2% of patients had failed after ankle OCA in the 16 included studies a (n = 470). The mean time to failure was 3.41 years. In total, 36.5% of 251 patients returned to the operating room at least once for further treatment. The Kaplan-Meier survival analysis demonstrated an allograft survivorship rate of 78.1% (95% CI, 71%-85.2%) in 191 patients at 5 years after transplantation and 62% (95% CI, 46.9%-77%) in 239 patients at 10 years post-transplantation. Eight studies b (n = 328) had available data regarding patient satisfaction with ankle OCA, with 76.7% of patients being at least somewhat satisfied with the results (Table 8).
OCA of the Shoulder, Hip, and Elbow
For the shoulder, 2 studies112,145 reported 39 patients who underwent shoulder OCA. Patients with OCA for reverse Hill-Sachs lesions after acute locked posterior shoulder joint dislocation have significantly improved function, a low degree of osteoarthritis, and excellent clinical outcomes compared with preoperative results.84,145 Riff et al 112 concluded that OCA was a feasible treatment option for humeral head osteochondral defects. Regarding OCA of the hip, Oladeji et al 100 (n = 10), Khanna et al 72 (n = 17), and Kosashvili et al 73 (n = 8) analyzed the clinical and radiological results of OCA in patients with sizable femoral head osteochondral defects and considered fresh OCA (OCA using a freshly preserved graft) a reasonable choice for young patients with hip cartilage defects. For OCA of the elbow, Mirzayan 96 (n = 9) first reported fresh OCA to treat osteochondritis dissecans of the capitellum in 2016 in 9 male baseball players, showing that OCA significantly improved throwing function, reduced pain, and allowed all patients to resume sports.
Discussion
OCA has become increasingly established and used clinically for >40 years as a cartilage restoration technique for treating focal articular cartilage defects.20,82,123 The past 2 decades have shown an increase in research related to damaged articular cartilage repair with OCA. 35 This review demonstrated an increasing trend in the number of English-published articles on OCA from 2001 to 2020. The number of published articles in 2018 was 8 times greater than in 2000. The number of included cases was approximately 21.8 times greater, reflecting the growing interest of cartilage repair researchers in OCA. This analysis presented the cases studied in the United States, the dominant location among clinical studies of OCA, with 90.1% of global cases over the past 20 years. The widespread use of OCA programs in the United States may be due to the adequate development of OCA technology, the commercial availability of freshly stored osteochondral allografts, and reported clinical success.20,35,82,122 In contrast, the availability of OCA in other countries is lower, which is most likely due to the meager donor rates resulting from cultural and educational differences among the populations, making OCA grafts scarce and expensive.54,116,119,120
OCA is a restorative cartilage technique that can restore joint function in the knee, hip, ankle, and shoulder joints in patients with symptomatic articular cartilage defects and is currently used in treating knee cartilage injury.35,82,122 Our study showed that the number of cases studied in the knee accounted for 88.9% of all cases over the past 20 years. OCA is primarily used to repair knee and ankle cartilage damage; however, there are fewer data on OCA for cartilage repair in the shoulder, hip, and elbow than in the knee or ankle. Therefore, future clinical research with long-term follow-up is needed to evaluate this technique’s indications and clinical efficacy in shoulder, hip, and elbow cartilage injuries.
Since OCA is mainly used for knee cartilage defects, the overall clinical characteristics and results of OCA are similar to the knee. For OCA of the knee, our analysis showed the mean age of the patients was 34 years, and 61% were male. Therefore, OCA is suitable for young, athletic male patients, because they want to restore high activity levels. Studies have shown less effective outcomes in patients with OCA >30 years of age.24,124 OCA grafts are likely to fail in older adults due to other combined confounders, such as concurrent disease and prior surgeries; therefore, surgeons tend to perform total knee arthroplasty to achieve generally good results for these patients.38,85,123 The studies we reviewed showed that patients treated with knee OCA had a mean BMI of 26.7 kg/m2. For some obese patients, OCA can also provide a successful option for the medium-term treatment of knee cartilage defects. 140 Our analysis showed that knee cartilage defects mainly occurred in the medial femoral condyle.
Articular cartilage defects in the knee can be caused by various factors such as trauma, degeneration, avascular necrosis, osteochondritis dissecans, or osteoarthritis. The principal diagnosis in patients treated with OCA is osteochondritis dissecans. Therefore, osteochondritis dissecans is the best indication for OCA, followed by degenerative lesions and acute trauma. 86 Furthermore, we found that common surgical procedures included chondral debridement and MSTs before knee OCA surgery. Traditionally, because of the expensive and complicated nature of OCA, it is often considered a second-line treatment after debridement or MST failures, and some authors believe that previous debridement and MST affects the outcome of OCA and suggest considering OCA as the preferred first-line treatment. 111 Studies analyzing the impact of various previous cartilage repair surgeries on the outcomes of OCA concluded that OCA can be a salvage surgical treatment after the failure of previous cartilage repair surgery.51,141
We found that the most common concomitant procedures were HTO and MAT. As knee joints with varus deformity accelerate the degeneration of the surrounding cartilage and joints by increasing their mechanical load, HTO is increasingly used as an auxiliary surgery for cartilage repair by optimizing the biomechanical microenvironment in the medial compartment. Several studies have shown that combining HTO and OCA is safe and effective for treating knee cartilage injury and has achieved satisfactory clinical results.3,8,65,81 Meniscal loss leads to the development of cartilage lesions, and MAT and OCA are considered symbiotic surgeries due to their complementary indications and contraindications. 41 Most patients who had failed knee OCA underwent total knee arthroplasty. This suggests that total knee arthroplasty is the preferred treatment after cartilage repair failure. 69 Our data analysis showed a mean failure rate after knee OCA of 16.8%. Matthews et al 86 described 5- and 10-year survival rates of 95% and 85%, respectively, after knee OCA, consistent with the results of this review. Studies have reported overall satisfaction with 88.1% of knee OCA, and the satisfaction of patients who underwent OCA for osteochondritis dissecans could be as high as 95.6%. 132
For OCA of the ankle, our analysis showed the mean age of the patients was 39 years, and 61% were male. Ankle cartilage defects mainly occurred in the medial talus, followed by the lateral, with the fewest cases concerning the central region. The distribution pattern of talar osteochondral lesions described by Dahmen et al 27 and van Diepen et al 133 agrees with the analysis in this review. Our data analysis showed that the mean failure rate after ankle OCA reached 26.2%.
And analysis demonstrated allograft survivorship of 78.1% at 5 years and 62% at 10 years, with an overall patient satisfaction rate of 76.7%. Higher failure rates and lower allograft survival rates were observed in the ankle than in the knee at 5 and 10 years after OCA. Further extensive studies are needed to analyze the causes of ankle osteochondral allograft postoperative failure compared with the knee. 118
Many studies have described graft storage methods, but there is a lack of consensus regarding the optimal storage conditions for osteochondral allografts. Regarding the graft preservation temperature, frozen allografts are thought to lack chondrocyte activity and decrease cartilage viability, leading to inferior clinical outcomes compared with fresh allografts. Therefore, freshly stored grafts are the preferred surgical choice.20,61,119,126 We found that the most commonly used preservation protocol for clinical grafts is the standard hypothermic protocol (4°C). It has been shown that the grafts were significantly improved when stored at 22°C to 25°C or 37°C compared with a storage temperature of 4°C, yet some studies have also shown opposing results60,125; thus, these temperatures cannot be used to determine the optimal preservation temperature. 126 Regarding allograft storage and methodology, different countries have different conservation programs. The optimal approach for allograft preservation before OCA remains controversial; studies have shown that chondrocyte viability is greatly reduced when the allograft is stored beyond 15 days, and chondrocytes survive up to 28 days before implantation.20,91 The short allograft preservation period causes logistical problems, such as donor tissue acquisition, transportation, processing, and time constraints. These logistical problems before the donor graft transplant and the high cost of the graft have seriously limited the use of OCA.48,86,126 Therefore, more intensive scientific research on safe and effective storage processes and methods of allografts can improve current practices, thus improving the clinical availability of OCA surgery.
Limitations
This study has some limitations. The primary limitation was the high heterogeneity of included studies. Due to limited available data, clinical control studies comparing OCA and other surgical procedures, follow-up studies on clinical outcomes solely on OCA, and all other clinical studies related to OCA were included in the analysis. Therefore, the overall quality of the included studies was relatively low. Second, due to the different focuses of clinical outcomes of OCA in different studies, the evaluation protocol for clinical outcomes could not be precisely quantified. Finally, data on failure details and complications were lacking, and the causes of failure could not be analyzed separately. Therefore, more high-quality, high-sample, multicenter randomized controlled trials for the clinical application of OCA could provide a more accurate evaluation of OCA’s clinical efficacy.
Conclusion
OCA has attracted significant research interest over the past 20 years, and the overall annual number of patients undergoing the procedure showed a significant upward trend, especially from 2016 to 2020. A majority of studies have been conducted in the United States. Patients receiving OCA were predominantly overweight, young adults, with most having had previous surgery at the same surgical site. The use of OCA is more established for cartilage injury in the knee than in other sites, and its best indication based on outcomes is osteochondritis dissecans. The results of our analysis demonstrated satisfactory long-term postoperative outcomes of OCA at all locations. More basic and clinical scientific research can improve the availability of OCA surgery in clinics and articular cartilage at other sites.
Footnotes
Final revision submitted April 6, 2023; accepted May 3, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (grants U21A20353 and 82172503), the Central Government Guides Local Science and Technology Development Funds (grant YDZJSX2022B011), and the Key Research and Development Program of Shanxi Province (grant 201903D421019). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.