
Abstract
Background:
Patella alta is a risk factor for recurrent patellar instability. Differences in chondral injury in patients with patellar instability between patella alta and patella norma have not been evaluated.
Purpose:
To analyze whether preoperative cartilage damage differs in severity and location between patellar instability patients with and without patella alta.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with patellar instability who underwent patellar realignment surgery at a single institution with preoperative magnetic resonance imaging (MRI) scans were included. After measurement of Caton-Deschamps index (CDI) on MRI, patients were divided into patella alta (CDI ≥1.3) and patella norma groups. The area measurement and depth and underlying structures (AMADEUS) score was used to quantify cartilage defect severity on MRI.
Results:
A total of 121 patients were divided into patella alta (n = 50) and patella norma (n = 71) groups. The groups did not differ significantly in sex ratio, age at MRI, body mass index, mean reported number of previous dislocations, or mean interval between first reported dislocation and date of MRI. A total of 34 (68%) of the patella alta group and 44 (62%) of the patella norma group had chondral defects (P = .625) with no significant between-group differences in defect size (P = .419). In both groups, chondral injuries most affected the medial patellar facet (55% in patella alta vs 52% in patella norma), followed by the lateral facet (25% vs 18%), and lateral femoral condyle (10% vs 14%). A smaller proportion of patients had full-thickness defects in the patella alta compared with the patella norma group (60% vs 82%; P = .030). The overall AMADEUS score was higher for the patella alta versus the patella norma group (68.9 vs 62.1; P = .023), indicating superior articular cartilage status.
Conclusion:
Patients with patella alta had less severe cartilage injury after patellar instability, including a lower proportion with full-thickness defects and better overall cartilage grade. The location of injury when present was similar between alta and norma, with most defects affecting the medial facet, lateral facet, and lateral femoral condyle in descending frequency.
Patellar instability is estimated to affect approximately 150 out of 100,000 adolescents between the ages of 14 and 18 years - a rate that is expected to increase over time. 14,16 Several risk factors have been associated with patellar instability, such as younger age, tibial tubercle-trochlear groove (TT-TG) distance, trochlear dysplasia, and patella alta. 3,6,9,21 Patella alta is defined as a superiorly positioned patella, commonly determined using the Caton-Deschamps index (CDI). 4 Patients with patella alta are approximately 2.5 to 4.0 times more likely to sustain a recurrent patellar dislocation, 9 which is thought to be due to the changes in biomechanics seen in patella alta. In these patients, the patella does not enter the trochlear groove until a greater degree of knee flexion. As such, there is greater reliance on the soft tissue restraints, including the medial patellofemoral ligament (MPFL) and medial quadriceps tendon femoral ligament. 2,19,24 Patella alta is also associated with further changes to patellofemoral joint (PFJ) biomechanics, such as increased length of soft tissue lateral restraints and changes in PFJ alignment. 22,24
Given these changes in biomechanics, it is possible that patella alta may alter cartilage injury patterns in patellofemoral instability. Stefanik et al 18 investigated cartilage damage patterns in patients with, or at risk of, osteoarthritis of the knee by analyzing magnetic resonance imaging (MRI) scans. They found that patients with patella alta and knee osteoarthritis were 3 times more likely to have lateral PFJ cartilage damage and 1.5 times more likely to have medial PFJ cartilage damage in comparison with those without patella alta. However, given this study was conducted in older patients (aged 50-79 years) that were at risk for or had knee osteoarthritis without previously documented patellar instability, these results cannot be extrapolated to our population of interest: young, active patients with patellar instability. This same group found in a follow-up study that patella alta was also associated with progression of cartilage damage and bone marrow lesions. 8
Mehl et al 13 found that trochlear dysplasia and patella alta contributed to the development of chondral defects when they compared those who had patellofemoral chondral defects and those who did not after anterior cruciate ligament injury. Ambra et al 1 found that trochlear dysplasia, lateral patellar tilt, and patella alta were associated more commonly with full-thickness patellofemoral chondral defects in their study. However, this study was conducted in 2 groups without a history of patellar instability. Articular damage has been found in as high as 76% of patients after acute patellar dislocation. 17,20 However, the effect of predisposing factors such as patella alta on cartilage damage severity and characterization has not been investigated.
The purpose of this study was to retrospectively analyze whether preoperative cartilage damage differs in severity and location between patellar instability patients with and without patella alta. We hypothesized that persons with patella alta, when controlling for the number of dislocations, will sustain a greater degrees of cartilage damage and that, when present, the location of defects would differ compared with persons with patella norma.
Methods
The current study was deemed exempt from institutional review board approval. A list of all patients who underwent patellar realignment surgery at our institution between January 1, 2014, and November 30, 2019, was obtained from the institution’s database. Patellar realignment surgery included MPFL reconstruction and/or tibial tubercle osteotomy as identified by the Current Procedural Terminology codes 27418, 27420, 27422, and 27427. Indications for patellar realignment surgery included first-time dislocation with loose body, osteochondral fracture, those who had failed nonoperative management, or history of recurrent dislocation. Patients were included if they had a proton-weighted MRI scan including sagittal, axial, and coronal views from within 3 months of injury on file and had a previous history of a patellar instability event. Patients were excluded if they underwent previous surgery to the ipsilateral knee, if they did not have a preoperative MRI, or if the preoperative MRI was undertaken more than 3 months before injury. In addition, 2 patients whose MRI scans were deemed to be of too poor quality to be accurately assessed by the readers, due to motion artifact, were excluded.
A total of 121 patients met the inclusion criteria (Figure 1). For all included patients, the sex, age at MRI scan, body mass index (BMI), date of earliest reported dislocation, and total number of reported dislocations were recorded from the electronic medical record.

Flowchart of patient inclusion. CPT, Current Procedural Terminology; MRI, magnetic resonance imaging.
MRI Analysis
Available preoperative 3-T or 1.5-T MRI examinations with adequate image quality and with standard MRI sequences including intermediate-weighted images, usually with fat saturation in at least 2 planes and a T1-weighted sequence in at least 1 plane (sagittal or coronal) were analyzed by 2 sports medicine clinical fellows (M.P.C. and M.R). Imaging parameters were used in accordance with Jungmann et al. 10 MRI scans were obtained in a standard fashion with the patients in the supine position, with the knee in an 8-channel knee coil, resulting in knee flexion of approximately 5°. To measure CDI on MRI, the technique described by Askenberger et al 3 was utilized. This technique determines CDI by using the sagittal slice showing the greatest length of the patella to determine patellar height (Figure 2). The readers individually selected the slice that they felt met this criterion best.
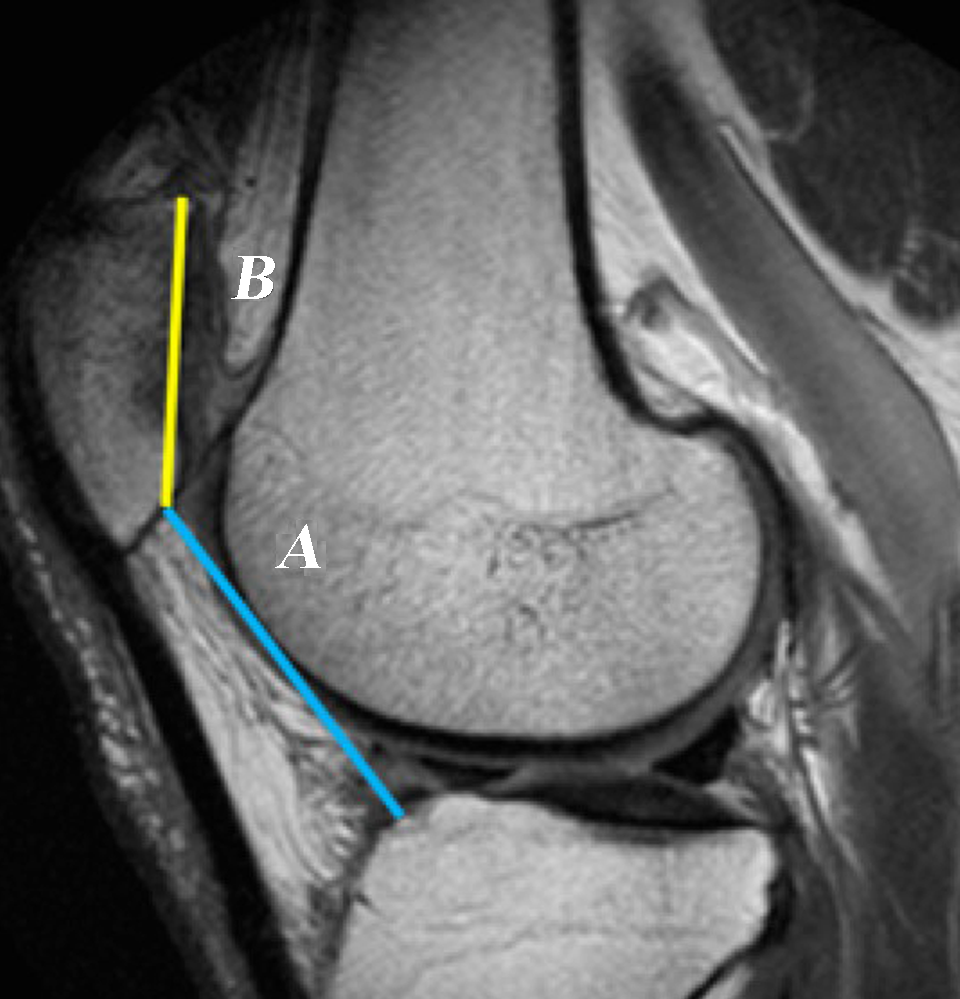
CDI measurement on a sagittal MRI image containing the greatest length of the patella. The CDI equals the distance from the distal aspect of the patellar articular cartilage to the anterosuperior corner of the tibial joint surface (A, blue line) divided by the length of the cartilaginous articular surface (B, yellow line). CDI, Caton-Deschamps index; MRI, magnetic resonance imaging.
The TT-TG distance was measured on axial images where the center of the tibial tubercle and trochlear groove were defined and the distance between the 2 was calculated. 5 In addition, patient images were assessed for trochlear dysplasia and characterized according to the Dejour classification. 11
To quantify cartilage defect severity, we used the MRI-based area measurement and depth and underlying structures (AMADEUS) score, first described by Jungmann et al. 10 The AMADEUS score characterizes cartilage defect size, defect depth, presence of subchondral bone defects, and bone marrow edema (BME). The scale is scored from 0 to 100, with 100 indicating no cartilage damage. In patients with multiple cartilage defects on MRI images, each defect was characterized and analyzed independently.
Statistical Analysis
Continuous variable data were reported as means with standard deviations and categorical data reported as frequencies with percentages. The distribution of data was assessed with the Shapiro-Wilk test. Continuous data were assessed with the Student’s t test and Mann-Whitney U tests as appropriate. Categorical data were assessed with chi-squared analysis. The threshold for significance was set to P < .05. Multivariate analysis was conducted with defect depth, bone edema, and AMADEUS score as the dependent variables. Interrater reliability was assessed by calculating intraclass correlation coefficients (ICCs) for continuous data and kappa agreement tests for categorical data. The ICC scores and kappa values were interpreted as follows: a score of 0 to 0.50 indicates weak reliability, a score of 0.51 to 0.70 indicates moderate reliability, and a score of 0.71 to 1.00 indicates a strong reliability. Interrater reliability was evaluated for CDI, each component of the AMADEUS classification, and total AMADEUS score. All statistical analyses were performed with R Studio (Version 3.6.3, RStudio: Integrated Development for R. RStudio, PBC, Boston, MA).
Results
The 121 study patients were divided into patella alta (n = 50) and patella norma (n = 71) groups based on a CDI cutoff of 1.3. The CDI measurements taken by each reviewer demonstrated strong interrater reliability (ICC = 0.76), so the mean of the CDI value obtained by each reviewer was utilized. The groups did not significantly differ in sex ratio, age at MRI, BMI, proportion of primary and recurrent dislocators, mean reported number of previous dislocations, or mean interval between first reported dislocation and date of MRI (Table 1). In addition, other baseline radiographic measurements including TT-TG and trochlear dysplasia did not differ significantly between groups.
Characteristics of Study Patients (N = 121) a
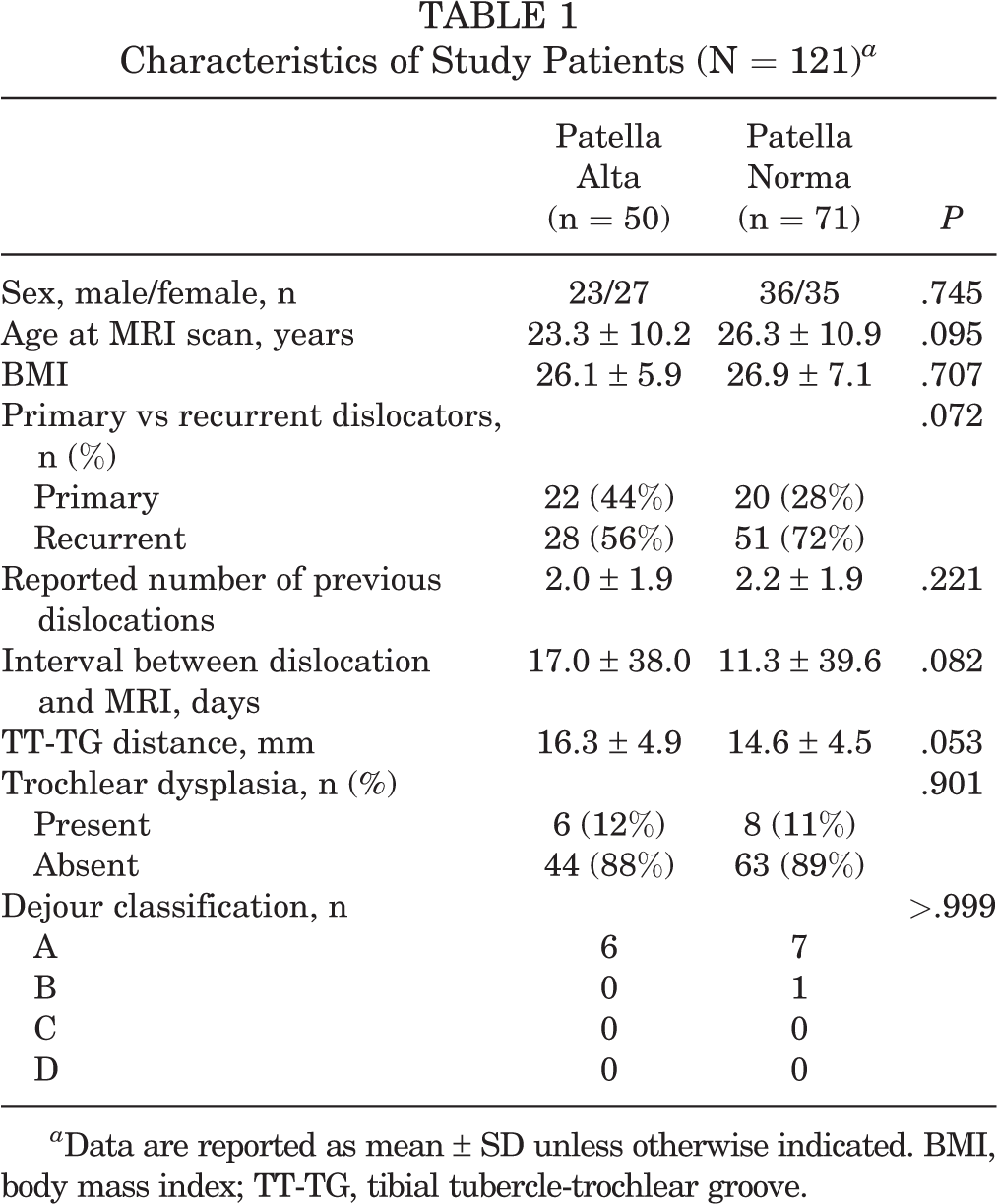
a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index; TT-TG, tibial tubercle-trochlear groove.
Upon analysis of MRIs for presence of chondral defect, 34 (68%) of the patella alta group and 44 (62%) of the patella norma group had chondral defects (P = .625). Defects identified on MRI images were further characterized via the AMADEUS classification system for a total of 40 lesions in 34 patients in the patella alta group and 56 lesions in 44 patients in the patella norma group. A total of 6 out of 34 patients (18%) in the patella alta group and 11 out of 44 patients (25%) in the patella norma group had multifocal chondral lesions (P = .435).
There were no significant differences between the groups in terms of defect size or characterization of subchondral bone defect. There were, however, differences in defect depth, BME, and total AMADEUS score (Table 2). The patella alta group had a smaller proportion of patients with full-thickness defects in comparison with the patella norma group (60% vs 82%; P = .030). In addition, a smaller proportion of patella alta patients had defect-associated BME (38% vs 59%; P = .048). The overall AMADEUS score for the patella alta group was higher (68.9 vs 62.1; P = .023) compared with the patella norma group. Data regarding defect size (ICC = 0.995), defect depth (κ = 0.853), subchondral bone defect (κ = 0.851), and bone edema (κ = 0.980) demonstrated strong agreement between the independent reviewers.
AMADEUS Chondral Defect Characterization a

a Given very strong agreement between reviewers, data from a single reviewer are shown. Data are reported as n (%) unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). AMADEUS, area measurement and depth and underlying structures; BME, bone marrow edema = like lesions.
There were no significant differences in the distribution of chondral defect locations between the 2 groups (Table 3).
Location of Chondral Defect a
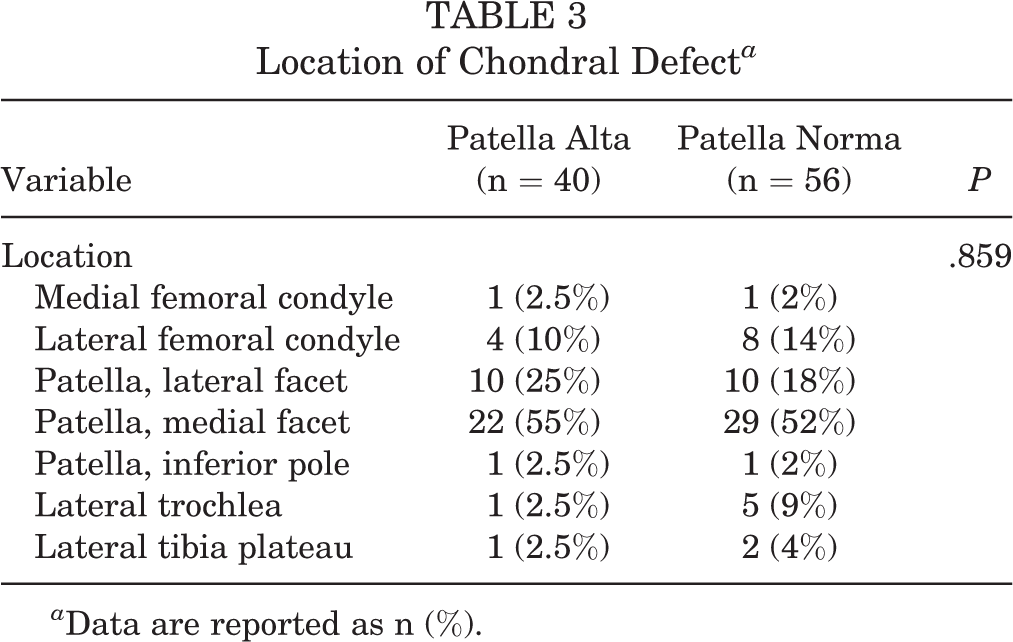
a Data are reported as n (%).
When looking at a multivariate regression using AMADEUS score as the dependent outcome, female sex showed an increase in AMADEUS score with a beta estimate of 11.96 (P < .001). Female sex also showed a higher probability of having no defect-associated BME (odds ratio = 6.7; P = .010) and a higher probability of partial-thickness defect rather than full-thickness (odds ratio = 3.9; P = .004). Age, BMI, interval between dislocation and MRI, and reported number of dislocations were not found to be associated with total AMADEUS score, probability of having defect-associated BME, or defect depth.
Discussion
Our hypothesis was rejected, as persons with patella alta had similar location of cartilage defects compared with persons with patella norma. This was in the setting of no significant difference in proportion of primary versus recurrent dislocators, TT-TG distance, or trochlear dysplasia between groups. Interestingly, there was a smaller proportion of patella alta patients with defect-associated BME-like lesions and the overall AMADEUS score for the patella alta group was higher compared with the patella norma group, indicating less severe defects in the patella alta group. Taken as a whole, these results indicate that patients with patella alta experience less severe cartilage damage after patellofemoral instability events, despite a similar frequency.
Persons with patella alta are at increased risk of patellar instability. Several factors have been identified that increase the risk of recurrent patellar instability, including younger age at initial dislocation, open physes, trochlear dysplasia, elevated TT-TG distance, and patella alta. 3 With patella alta, the patella articulates with the trochlear groove at greater flexion angle. 7,12,23 This anatomic difference increases risk of recurrent patellar instability with patella alta. The question of how this increased risk relates to chondral injury had not been answered.
In these preoperative cohorts, we found the groups to be demographically similar, and we found the number of dislocations before surgery to be statistically similar, averaging 2 previous dislocations, with a similar proportion of primary dislocators in each group. There was no statistically significant difference in the size of the chondral defects between the groups, with lesions most commonly being less than 1 cm2. In addition, chondral injuries were located mostly on the medial patellar facet (∼50%), followed by the lateral patellar facet, and lateral femoral condyle, in descending frequency. Interestingly, there was a higher likelihood of sustaining a full-thickness injury in the patella norma group, as compared with persons with patella alta. In addition, per the cartilage injury scoring system utilized, AMADEUS, patients with patella norma had a statistically significant more severe injury when evaluating lesion size, depth, and bony involvement in whole. While we found that those with patella alta had fewer full-thickness lesions and overall less severe cartilage damage as characterized by the AMADEUS scoring system, it is unclear whether this difference in severity of chondral injury has clinical significance. Runer et al 15 looked at AMADEUS scores in preoperative patients undergoing matrix-induced autologous chondrocyte implantation and correlated these scores with preoperative International Knee Documentation Committee, Lysholm, Short Form-12, and Core Outcome Measures Index (COMI) scores. They found a moderate correlation with COMI but no association with any of the other patient-reported outcome measures. Although the patient population in our current study differs from that of Runer et al, 15 it demonstrates the challenges with correlating cartilage injury with patient symptoms and function.
Cartilage injury after patellar dislocation has been evaluated previously. Zhang et al 26 studied 49 patients that underwent ultrasonography after acute lateral patellar dislocation. The rates of chondral and osteochondral injury to the inferomedial facet were approximately 35% and 25%. Our study found a higher rate of chondral injury to the medial facet, over 50%, which could be due to MRI having a higher sensitivity for identifying cartilage injury. In a follow-up study, Zhang et al 25 evaluated 121 consecutive adults with lateral patellar dislocation to identify the location of MPFL injury and lateral femoral condyle cartilage injury. MPFL injury occurred more commonly at the femoral insertion, with chondral and osteochondral injury rates of 4.2% and 6.3%, respectively. In patellar-sided MPFL injuries, there was a 19.4% and 22.2% rate of chondral and osteochondral injuries of the lateral femoral condyle, respectively. The incidence of lateral femoral condyle lesions in our study is similar to the findings of Zhang et al, 25 at 10% for the patella alta group and 14% for the patella norma group.
The effect of patella alta on cartilage injury has been studied previously in patients without a history of patellofemoral instability. Mehl et al 13 compared 43 patients with patellar cartilage defects with a cohort of patients with anterior cruciate ligament injury without patellofemoral chondral defects to determine whether there were anatomic features associated with risk of patellofemoral cartilage disease. They found that a flat and shallow trochlea, trochlea dysplasia, and patella alta contributed to the development of chondral defects. Ambra et al 1 compared a group of 135 patients undergoing cartilage restoration for patellofemoral chondral defects, without a history of instability, with a control group without chondral defects. They found trochlear dysplasia, patella alta, and lateral patellar tilt associated more commonly with full-thickness patellofemoral chondral defects. There does appear to be an association between patella alta and more severe patellofemoral disease in patients without a history of patellar instability.
With patella alta, there may be a component of ligamentous laxity that is protective in the setting of patellar instability. This would explain a lower proportion of our patients with full-thickness chondral defects in the patella alta group. Yanke et al 24 studied varying degrees of patella alta, and different attachment sites of the MPFL to the extensor mechanism, in 8 cadavers. They found that patella alta affects length changes of the proximal MPFC, especially with a CDI of over 1.6. It is possible that reduced soft tissue constraints dampen chondral injury in patients with patellar alta and instability. Further, patients with patella alta may have dislocation when the patella is less engaged in the trochlea, as a result of altered biomechanics. Thus, this may lead to less bone-to-bone and cartilage-to-cartilage shear forces occurring as well.
Limitations
There are limitations to this study. First, it is retrospective in nature. In addition, we did not have patient-reported outcomes to evaluate whether the differences in cartilage severity correlated with symptoms. Further, MRI image quality may have differed between patients, as they were not performed at the same facility and may have been performed with varying field strength and machine type. However, any MRI scan that did not meet criteria for analysis was excluded. This study included patients who underwent surgical intervention for patellar instability. It is unclear whether these results would hold true for patients who were successfully managed conservatively. Whereas we used regression analysis to look for confounding variables, the overall low mean number of previous dislocations may limit our ability to find significant association. Further study is warranted to determine the biomechanics of cartilage injury and patellar height as well as clinical implications of these differences in cartilage injury in pain, function, and treatment options for patients with patellar instability.
Conclusion
In this study, there was a high percentage of cartilage injury in patients with a history of patellar instability, with over 60% of patients showing cartilage damage on MRI images. Patients with normal patellar height had a higher frequency of full-thickness cartilage defects and more severe injury compared with those with patella alta. The location of cartilage injury between alta and norma was similar, with most defects affecting the medial facet, lateral facet, and lateral femoral condyle in descending frequency.
Footnotes
Final revision submitted March 8, 2023; accepted April 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.R. has received education payments from Liberty Surgical and Medical Device Business Services. B.J.E. has received research support from Arthrex, DePuy, Linvatec, Smith & Nephew, and Stryker and consulting fees from Arthrex. F.P.T. has received consulting fees from DePuy/Medical Device Business Services, has stock/stock options in Trice Medical, and has received hospitality payments from Smith & Nephew. K.B.F. has received consulting fees from DePuy and Vericel. M.E.B. has received education payments from Gotham Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (study 19E.938).