
Abstract
Background:
Few studies have examined the short-term clinical outcomes of rotator cuff repair (RCR) with all-suture anchors for medial row anchor fixation.
Purpose:
To evaluate clinical outcomes of double-row suture bridge RCR using a novel all-suture medial row anchor.
Study Design:
Case series; Level of evidence, 4.
Methods:
We enrolled 179 patients before double-row suture bridge RCR (mean age at surgery, 60.0 years; 63% male patients) at a single institution. All patients underwent RCR with all-suture anchor fixation for the medial row and solid anchor fixation for the lateral row. Preoperative (baseline) and follow-up (minimum follow-up time of 2 years; mean, 2.5 years) clinical outcomes were compared using the American Shoulder and Elbow Surgeons (ASES) score and a 10-point numeric pain rating scale (NPRS). We calculated the proportions of patients meeting previously published Patient Acceptable Symptom State (PASS) thresholds for the ASES (≥78.0) and NPRS (≤1.7). We further compared baseline and follow-up outcome scores and the proportions of patients meeting PASS thresholds using paired t tests and McNemar tests, respectively, and calculated effect size to quantify the magnitude of change from baseline to follow-up.
Results:
Values significantly improved from baseline to follow-up for ASES (from 45.3 ± 19.8 to 87.3 ± 17.1) and NPRS (from 5.2 ± 2.5 to 1.4 ± 2.1). The proportion of patients meeting PASS thresholds also significantly improved for the ASES (from 6% to 77%) and the NPRS (from 7% to 72%). The magnitude of baseline to follow-up change for all measures was large (all effect sizes ≥1.5).
Conclusion:
Our study demonstrated excellent short-term clinical outcomes and substantial improvements for patients undergoing double-row suture bridge RCR with all-suture anchors for medial row fixation.
Over the past 2 decades, rotator cuff repair (RCR) has advanced, especially with regard to arthroscopic instrumentation and suture anchor technology. Arthroscopic RCR is now performed routinely, demonstrating less pain, decreased deltoid dysfunction, and improved range of motion in early recovery when compared with mini-open RCR. 29 Suture anchor technology has advanced in the past 10 years to include the development of all-suture soft anchors. Advantages of all-suture anchors over conventional solid anchors are numerous. Principally, all-suture anchors are smaller in diameter than solid anchors, and less bone is displaced when drilling and setting these anchors, preserving bone stock. 6,18 This can prove especially useful in revision RCR, where bone stock has already been decreased by previous implants. Additional complications with conventional solid metal or biocomposite anchors may be avoided with all-suture anchors. These include anchor migration, synovitis, chondrolysis, reactive osteolysis, and chondral damage caused by third-body wear. 6,8,9,13 All-suture anchors have been shown to demonstrate less bone reaction and perianchor cyst formation when compared with polyetheretherketone anchors and bioabsorbable anchors, suggesting more reliable postoperative biologic fixation. 16,26 This is of particular clinical relevance, as rotator cuff retear rates have been demonstrated to correlate with bone reaction severity and perianchor cyst development. 26
Previous biomechanical studies have demonstrated similar or better mechanical performance of all-suture anchors when compared with conventional solid anchors during RCR. 1,2,10,18,22 A study comparing conventional solid anchors and all-suture anchors demonstrated no difference in 2-mm pullout but higher ultimate load to failure for the all-suture anchor. 22 Different manufacturers’ all-suture anchors also display similar biomechanical properties with regard to cyclic displacement, construct stiffness, and load to failure. 33 Application of an all-suture medial row in single and double-row RCR has also demonstrated similar mechanical performance and clinical efficacy in retrospective case series, with failure rates similar to those of conventional solid anchors. 2,7,20,34 For full-thickness RCR, we prefer a double-row suture bridge technique to optimize structural healing of the rotator cuff tendon, especially in large or massive tears. 23,31
In this study, we sought to evaluate our early experience using a novel all-suture medial row anchor in double-row suture bridge RCR. We hypothesized that an all-suture medial row construct would yield good outcomes without any untoward effects.
Methods
Patient Selection
The study protocol received institutional review board approval, and we followed STROBE guidelines in the development, conduct, and reporting of the research. 35 To identify potential participants, we conducted a retrospective billing code database search of RCR procedures from 2016 through 2018 at Andrews Sports Medicine and Orthopaedic Center performed by 1 of 4 fellowship-trained orthopaedic surgeons (E.L.C, J.R.D, B.A.E, and M.A.R). Patients were included in the study if they (1) underwent a primary, double-row, suture bridge RCR with all-suture medial row anchors; (2) were between the ages of 18 and 85 years at the time of surgery; (3) were enrolled in our ongoing data repository and had preoperative (baseline) patient-reported outcomes data; and (4) had at least 2 years of postoperative data. Patients were excluded if they: (1) did not undergo double-row RCR with all-suture medial row anchors (eg, solid anchors or single-row RCR) or (2) underwent revision RCR as an index procedure.
Surgical Technique and Postoperative Rehabilitation
Patients with full-thickness rotator cuff tears were identified and selected for surgery according to activity level, Goutallier grade of ≤3, and absence of degenerative glenohumeral changes on radiographs. All surgeries were performed in the lateral decubitus position, with the arm hung in 10 to 15 pounds (4-7 kg) of balanced suspension. Shoulders with associated acromioclavicular osteoarthritis were treated with concomitant arthroscopic distal clavicle excision. Shoulders with associated biceps tearing, superior labrum tearing, or significant tendinitis were treated with concomitant mini-open subpectoral biceps tenodesis.
Rotator cuff tears were debrided back to healthy tissue. The greater tuberosity insertion of the torn cuff was decorticated lightly with a shaver, as heavier decortication into trabecular bone has demonstrated decreased ultimate load to failure. 28 In the case of large or massive rotator cuff tears, the footprint was medialized slightly to within the margin of the articular cartilage. In the case of large L-shaped patterns, additional permanent No. 2 sutures were placed in side-to-side configuration to aid in accurate rotator cuff reduction. In the case of massive cuff U-shaped tears, a shoelace technique was employed to achieve side-to-side strain reduction by margin convergence. 3,17 For the medial row, 1 to 4 2.6-mm FiberTak all-suture anchors (Arthrex) double-loaded with 1.3-mm SutureTape were used (Arthrex), depending on tear width. These were drilled and anchored at the articular margin using an accessory lateral portal, attempting to be orthogonal to the bone surface for optimal insertion angle. 15 SutureTape limbs were passed in an interlocking/ripstop mattress or simple mattress pattern and knots tied. Alternating sutures were incorporated into a lateral row using 1 to 2 5.5-mm SwiveLock anchors (Arthrex).
Postoperative rehabilitation included physical therapy beginning on postoperative day 1 for range of motion, shoulder immobilization at rest for 6 weeks, and isometric strengthening beginning around the end of week 6.
Clinical Outcomes and Data Collection
To collect patient-reported function data, we enrolled patients who underwent RCR into an ongoing electronic data repository (OBERD; Universal Research Solutions) before their surgery and collected baseline (preoperative) surveys. The OBERD system then regularly distributed outcomes surveys electronically to enrolled patients using automated emails and/or text messages at 2 years after their RCR. Patients who did not respond to the electronic survey request were contacted via telephone and provided survey question responses orally. Before enrollment in our data repository, all patients provided either written, electronic informed consent (data repository data collection) or oral consent (telephone data collection).
Demographic and clinical data were obtained from chart and operative note reviews housed within our electronic health record. These data included age, sex, rotator cuff tear size, the number of medial row anchors utilized, the specific type of medial row anchor utilized, and whether the operative shoulder underwent revision surgery for retear at our institution. Rotator cuff tear sizes were categorized as small (<1 cm), medium (1-3 cm), large (3-5 cm), or massive (>5 cm). 5 Outcomes were reported with the American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment Form (scored from 0 to 100 [highest]), which evaluates limitations in shoulder-related function and includes subsections on pain, instability, and activities of daily living. 25 The ASES is valid, reliable, and responsive in measuring shoulder function for patients with rotator cuff pathology/RCR and has a minimal clinically important difference value of 6.4 points. 21 In addition, we extracted and used the numeric pain rating scale (NPRS) item for shoulder-related pain within the ASES to quantify pain (scored from 0 [best] to 10 [worst]).
Statistical Analyses
Summary statistics were calculated for baseline and follow-up demographic, clinical, surgical, and outcomes data. For ASES and NPRS scores at baseline and follow-up, we further calculated the proportions meeting previously reported Patient Acceptable Symptom State (PASS) cutoffs previously established for RCR (ASES, ≥78.0; NPRS, ≤1.7). 14 The baseline and follow-up ASES and NPRS scores were compared using the paired-samples t test, and the proportion of patients meeting the PASS thresholds for the ASES and NPRS were compared using the McNemar test. For all analyses, we considered timepoint differences (baseline to follow-up) statistically significant when P values were <.05. We further calculated effect sizes to quantify the magnitude of baseline to follow-up change in ASES/NPRS scores (Cohen d) and the proportion of patients meeting PASS thresholds for the ASES/NPRS (Cohen h).
Results
There were 196 RCR procedures that met the criteria for eligibility. Of these patients, 179 (91.3%) had baseline measurements and minimum 2-year follow-up data (Figure 1). Demographic and clinical data for the cohort are shown in Table 1. Both absolute scores and the proportions of patients meeting PASS thresholds significantly improved from baseline to follow-up for the ASES and the NPRS (all P < .01) (Table 2). The magnitude of baseline to follow-up change for all measures (absolute ASES and NPRS scores; meeting PASS thresholds) was large (Table 2).

Flowchart of patient inclusion. RCR, rotator cuff repair.
Demographic and Clinical Data (N = 179) a
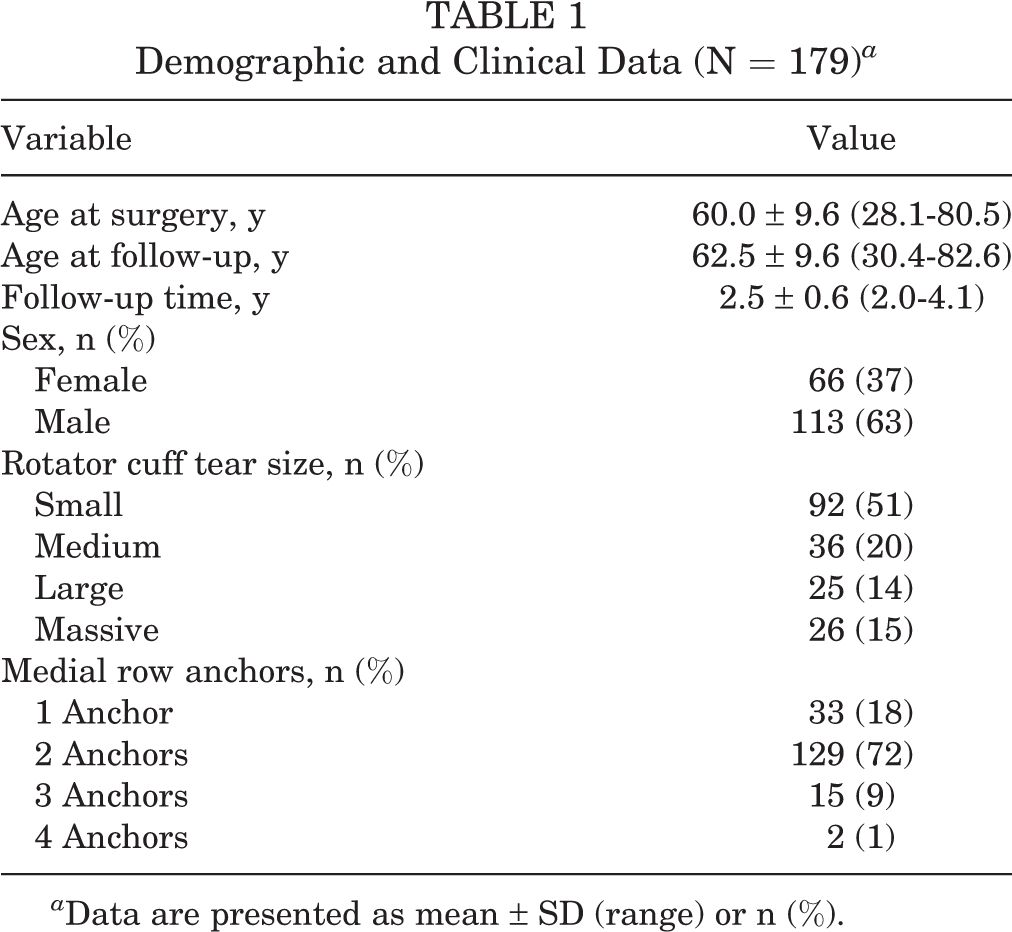
a Data are presented as mean ± SD (range) or n (%).
Baseline and Follow-up Patient-Reported Outcomes Data a

a ASES, American Shoulder and Elbow Surgeons Standardized Shoulder Assessment; NPRS, numeric pain rating scale; PASS, Patient Acceptable Symptom State.
b PASS values: ASES, ≥78.0; NPRS, ≤1.7.
No adverse reactions to the all-suture anchors were identified during routine postoperative follow-up. Only 2 of 196 patients (1.0%) underwent revision surgery at our institution for retear at the time of latest contact. Of these 2 failed repairs, 1 was a massive RCR that had an acute massive retear at approximately 20 months postoperative while performing manual labor and underwent revision RCR. The second failed repair was a large RCR that became a massive retear after a slip and fall at approximately 2 years postoperative and was subsequently converted to a reverse total shoulder arthroplasty. Both of these patients had failure at the musculotendinous junction, without anchor pullout.
Discussion
We found excellent clinical outcomes with RCR using a double-row suture bridge technique and a novel all-suture medial row anchor. Specifically, significant, clinically relevant improvements in ASES and NPRS scores were seen, and our same-institution revision RCR rate was low. To our knowledge, this is the first study to examine short-term clinical outcomes of RCR using this anchor and surgical approach.
Given that previous biomechanical studies demonstrated similar mechanical performance of all-suture anchors when compared with conventional solid anchors, 1,2,10,18,22 we expected similar or better findings with regard to clinical outcomes. Specifically, a cadaveric biomechanical study compared all-suture and conventional medial row anchors during double-row RCR and found no significant difference in cyclic creep, elongation, construct stiffness, failure mechanics, and maximum load (∼617 vs ∼545 N, respectively). 2 Previous 10-year clinical outcomes data from Johannsen et al 12 using conventional solid anchors in a double-row construct demonstrated a mean ASES score of 93.1. Tashjian et al 32 demonstrated a mean ASES score of 87.3 and excellent pain scores with a similar solid anchor double-row suture bridge technique. Studies of double-row solid anchors from Ji et al 11 and McCormick et al 19 reported similar mean ASES scores of 91.5 and 87, respectively; however, neither of these studies reported on complications specifically associated with solid anchors. For both of these studies, 11,19 the mean ASES score was within the minimal clinically important difference from our own series ASES score of 87.3, indicating a rate of success for the current study that was commensurate with other solid-anchor RCR data in the literature.
There are several potential advantages related to the use of all-suture anchors during RCR. Most notable is the smaller footprint inherent to an all-suture anchor. The anchors used in the current study had a drill diameter of 2.6 mm, which is considerably smaller than the typical 3.5- to 5.5-mm solid anchors offered by the same manufacturer. 30 In addition, all-suture anchors have been shown to have less bone reaction and perianchor cyst formation than polyetheretherketone or bioabsorbable implants. 26 Most all-suture anchors demonstrate minimal or zero cystic fluid around the anchor with magnetic resonance imaging follow-up 4,20,34 ; however, it is important to note that cysts can still occur if there is the presence of micromotion. 24 Micromotion may be present due to implant design or inadequate bunching of the anchor while tightening during anchor deployment. We recommend that, for knotted all-suture anchors, the anchor is pulled firmly by the surgeon to set it securely in bone and confirm adequate pull-out strength intraoperatively and minimize chance of intraoperative or postoperative failure of the anchor. This may prevent later subfailure cyclic displacement, anchor settling, anchor micromotion, anchor pull out, perianchor bone cyst formation, and, importantly, rotator cuff retear. 15,18,24,27
Finally, bone quality, which has been shown to correlate with subclinical anchor settling, 27 and cortical integrity could both affect construct stability and increase risk of anchor pull-out. In the event of intraoperative pull-out of an all-suture anchor during surgery on an osteopenic patient, we consider the use of conventional solid anchors as a backup. 7 In the current study, solid anchors were used for the lateral row as, to our knowledge, there is not yet an all-suture anchor construct available for this application. However, the aforementioned benefits of an all-suture medial row, namely the reduced anchor footprint and quality of cuff fixation at this location, support its use.
Limitations
There are a number of limitations to our study. Single-institution databases such as ours are vulnerable to bias and errors at the time of data entry. Similarly, there are inherent biases present in single-arm survey- and outcomes-based research, including the lack of a comparison group either not undergoing RCR or undergoing RCR with other medial row anchors. RCR surgeries were performed by experienced, high-volume surgeons, and our outcomes may not be generalizable to all clinical scenarios. We further understand that some of the improvement in ASES and NPRS scores may be attributable to concomitant procedures performed at the time of RCR, such as subacromial decompression or distal clavicle excision. However, because we did not collect these data routinely, we were unable to evaluate their potential effect on outcomes in this study.
In addition, we did not compare all-suture anchor outcomes with solid or other anchor outcomes, but plan to compare these groups in future work. It is also important to note that we did not record clinical RCR failures that did not undergo revision surgery, nor did we track revision surgeries outside of our center. However, we expect that, as a large referral center, revisions performed elsewhere were likely infrequent. We acknowledge that postoperative magnetic resonance imaging, which we do not obtain routinely in clinical follow-up, would have strengthened this study and elucidated the proportion of retears that did not require same-institution revision RCR. Lastly, as there is a paucity of biomechanical data on all-suture soft anchors, our specific double-row construct RCR has not been tested in a biomechanical study. Future studies should include biomechanical testing of all-suture soft anchor RCR, longer term follow-up of all-suture soft anchor RCR, and randomized trials comparing anchor types. We further recommend the evaluation of prevalence and incidence of complications and RCR failures/revisions with the use of an all-suture medial row.
Conclusion
Outcomes within our cohort of double-row suture bridge RCR with novel all-suture medial row anchors demonstrated significant improvements with clinical outcome scores comparable with previously published conventional solid anchor outcomes data. The clinical advantages of this approach include the preservation of bone stock and the reduction of anchor-related complications.
Footnotes
Final revision submitted April 10, 2023; accepted April 27, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded in part by support from Arthrex (Grant US-00697). The funding agency had no role in the collection, analysis, or interpretation of the data presented herein and no involvement in the writing of the manuscript or the decision to submit the manuscript for publication. J.J.F. has received education payments from Arthrex and Smith & Nephew. M.K.R. has received grant support from Arthrex; education payments from Arthrex, DJO, Fones Marketing Management, and Smith & Nephew; consulting fees and speaking fees from Arthrex and Zimmer Biomet; and hospitality payments from Linvatec and Prime Surgical. M.A.R. has received education payments from Arthrex, Smith & Nephew, and Zimmer Biomet and nonconsulting fees from Arthrex. B.A.E. has received consulting fees, nonconsulting fees, and royalties from Arthrex. J.R.D. has received consulting fees from Arthrex, Bioventus, DJO, Royal Biologics, and Smith & Nephew; nonconsulting fees from Arthrex; royalty from Arthrex and In2Bones. E.L.C. has received education payments from Prime Surgical and Zimmer Biomet; consulting fees from Arthrex, DJO, Smith & Nephew, and Zimmer Biomet; nonconsulting fees from Arthrex, Medical Device Business Services, and Smith & Nephew; royalties from Arthrex; and hospitality payments from Encore Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sterling IRB (no. 6280-ELCain).