
Abstract
Background:
Operative treatment of displaced tibial spine fractures consists of fixation and reduction of the fragment in addition to restoring tension of the anterior cruciate ligament.
Purpose:
To determine whether residual displacement of the anterior portion of a tibial spine fragment affects the range of motion (ROM) or laxity in operatively and nonoperatively treated patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were gathered from 328 patients younger than 18 years who were treated for tibial spine fractures between 2000 and 2019 at 10 institutions. ROM and anterior lip displacement (ALD) measurements were summarized and compared from pretreatment to final follow-up. ALD measurements were categorized as excellent (0 to <1 mm), good (1 to <3 mm), fair (3 to 5 mm), or poor (>5 mm). Posttreatment residual laxity and arthrofibrosis were assessed.
Results:
Overall, 88% of patients (290/328) underwent operative treatment. The median follow-up was 8.1 months (range, 3-152 months) for the operative group and 6.7 months (range, 3-72 months) for the nonoperative group. The median ALD measurement of the cohort was 6 mm pretreatment, decreasing to 0 mm after treatment (P < .001). At final follow-up, 62% of all patients (203/328) had excellent ALD measurements, compared with 5% (12/264) before treatment. Subjective laxity was seen in 11% of the nonoperative group (4/37) and 5% of the operative group (15/285; P = .25). Across the cohort, there was no association between final knee ROM and final ALD category. While there were more patients with arthrofibrosis in the operative group (7%) compared with the nonoperative group (3%) (P = .49), this was not different across the ALD displacement categories.
Conclusion:
Residual ALD was not associated with posttreatment subjective residual laxity, extension loss, or flexion loss. The results suggest that anatomic reduction of a tibial spine fracture may not be mandatory if knee stability and functional ROM are achieved.
Tibial spine fractures represent an avulsion injury of the anterior cruciate ligament (ACL) with its insertion onto the tibia. Treatment of tibial spine fractures is based upon the degree of displacement as classified by the Meyers and McKeever system. 14 Type 1 fractures are nondisplaced and treated nonoperatively. Type 3 fractures are fully displaced, and type 4 fractures are fully displaced with comminution 19 ; both are typically treated with arthroscopic or open reduction. 11,13 Treatment of type 2 fractures can be controversial, but recent studies have shown that operative treatment of type 2 fractures results in improved stability but higher rates of arthrofibrosis, while nonoperative treatment leads to more motion but decreased stability and increased rates of ACL reinjury. 1,3,15,16 The goal of operative treatment is 2-fold, to restore the stability and tension of the ACL and to reduce the fracture as anatomically accurately as possible.
Techniques for fracture reduction include interfragmentary screw fixation or suture fixation through the ACL footprint. Occasionally, these techniques may not achieve an anatomic reduction or may cause deformation of the tibial eminence fragment, in both instances resulting in the fracture fragment having residual anterior elevation or displacement. The significance of this “anterior lip” has not been examined, but the resulting displacement has been thought to interfere with full range of motion (ROM) of the knee. 17
The purpose of this study was to investigate any association between the quality of tibial spine fracture reduction and motion loss and/or residual laxity. It was hypothesized that residual anterior lip displacement (ALD) at the final follow-up visit would not have an effect on residual laxity or ROM in patients, regardless of whether they undergo operative or nonoperative treatment.
Methods
Patients
This was a multicenter institutional review board-approved study conducted at 10 institutions across the United States. A query was performed to identify all patients aged <18 years who were evaluated at participating sites with a tibial spine fracture between January 1, 2000, and January 31, 2019. To eliminate confounding from polytrauma, patients with additional lower extremity fractures were excluded from the study. A review of patient medical records was performed to record patient demographic characteristics, clinical and surgical variables, and the incidence and subsequent outcomes of patients who developed complications after their tibial spine fracture treatment. Patients who had follow-up radiographic anterior displacement measurements and at least 3 months of follow-up ROM measurements were included. This resulted in 328 patients in the final cohort.
Patient Characteristics
Demographic, clinical, surgical, and radiographic data were collected retrospectively from patient medical records. Demographic data included age at presentation, sex, and race/ethnicity. Clinical data included date of injury, dates of visits for tibial spine care, clinical notes, and vital sign measurements taken at clinic visits. Injury characteristics, such as mechanism of injury, ROM, laxity (defined as a positive Lachman, anterior drawer, or pivot shift), effusion, and tenderness, were collected from clinic notes. Surgical decision-making was based upon individual provider indications but generally included gross displacement of the tibial spine. Surgical data included operative notes, surgery-related variables, and any complications during follow-up. Relevant intraoperative times were also recorded, including time of incision, time of procedure start and end, and time leaving the operating room. We defined arthrofibrosis as >5° of extension loss and/or a lack of knee flexion past 100° compared with the contralateral knee at 3 months after treatment.
Radiographic Imaging and Analysis
Standard-of-care imaging related to diagnosis and care for the patient’s tibial spine fracture were reviewed from the patient’s medical record. Magnetic resonance imaging scans and radiographs were analyzed to collect growth plate status, ALD of the tibial spine, and additional injuries to the knee. ALD was measured from the top of the fragment to the tibial plateau anteriorly on the lateral radiograph (Figure 1). 7 The accuracy and reproducibility of the ALD measurements have been demonstrated in a previous study by this author group. 7 In addition, the residual ALD measurements were categorized as excellent (0 to <1 mm), good (1 to <3 mm), fair (3 to 5 mm), or poor (>5 mm).

Measurement of ALD. The red line indicates the top of the tibial plateau with the top of the displaced fragment. This measurement was 6 mm and would be classified as poor. ALD, anterior lip displacement.
Statistical Analysis
Patient demographics, injury characteristics, and outcomes were summarized for the cohort. Continuous variables were summarized as means and standard deviations or the median and interquartile range where appropriate, based on normality of data distribution. Categorical variables were summarized by frequency and percentage. Bivariate analysis was done using chi-square test and independent-samples Student t test to compare patient demographics and outcomes between treatment groups. ROM and ALD measurements were summarized and compared from pretreatment to the final follow-up. The change in measurement was calculated from pretreatment to final follow-up, and the Wilcoxon signed-rank test was used to compare continuous variables. The McNemar test was used for binary variables in comparing proportions from before treatment with those from final follow-up.
Logistic regression was utilized to determine whether there was a significant association between ALD category and laxity, controlling for surgery, and analysis of variance was used to determine association between ALD category and final ROM measurements.
A subanalysis was conducted on patients in the operative group (n = 290), first looking at ROM measurements and contracture data. Kruskal-Wallis tests were used to determine whether there was at least 1 median ROM measurement from the ALD category that was different from the median of at least 1 of the other ALD categories. Post hoc pairwise Mann-Whitney tests with a Bonferroni correction were utilized to determine which specific ALD category measurements differed significantly from one another. Logistic regression was utilized to determine whether ROM measurements or laxity were associated with having a complication. A P value <.008 was considered significant for post hoc tests, while all other tests were considered significant if the P value was ≤.05. All comparative statistical analyses were 2-tailed. Statistical analysis performed with SAS (Version 9.4, SAS Institute).
Results
Of 580 initially identified patients, 328 patients were included in the study cohort (Figure 2). The mean age at the time of injury was 11.7 years (range, 5.09-17.85 years), and 63% of the cohort was male (207/328). In all, 88% (290/328) of patients had operative treatment, while 12% of patients (38/328) had nonoperative treatment. Tables 1 and 2 show the patient and injury characteristics of the patients overall and by treatment group. The only significant difference in demographics between the groups was that patients who underwent nonoperative treatment were slightly younger compared with those who underwent operative treatment (10.8 vs 11.8 years; P = .04).

Flowchart of patient inclusion and anterior lip displacement category.
Patient Characteristics Overall and by Treatment Group a

a Data are shown as mean ± SD or n (%). Boldface P value indicates statistically significant difference between groups (P ≤ .05). BMI, body mass index.
b Number of patients with available data for the given characteristic.
Injury Characteristics Overall and by Treatment Group a
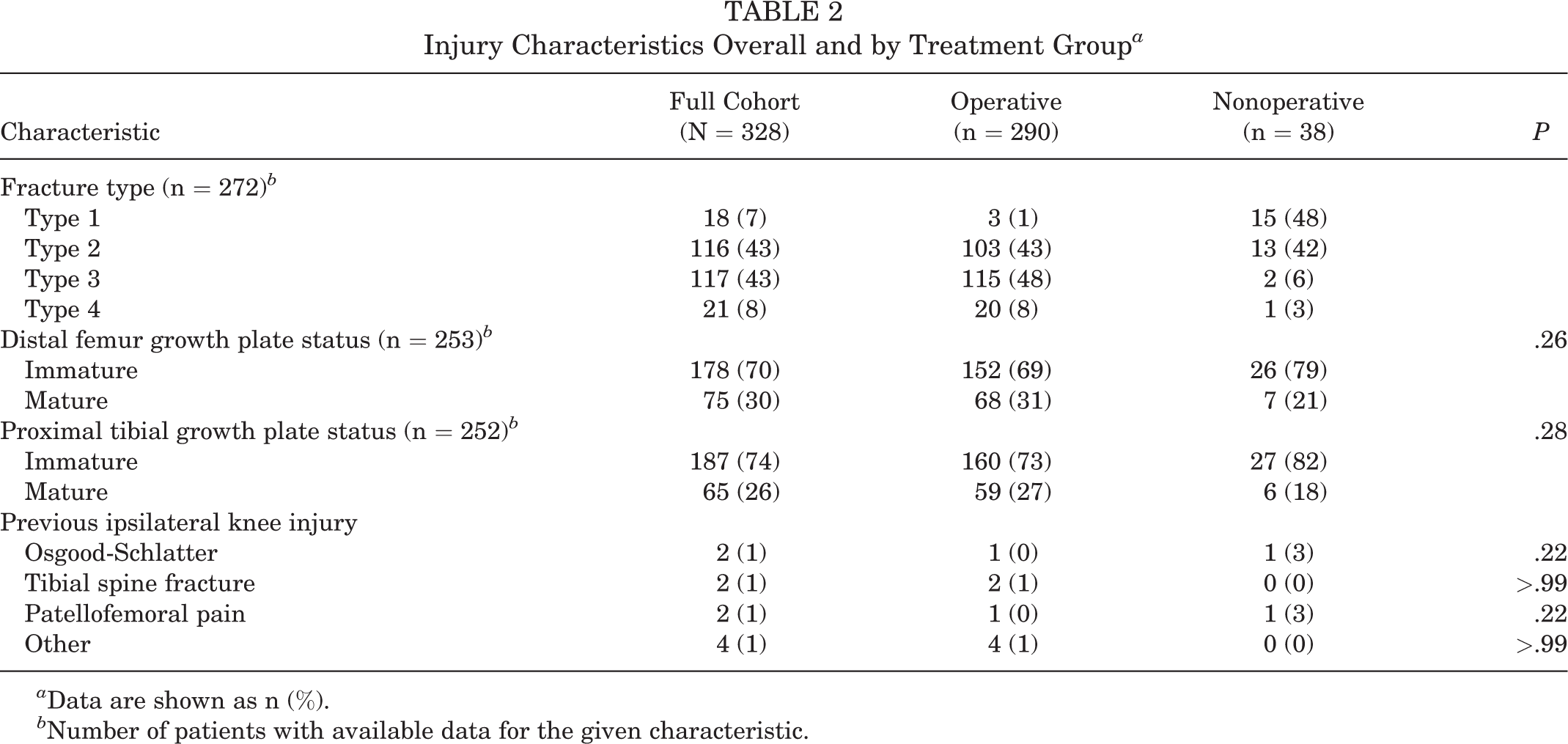
a Data are shown as n (%).
b Number of patients with available data for the given characteristic.
Immobilization in hyperextension, full extension or 15° was the most frequent treatment (97%) in the nonoperative group while the majority of patients in the operative group (87%) received arthroscopic reduction and internal fixation. There were 177 patients (61%) who underwent suture fixation, 72 (25%) who had screw fixation, and 27 patients (9%) who had both suture and screw fixation. Although there was not a standardized protocol, the majority of patients were not cast immobilized in full knee extension postoperatively but rather utilized a gradated ROM protocol. The median time to final ROM measurements for the operative group was 8.1 months (range, 3.02-151.66 months) and the median time to final radiographic measurement was 4.0 months from surgery (range, 0.13-91.86 months). The nonoperative group had a median time of 6.7 months to final ROM measurement (range, 3.02-71.75 months) and 3.9 months to final radiographic measurement (range, 0.59-55.13 months).
The median ALD measurement for all patients was 6.0 mm before treatment and decreased to 0 mm after treatment (P < .001). At final follow-up, residual ALD was categorized as excellent in 203/328 (62%), good in 49/328 (15%), fair in 60/328 (18%), and poor in 16/328 (5%) patients (Figure 2). The breakdown of final outcomes between treatment groups is listed in Table 3. There were no between-group differences in the final ALD measurements. At the final follow-up, over half (62%; 203/328) were categorized in the excellent group for the ALD measurement compared with 5% (12/264) pretreatment (Table 4). We also performed a subanalysis of patients in the operative group who underwent suture fixation (n = 177) compared with screw fixation (n = 72), and the final residual anterior displacement measurements yielded a similar distribution of patients in each category (excellent, 63% vs 63%; good, 15% vs 11%; fair, 18% vs 22%; and poor, 4% vs 4%).
Outcomes Overall and by Treatment Group a
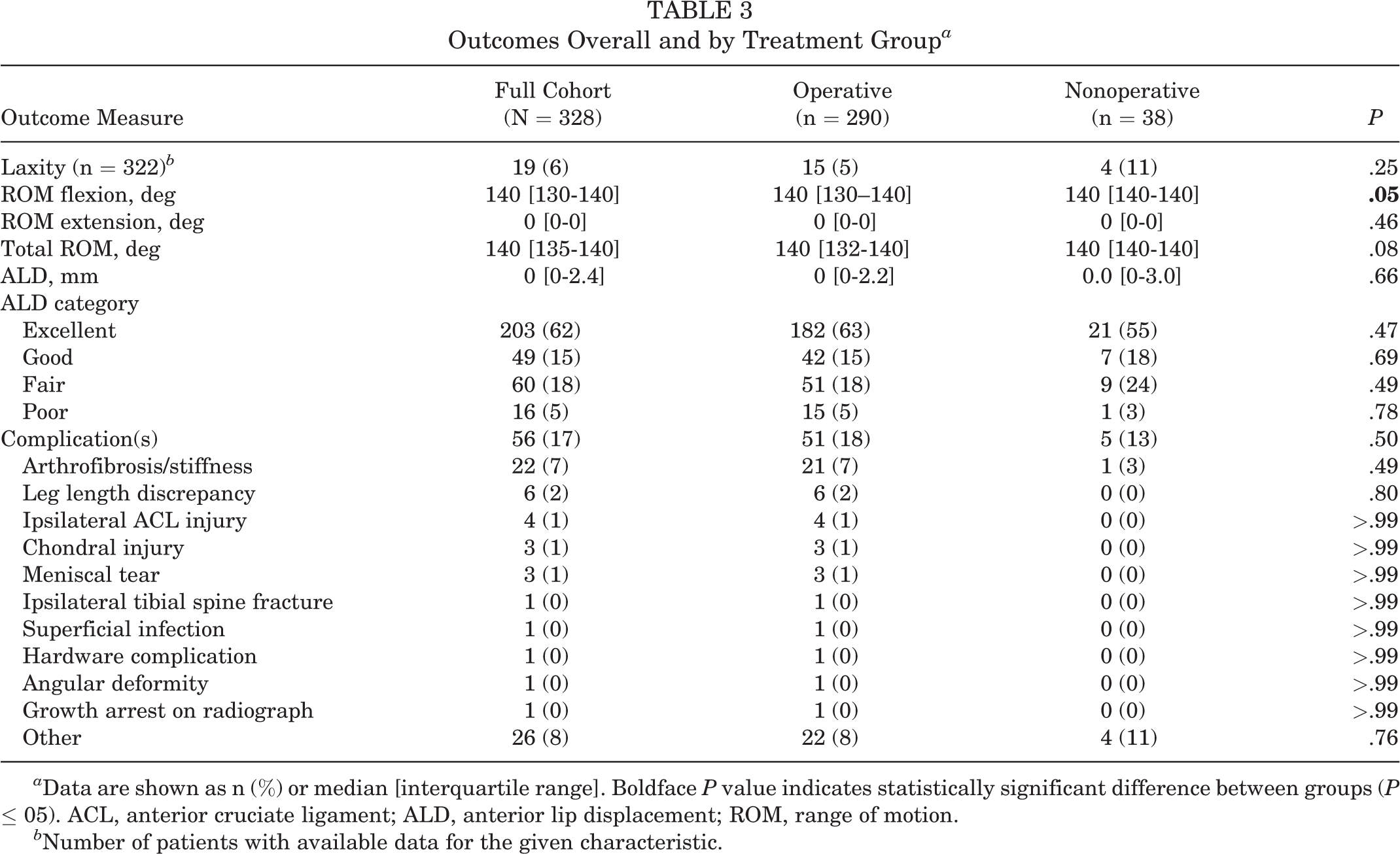
a Data are shown as n (%) or median [interquartile range]. Boldface P value indicates statistically significant difference between groups (P ≤ 05). ACL, anterior cruciate ligament; ALD, anterior lip displacement; ROM, range of motion.
b Number of patients with available data for the given characteristic.
Outcomes From Pretreatment to Final Follow-up a

a Data are shown as n (%) or median [interquartile range] unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P ≤ .05). Dashes indicate areas not applicable. ALD, anterior lip displacement; ROM, range of motion.
Laxity
A total of 11% of patients in the nonoperative group had a positive finding of laxity (4/37) and 5% had a positive finding of laxity in the operative group (15/285; P = .25) (Table 3). Across the entire cohort within each residual ALD group, there was no difference between the groups (Table 5). There were 9 patients who underwent delayed ACL reconstruction in the operative group and 1 patient in the nonoperative group.
Outcomes by Final ALD Category Stratified by Treatment Group a
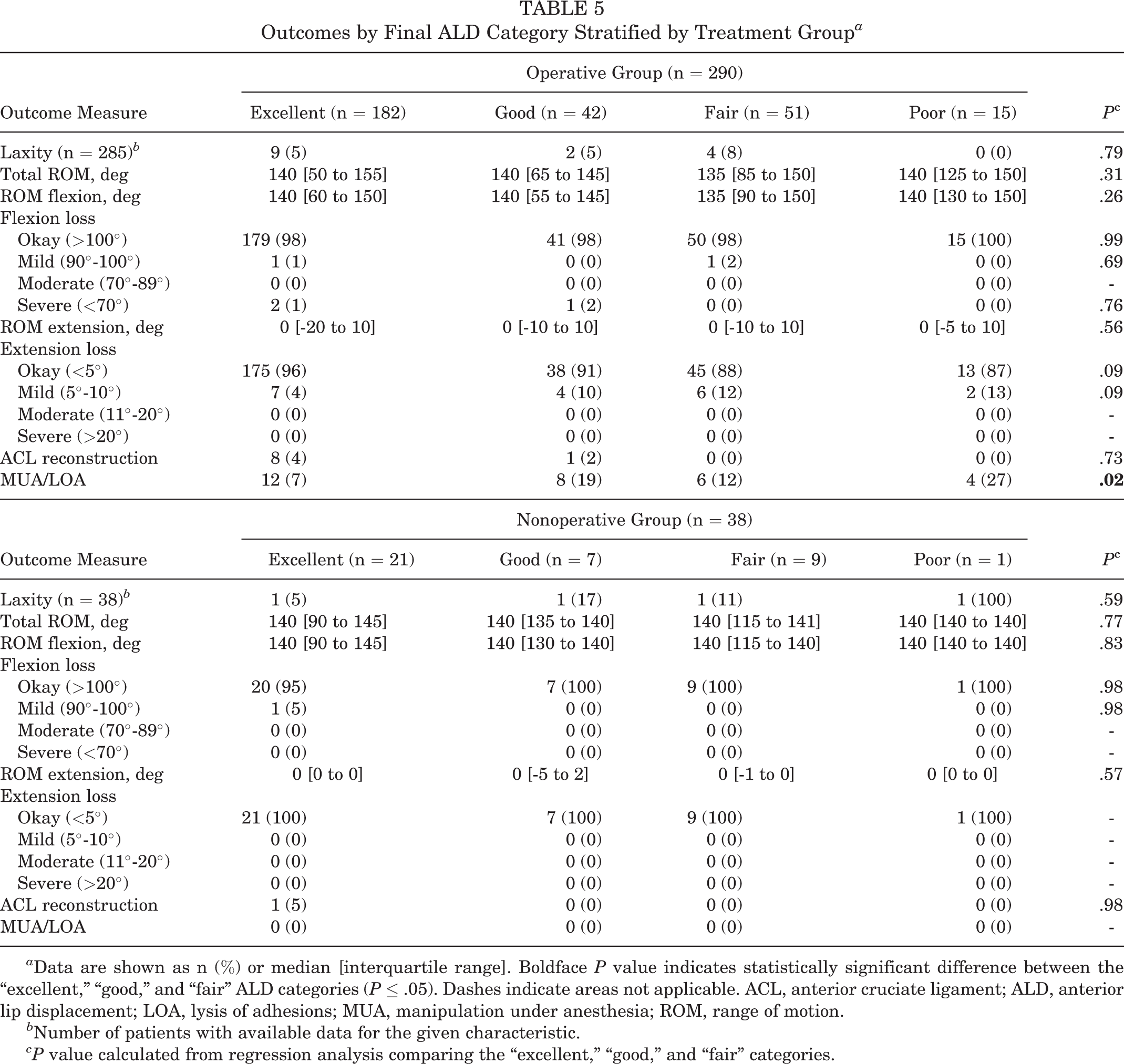
a Data are shown as n (%) or median [interquartile range]. Boldface P value indicates statistically significant difference between the “excellent,” “good,” and “fair” ALD categories (P ≤ .05). Dashes indicate areas not applicable. ACL, anterior cruciate ligament; ALD, anterior lip displacement; LOA, lysis of adhesions; MUA, manipulation under anesthesia; ROM, range of motion.
b Number of patients with available data for the given characteristic.
c P value calculated from regression analysis comparing the “excellent,” “good,” and “fair” categories.
Range of Motion
Total ROM arc before treatment was 80° and increased to 140° after treatment (P < .001) (Table 4). There were no significant associations detected between final ALD category and final ROM measurements.
We utilized a 2016 international consensus to classify arthrofibrosis of the knee into 1 of 4 categories for extension restriction (okay, <5°; mild, 5°-10°; moderate, 11°-20°; or severe, >20°) and flexion restriction (okay, >100°; mild, 90°-100°; moderate, 70°-89°; or severe <70°). 9 Within the operative cohort, there were no patients with moderate or severe extension loss, and the majority of patients were classified as “okay.” There was no difference in the proportion of patients with mild (5°-10°) extension loss between the ALD categories. This finding was also seen with flexion loss. In the operative group, there was an association between ALD category and secondary surgery for a manipulation under anesthesia (MUA) or lysis of adhesions (LOA) (P = .02) (Table 5).
In the nonoperative cohort, there were no patients with extension loss, and only 1 patient experienced flexion loss. In addition, there were no recordings of a secondary surgery for a MUA/LOA in the nonoperative group.
Complications
Eighteen percent of patients in the operative group had at least 1 complication, compared with 13% of patients in the nonoperative group (P = .50) (Table 3). For each 10° increase in final ROM, the odds of having a complication decreased by 52% (odds ratio = 0.48; 95% CI = 0.36-0.66; P < .001), controlling for surgery.
Discussion
This study is one of the largest comparative studies investigating residual anterior displacement of a tibial spine fracture in a geographically diverse, multicenter cohort of patients. In this study, strict anatomic reduction was not found to be absolutely mandatory to achieve subjective stability and near-normal ROM.
Two simultaneous events occur during a tibial spine fracture: elongation of the ACL through plastic deformation and the avulsion fracture itself. Screw and suture fixation utilize 2 different methods in addressing these simultaneous events. Screw fixation attempts to directly compress the bone fragments together, thereby indirectly tensioning the ACL. Suture fixation is performed through the base of the ACL fibers, tensioning the ACL and indirectly reducing and fixing the fracture fragment. While the goal of any fracture surgery is anatomic reduction of the displaced fragment, perfect reduction is not always achieved with either method, and tibial fracture fragment deformation may result from compression fixation. Rather, as a ligament avulsion fracture it is vital to restore the appropriate length-tension relationship of the ACL while ensuring no mechanical block to extension results. Residual anterior displacement of the tibial spine is believed to lead to limitations in the ROM of the knee, particularly with extension, and potential instability of the ACL.
A previous study seeking to compare suture versus screw fixation found that superior displacement of the anterior portion of the tibial spine fragment tended to be greater in patients who had repair with sutures. 6 This may be a consequence of a particular surgical technique in which suture fixation performed through the base of the ACL, which is located on the posterior portion of the fragment, may cause plastic deformation and superior elevation of the anterior-most portion of the fragment, which does not have any ACL fibers attached. In the current study, suture versus screw fixation had similar distributions in each category, yielding no difference in final radiographic result based on fixation strategy.
The classification of reduction was based upon the final measurement of the residual ALD. The operative cohort had 77% of patients with excellent-to-good reduction, 18% with fair reduction, and 5% with poor reduction. The nonoperative group had 74% excellent-to-good reduction, 24% fair reduction, and 3% poor. Most patients (84%) were classified as being in the fair or poor category before treatment, but 77% were classified in the excellent-to-good category after treatment. In a recent publication, 2 64% of a group of fellowship-trained surgeons recommended surgical treatment of tibial spine fracture with >3.5 mm of displacement. However, there is little consensus of what is acceptable after surgical treatment. Interestingly, 51/328 (16%) of patients within this cohort had a final measurement of >3.5 mm, even after receiving treatment.
Clinical laxity was defined as laxity on physical examination or subjective laxity experienced by the patient. Pretreatment, laxity was reported in 80% of all patients with data; after treatment, laxity was reported in 6% of patients. Overall, 5% of the operative cohort and 11% of the nonoperative cohort had clinical laxity; however, this difference was not statistically different. These data are lower in comparison with the range of instability in previous literature (14%-83%), but our data did not include any objective KT-1000 arthrometer measurements. 4,6,8,10 There was no difference in laxity in either cohort when stratifying for residual anterior displacement. In comparing the difference between the operatively treated and nonoperatively treated cohorts, this laxity may be reflective of the slightly higher degree of residual displacement in the nonoperative group compared with the operative group, but it is more likely indicative of modern surgical techniques designed to increase the tension of the ACL. Despite having more clinical laxity in the nonoperative group, there was no difference in ipsilateral ACL injury in either treatment group (1 vs 0); however, 9 patients in the operative group underwent delayed ACL reconstruction compared with 1 patient in the nonoperative group.
ROM of the knee and laxity directly relate to the overall function of the knee. The arc of motion preoperatively averaged 80° and increased to a median of 140° after treatment. Knee ROM from 10° to 115° is required for most activities of daily living, 12 and limitations in achieving these ranges can be detrimental and affect quality of life, especially in the young patient population. Overall, 7% of the study cohort (3% in the nonoperative group and 7% in the operative group) had arthrofibrosis. However, the final ALD category did not adversely contribute to extension loss, with only a marginal increase in developing extension loss if the reduction was not “excellent.” The common perception is that a residual anterior displacement of the tibial spine would prevent full extension, but this likely is dependent upon accommodation within the anterior aspect of the intercondylar notch and any medial or lateral translation. This study did not find any extension loss in the nonoperative group, even with fair to poor ALD. This may be a result of casting the knee in full extension or hyperextension while the fracture healed. 5,18 In addition, some patients who had a perfect reduction still experienced extension loss, which supports a multifactorial reason for arthrofibrosis. ALD was also not associated with flexion loss; 2 patients had to return to the operating room for treatment of arthrofibrosis.
Limitations
Although this was a large multicenter study of tibial spine fractures across varied geographically diverse, high-volume institutions, this study has a number of limitations, especially given the retrospective design. Data extended back to 2000, which affects the completeness of the injury recovery timeline for some patients and the lack of patient reported outcomes data (including activity level and return to activity rates, as well as long-term outcomes). Without complete data, some patients were excluded from the study cohort. In addition, due to the nature of this multicenter study, there may be some variation in interpreting radiology reports across institutions lending to a potential for diagnostic bias, although ALD measurement has been validated across these institutions. 7
In addition, the majority of patients were in the excellent-to-good category of ALD, and this increases the chance of a type II error with the smaller number of patients in the poor category. Specifically, a post hoc power analysis showed only 50% power in detecting extension loss differences in the operative group. However, this is biased by the quality of the reduction that is typically achieved. The nature of multicenter studies is that significant practice variation exists across numerous surgeons as does measurement of laxity (particularly without objective KT-1000 data) and ROM that could have influenced the reporting of these variables. In addition, this study did not specifically examine overreduction of the tibial spine (ie, negative displacement) but grouped them all into the “excellent” category to eliminate the risk of hiding an effect through averaging positive and negative values.
The standard-of-care clinical follow-up for these fractures extends to 9 to 12 months after initiation of treatment. We included patients with at least 3 months of clinical follow-up. Although these data skew the follow-up range values, we felt it was important to account for these ALD measures while assessing the sufficiency of the modern surgical technique for this cohort as a whole. While most patients had final radiographs that demonstrated complete healing, some patients with only postoperative radiographs were included. There is the possibility that some remodeling would have occurred that would place patients into a different category, but for those patients in whom there were serial radiographs, this phenomenon was not observed.
Conclusion
The findings of this study provide evidence that some residual displacement of the anterior lip may not negatively influence a patient’s posttreatment ROM, as has been previously thought, or affect residual laxity. Although the study results confirm that return to normal ROM and stability is possible without an ideal reduction of the anterior lip, we are not advocating for ignoring anatomic reduction. Rather, the study results suggest that persistent, repeated attempts at achieving intraoperative radiographic perfection may not be mandatory as long as knee stability and functional ROM are achieved.
Footnotes
Authors
Shannon A. McGurty, BS, Boston Children’s Hospital, Boston, Massachusetts, USA; Theodore J. Ganley, MD, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; Indranil Kushare, MD, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; Tomasina M. Leska, BS, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; Julian T. Aoyama, BA, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; Henry B. Ellis, MD, Texas Scottish Rite for Children, Dallas, Texas, USA; Ben Johnson, PA-C, Texas Scottish Rite for Children, Dallas, Texas, USA; Soroush Baghdadi, MD, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; Aristides I. Cruz Jr, MD, MBA, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA; Peter D. Fabricant, MD, MPH, Hospital for Special Surgery, New York, New York, USA; Daniel W. Green, MD, Hospital for Special Surgery, New York, New York, USA; R. Jay Lee, MD, Johns Hopkins University, Baltimore, Maryland, USA; Scott D. McKay, MD, Texas Children’s Hospital, The Woodlands, Texas, USA; Todd A. Milbrandt, MD, Mayo Clinic, Rochester, Minnesota, USA; Neeraj M. Patel, MD, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, Illinois, USA; Jason T. Rhodes, MD, Children’s Hospital of Colorado, Aurora, Colorado, USA; Brant Sachleben, MD, Arkansas Children’s Hospital, Little Rock, Arkansas, USA; Jessica L. Traver, MD, McGovern Medical School of the University of Texas Health Science Center, Houston, Texas, USA; R. Justin Mistovich, MD, MBA, University Hospitals Rainbow Babies and Children’s Hospital, Cleveland, Ohio, USA; Gregory A. Schmale, MD, Seattle Children’s, Seattle, Washington, USA; Danielle L. Cook, MA, Boston Children’s Hospital, Boston, Massachusetts, USA; Yi-Meng Yen, MD, PhD, Boston Children’s Hospital, Boston, Massachusetts, USA.
Final revision submitted March 21, 2023; accepted April 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.J.G. has received hospitality payments from Arthrex and is a paid associate editor for the American Journal of Sports Medicine. I.K. has received education payments from Medinc of Texas. H.B.E. has received education payments from Pylant Medical, consulting fees from WishBone Medical, and hospitality payments from Stryker. D.W.G. has received consulting fees from OrthoPediatrics, nonconsulting fees from Arthrex and Synthes, and royalties from Arthrex. R.J.L. has received education payments from Arthrex and hospitality payments from Vericel. S.D.M. has received education payments from Medinc of Texas. T.A.M. has received consulting fees from OrthoPediatrics, Medtronic, and Zimmer Biomet. N.M.P. has received education payments from Medwest and nonconsulting fees from Arthrex. B.S. has received education payments from Midsouth Orthopedics. R.J.M. has received consulting fees from OrthoPediatrics and Philips Electronics, nonconsulting fees from Philips Electronics, and hospitality payments from Globus Medical and Medical Device Business Services. G.A.S. has received education payments from Summit Surgical. Y.-M.Y. has received consulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Children’s Hospital of Philadelphia (No. 17-013853).