
Abstract
Background:
Meniscal root repair can improve patient outcomes significantly; however, several contraindications exist, including arthritic change to the medial or lateral tibiofemoral compartments.
Purpose/Hypothesis:
The purpose of this study was to evaluate the outcomes of meniscal root repair in patients with advanced patellofemoral chondromalacia (PFC). It was hypothesized that the presence of advanced PFC would not significantly affect the postoperative outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was conducted of patients who underwent meniscal root repair with at least 2 years of follow-up data. Patients with chondromalacia as determined by arthroscopic visualization (defined as Outerbridge grade 3 or 4) were placed in the PFC group; patients with Outerbridge grade 0 to 2 chondromalacia were placed in the non-PFC group. Outcomes were measured by the Lysholm knee scoring scale and the International Knee Documentation Committee (IKDC) Subjective Knee Form. Clinical outcomes including complications were also recorded. Quantitative data between the groups were analyzed using the 2-tailed independent-samples t test.
Results:
Overall, this study included 81 patients (35 in the PFC group, 46 in the non-PFC group). The mean follow-up times were 25.1 months in the PFC group and 24.8 months in the non-PFC group. In both groups, Lysholm and IKDC scores improved significantly with 24-month Lysholm scores averaging 85.86 in the PFC group and 86.61 in the non-PFC group (P = .62) and 24-month IKDC scores averaging 77.66 for the PFC group and 79.59 for the non-PFC group (P = .45). The cohorts demonstrated similar rates of retear, arthrofibrosis, infection, and progression to total knee arthroplasty.
Conclusion:
The presence of advanced PFC was not associated with inferior outcomes in patients who underwent posterior meniscal root repair, and rates of recurrent tears, postoperative infection, arthrofibrosis, and conversion to total knee arthroplasty were similar between the study groups. These findings suggest that PFC may not significantly alter the results of meniscal root repair and should not be considered an absolute contraindication for this procedure.
The meniscus plays a major role in the health and proper functioning of the knee joint in various roles including shock absorption and dissipation of stresses across the knee joint. 3,5,22,23,28 In order to function appropriately, meniscal root integrity is paramount. 2,30 Damage to the meniscal roots occurs in up to 21% of all meniscal tears and increases force across the femoral-tibial cartilage due to loss of circumferential hoop stress. 7,14,29 It has been shown that peak contact pressures increase and contact area decreases in both the medial and lateral compartments in response to meniscal root disruption. 1,18,19
There has been a growing interest in operative intervention for meniscal root tears as this injury has been associated with the development of accelerated knee arthritis. Specifically, meniscal root tears have been shown to accelerate the breakdown of cartilage in the affected compartment with biomechanical changes that can mimic a complete meniscectomy. 1 Not surprisingly, it has been demonstrated that these injuries significantly increase the risk of total knee arthroplasty (TKA) if left unaddressed. 2,14,29 Repairing meniscal root tears may be beneficial in improving patient symptoms and outcomes after injury. Several studies have shown that meniscal root repair is superior to meniscectomy in terms of osteoarthritis progression and the need for eventual TKA in this patient cohort. 2,10,14
Among other patient factors, the presence of advanced chondromalacia in the tibiofemoral joint has been thought to lead to poor outcomes after meniscal root repair. 6,20 Despite the prior dogma that arthritis in the medial or lateral compartments portends a poor response to repair, the consequence of chondromalacia to the patellofemoral joint remains unknown. The purpose of this study was to evaluate the outcomes of meniscal root repair in patients with and without Outerbridge grade 3 and 4 patellofemoral chondromalacia (PFC). We hypothesized that the presence of advanced PFC would not significantly affect the outcomes of meniscal root repair.
Methods
Study Design and Cohort
Institutional review board approval was obtained for the study protocol. A retrospective review was performed for patients who underwent meniscal root repair by a single surgeon (K.J.E.) between January 2016 and December 2019. Patients were included in the study if they underwent either posterior meniscal root repair of either the medial or lateral side, were between the ages of 18 and 75 years, and had at least 2 years of follow-up data. Excluded were patients with concomitant knee procedures, such as anterior cruciate ligament (ACL) reconstruction or meniscectomy/meniscal repair, advanced chondromalacia of the tibiofemoral joint (Outerbridge grade 3-4), history of ipsilateral knee surgery, revision meniscal root repair, history of inflammatory arthritis, or follow-up shorter than 2 years. Patients were grouped according to the degree of chondromalacia of the patellofemoral joint. Patients with Outerbridge grade 0 to 2 chondromalacia as determined by arthroscopic visualization were placed in the non-PFC group, and those with Outerbridge grade 3 to 4 were placed in the PFC group.
Surgical Procedure
Each patient underwent the procedure in the supine position. General anesthesia was used in each case without regional block. A tourniquet was used in all cases to allow clear visualization. Diagnostic arthroscopy was performed through standard anterior-lateral and anterior-medial portals. The patellofemoral joint was evaluated first. Chondromalacia was noted under the patella and trochlea using the Outerbridge grading system. 27 In the setting of either grade 3 or 4 chondromalacia, no shaving chondroplasty was performed. Instead, loose bodies were removed if present. After evaluation of the patellofemoral joint, the medial joint space was evaluated with the knee on valgus stress. Chondromalacia of the medial femoral condyle and medial tibial plateau were graded using the Outerbridge classification. The medial meniscus was then evaluated with a probe. The posterior horn of the meniscus was specifically probed to determine the stability of the meniscal root. Meniscal root tears were confirmed by visualizing a complete radial tear through the posterior meniscus <1 cm from the physical attachment of the meniscus to its bony attachment. Complete meniscal root tearing was confirmed by visualizing the meniscal root being pulled away from its footprint during probing by the surgeon. Once the medial compartment was evaluated, the process was repeated in the lateral compartment with the knee in a figure-of-4 position. If a meniscal root tear was confirmed, repair was not performed until the diagnostic arthroscopy was completed in both compartments.
Surgical repair of the meniscal root was performed via a transtibial pull-though technique. Tears of the medial meniscal root were performed while the knee was on valgus stress. If visualization of the posterior meniscal root was difficult due to tightness of the medial compartment, a medial collateral ligament (MCL) release was performed using an 18-gauge needle for a pie-crusting technique. 25 Lateral meniscal root repairs were performed with the knee in a figure-of-4 position. To begin the repair, 2 number 2 FiberWire sutures (Arthrex) were placed in the lateral 2 cm of the posterior horn of the meniscus using an Arthrex Meniscal Scorpion device. Both sutures were placed in a luggage-handle fashion. Next, a meniscal root guide was placed in the center of the posterior horn footprint. A 6-mm Flipcutter (Arthrex) was then drilled into the center of the footprint then deployed and a 10-mm-deep socket was then created. A FiberStick (Arthrex) was then placed up through the anterior tibial cortex and into the socket made by the Flipcutter. The FiberStick suture was then pulled out the anterior-medial portal. The number 2 FiberWire sutures previously passed through the meniscus were then placed in the loop of the Fiberstich and pulled through the anterior cortex of the tibia. This brought the meniscal root into the socket. With the knee extended, a 4.75-mm Swivellock (Arthrex) was used to anchor the sutures to the anterior cortex stabilizing the meniscus in its socket.
Postoperative Rehabilitation
After surgery, patients were placed in an X-Act ROM Knee (DonJoy) locked in extension. Patients were placed on crutches and allowed to ambulate toe-touch weightbearing in the brace locked in extension for 6 weeks. Formal physical therapy was started at 10 to 14 days after surgery. Range of motion (ROM) was limited to 90° of flexion for the first 6 weeks. The brace was discontinued at 6 weeks, and weightbearing and ROM were allowed as tolerated. Activities were increased to an as-tolerated basis at 3 months. Sports-specific activities were added between months 4 and 6.
Patient Demographics
The chart of each patient included in the study was evaluated. Demographic information on each patient including age, sex, and body mass index (BMI) were collected. Side of procedure and laterality of the meniscal root repair were also noted. The amount of chondromalacia in the trochlea and under the patella was also documented. Complications including recurrent tears, infection, arthrofibrosis, and conversion to TKA were extracted via retrospective chart review.
Outcome Measures
The Lysholm knee scoring scale and the International Knee Documentation Committee (IKDC) Subjective Knee Form were used to quantify patient-reported outcomes preoperatively and at 6, 12, and 24 months postoperatively. Clinical outcomes and complications, such as meniscal root retearing, infection, arthrofibrosis, and conversion to TKA, were also noted.
Statistical Analysis
Quantitative data were analyzed using a 2-tailed independent-samples t test for continuous data. The chi-square test was used for normative data. Significance was determined at the alpha level of 0.05. Statistical analysis was performed with Excel
Results
Overall, 116 meniscal root repairs were performed during the 3-year study period. Of these, 12 patients were excluded due to concomitant procedures (all ACL reconstructions), 10 were excluded for having advanced tibiofemoral chondromalacia, and 13 patients did not have 2 years of follow-up data. Thus, 81 meniscal root repairs were included in the study (Figure 1). Of these 81 patients, 35 had advanced chondromalacia of the patellofemoral joint, making up the PFC group, and 46 did not, constituting the non-PFC group (Figure 2). The demographics of the 2 groups were similar with regard to age, sex, BMI, and side of procedure (Table 1). The groups were also comparable with regard to Outerbridge scores of the medial and lateral tibiofemoral compartments.
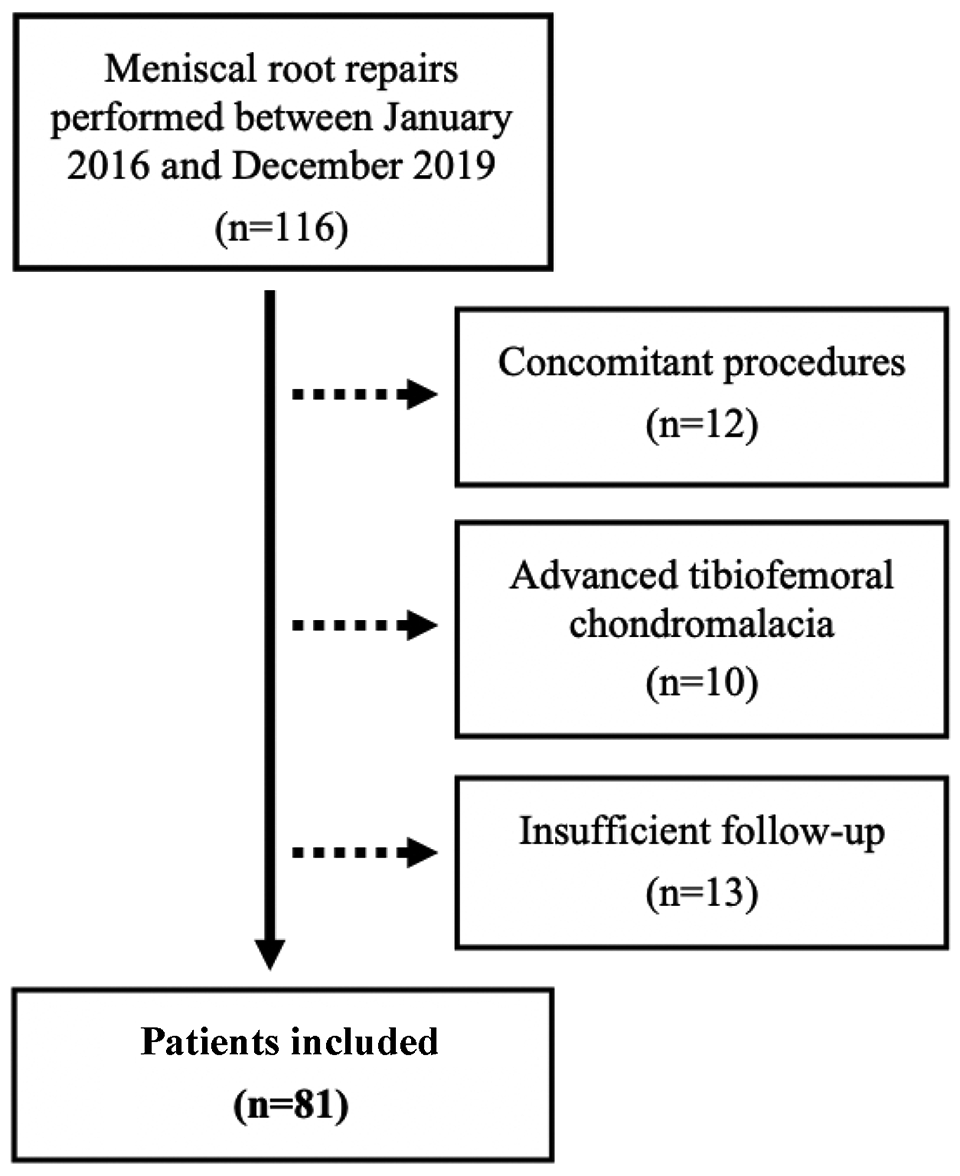
Flowchart of patient selection.

Outerbridge classifications by group. PFC, patellofemoral chondromalacia cohort; NPFC, non–patellofemoral chondromalacia cohort.
Patient Characteristics According to Study Group a

a Boldface P value indicates statistically significant difference between groups (P < .05). BMI, body mass index; LC, lateral compartment; MC, medial compartment; PFC, patellofemoral chondromalacia.
The site of advanced chondromalacia within the patellofemoral joint was identified for patients in the PFC group; 51.9% of cases of advanced PFC involved the patella, 66.7% involved the trochlea, and 18.6% involved both structures. Overall, the average Outerbridge score of the patellofemoral joint was 3.77 for the PFC group and 1.63 for the non-PFC group (P < .001) (Table 1). In addition, Outerbridge scores were stratified by site for the 2 groups. The mean Outerbridge score for the patella was 3.2 in the PFC group and 1.8 in the non-PFC group (P < .001). The mean Outerbridge score of the trochlea was 3.4 and 1.7 in the PFC and non-PFC groups, respectively (P < .001).
The preoperative Lysholm and IKDC scores did not significantly differ between groups, and patients in both groups saw improvement in scores at 6, 12, and 24 months postoperatively (Table 2). The average increase in Lysholm score for the PFC group was 36.23 over 2 years, and the average 24-month increase in Lysholm scores for the non-PFC group was 37.50. Similarly, IDKC scores improved by 31.23 and 35.13 on average from preoperative measurement to 2-year follow-up for the PFC and non-PFC groups, respectively. There were no significant between-group differences in mean Lysholm and IKDC scores at any postoperative time point (Table 2). Final Lysholm scores averaged 85.86 in the PFC group and 86.61 in the non-PFC group (P = .62). Final IKDC scores were 77.66 for the PFC group and 79.59 for the non-PFC group after meniscal root repair (P = .45).
Patient-Reported Outcome Scores According to Study Group a

a IKDC, International Knee Documentation Committee Score; PFC, patellofemoral chondromalacia; postop, postoperative; preop, preoperative.
Clinically relevant complications after meniscal root repair were reported in Table 3. A total of 3 retears occurred in the study including 2 in the non-PFC group and 1 in the PFC group (P = .73). One patient converted to TKA at the 2-year follow-up in the PFC group and none in the non-PFC group (P = .25). A single, superficial infection occurred in the non-PFC group and was successfully treated with oral antibiotics. No infections occurred in the PFC group. Arthrofibrosis requiring manipulation and lysis of adhesions occurred in 1 patient in each group.
Clinical Outcomes According to Study Group a

a PFC, patellofemoral chondromalacia; TKA, total knee arthroplasty.
Discussion
The goal of this study was to evaluate the outcomes of meniscal root repair in patients with PFC. In this series, the presence of advanced PFC did not lead to significantly inferior outcomes in terms of the Lysholm or IKDC scores in patients undergoing meniscal root repair when compared with those without PFC. The groups also did not demonstrate significantly different rates of rerupture or infection at 2 years of follow-up. Lastly, those with and without PFC had similar rates of conversion to TKA.
Meniscal root injuries are an increasingly recognized pathology that portends significant functional limitations and cartilage degeneration. Repair is typically indicated in acute injuries in the young and active population with minimal to no existing arthritis. However, these injuries are more likely to occur in the subacute or degenerative setting in the middle-aged population. 24,26 Accordingly, it is important to understand the interaction that concomitant degenerative pathologies share with meniscal root management. In this series of patients with and without PFC, outcome scores including the Lysholm and IKDC were similar at every time point. At 2 years of follow-up, Lysholm improvement in the PFC and non-PFC groups was 36.3 and 37.5, respectively, both of which exceed the reported minimal clinically important difference of 10.1. 4,13 Similarly, improvements in the IKDC outcome score exceeded 30 in both cohorts, which meets the reported minimal clinically important difference values that range between 3.19 and 16.7. 8,11 Taken together, our results suggest that the presence of PFC does not compromise the clinical benefit that can be afforded from meniscal root repair.
Clinical outcomes such as retear rate, infection, and arthrofibrosis were also collected and did not significantly differ between the 2 groups at final follow-up. Specifically, meniscal root tears recurred in 1 (2.9%) in the PFC group and 2 (4.3%) of the non-PFC group. These rates are similar to reports in the current literature with estimates of meniscal root retear or tear failure rate at 4.97%. 9 Other complications included 1 superficial infection managed with oral antibiotics in the non-PFC group and 1 case of arthrofibrosis requiring lysis of adhesions in each cohort. In total, rates of these complications were similar between the 2 groups at 5.7% and 6.5% for the PFC and non-PFC cohorts, respectively. Again, these are comparable to previous reports in the literature as noted by LaPrade et al, 21 who reported a 6.7% rate of overall revision surgery in patients undergoing medial meniscal root repairs at 2 years of follow-up. These results suggest that the presence of PFC does not independently increase the risk for complications at 2 years of follow-up.
Meniscal root tears are associated with accelerated progression of osteoarthritis and the need for eventual TKA. 14,17 It has been reported that when managed with meniscectomy alone, over half of these patients progress to requiring a TKA at 5 years postoperatively. 16 In our series, though 1 patient in the PFC group progressed to requiring TKA, this result was not significant when compared with the non-PFC cohort. Of note, this patient had advanced chondromalacia of both the patella and trochlea. It is difficult to extrapolate conclusions on the rate of TKA conversion as previous reports on the topic have included at least 5 years of follow-up. However, our data provide preliminary data to suggest that those with PFC do not rapidly progress to requiring TKA after meniscal root repair compared with those patients without advanced PFC.
Indications and technique for meniscal root repair continue to expand. Two main techniques exist, including the suture anchor and transtibial techniques. The senior author of this investigation (K.J.E.) utilizes the transtibial pull-out repair technique that has been shown to be economically effective in addition to beneficial for patient outcomes. 12 Indications and contraindications for meniscal root tears continue to be developed. Acute tears are generally indicated for repair in the absence of contraindications including BMI >30 kg/m2, untreated instability, significant malalignment, subchondral collapse, or grade 3+ changes. 15 Indications for repair in the chronic degenerative setting continue to develop as the optimal patient factors are not fully established. Our results demonstrate that PFC, in isolation, should not serve as a contraindication to repair as patients with this entity demonstrated comparable improvement and complication rates when compared with a cohort without the pathology.
Limitations
This study has several limitations. It is somewhat limited by sample size and therefore statistical power. The retrospective nature of this study also restricts the variables available for analysis, and this study did not include biomechanical factors. Though the single surgeon (K.J.E.) affords consistency, it does limit external validity as different repair techniques or patient populations may influence the results. As the presence of chondromalacia is a spectrum, an arbitrary cutoff of 0 to 2 and 3 to 4 was required to create 2 comparative groups. Although this is inherently subjective, grading was performed arthroscopically by an experienced sports medicine–trained surgeon.
Conclusion
The presence of advanced PFC did not lead to significantly inferior outcomes in patients undergoing posterior meniscal root repair. Patient-reported outcomes were similar between patients with and without advanced PFC at 2 years of follow-up. Furthermore, rates of recurrent tears, postoperative infection, arthrofibrosis, and conversion to TKA were similar between groups. These findings suggest that PFC does not significantly alter the results of meniscal root repair and should not necessarily be considered a contraindication.
Footnotes
Final revision submitted April 10, 2023; accepted April 27, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.V.T. has received education payments from ImpactOrtho. K.J.E. has received education payments and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from WCG IRB (study No. 1322973).