
Abstract
Background:
Satisfaction with social roles and activities is an important outcome for postsurgical rehabilitation and quality of life but not commonly assessed.
Purpose:
To evaluate longitudinal patterns of the Patient-Reported Outcomes Measurement Information System (PROMIS) Satisfaction with Social Roles and Activities measure, including how it relates to other biopsychosocial factors, before and up to 6 months after sports-related orthopaedic surgery.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Participants (N = 223) who underwent knee and shoulder sports orthopaedic surgeries between August 2016 and October 2020 completed PROMIS computer-adaptive testing item banks and pain-related measures before surgery and at 6-week, 3-month, and 6-month follow-ups. In a generalized additive mixed model, covariates included time point; peripheral nerve block; the PROMIS Anxiety, Sleep Disturbance, and Pain Behavior measures; and previous 24-hour pain intensity. Patient-reported outcomes were modeled as nonlinear (smoothed) effects.
Results:
The linear (estimate, 2.06; 95% CI, 0.77-3.35; P = .002) and quadratic (estimate, 2.93; 95% CI, 1.78-4.08; P < .001) effects of time, as well the nonlinear effects of PROMIS Anxiety (P < .001), PROMIS Sleep Disturbance (P < .001), PROMIS Pain Behavior (P < .001), and pain intensity (P = .02), were significantly associated with PROMIS Satisfaction with Social Roles and Activities. The cubic effect of time (P = .06) and peripheral nerve block (P = .28) were not. The proportion of patients with a 0.5-SD improvement in the primary outcome increased from 23% at 6 weeks to 52% by 6 months postsurgery, whereas those reporting worsening PROMIS Satisfaction with Social Roles and Activities decreased from 30% at 6 weeks to 13% at 6 months.
Conclusion:
The PROMIS Satisfaction with Social Roles and Activities measure was found to be related to additional domains of function (eg, mental health, behavioral, pain) associated with postsurgical rehabilitation.
Inadequate and incomplete return to sport and work after orthopaedic sports surgery is not uncommon. For example, 60% of patients who underwent surgical intervention for multiligamentous knee surgery were able to return to any level of sport after a median 6-month recovery time, with about 25% returning to high-level activity, 13 whereas 85% of patients who underwent procedures such as Lisfranc repair and shoulder arthroplasty returned to sport. 4,34 In addition to variation by impacted joint and surgery, variability in postsurgical functional restoration may be attributed to occupational physical demand 1,2 or sports participation. 39 Therefore, to optimize postsurgical rehabilitation for patients undergoing a variety of surgeries with a range of physical restoration needs, identifying and monitoring multifaceted aspects of functioning could allow for targeted and timely interventions and clinical decisions (eg, increase therapy frequency, decrease medication dose).
Although legacy measures of orthopaedic surgery recovery have often included self-reported (eg, physical function and return to work/sport) and objective (eg, physical performance) outcomes, few studies have examined patients’ satisfaction with their social role functioning and activities. Satisfaction with social roles and activities refers to patients’ satisfaction with their ability to engage in work, social activities (eg, time with family and friends), and daily activities (eg, chores, errands, hobbies), as well as satisfaction with the quality of and time spent in their social roles. 20,21 Previous evidence indicates that greater mental and physical health morbidity are associated with lower social role satisfaction, 5 whereas higher reported resilience is associated with higher social role satisfaction. 6 Although evidence indicating satisfaction with social roles and activities is an important outcome to patients and could aid providers in responsive rehabilitation planning, 17 this outcome remains underexplored in patients undergoing sports orthopaedic surgery. Moreover, as providers move to value-based care, it is important to assess outcomes that are important to patients and identify distinct modifiable factors that could be modulated to improve postsurgical rehabilitation and functional restoration.
Variability in postsurgical recovery may be explained, in part, by several biopsychosocial factors (eg, sleep, mood, pain), which can be present both before and in the weeks to months after surgery. For example, presurgical sleep disturbances are associated with greater presurgical and postsurgical opioid use, poor postsurgical acute pain control, and reduced recovery. 35,61 In addition, elevated presurgical mental health and physical health symptoms are associated with poor postsurgical acute pain control in a meta-analysis of heterogeneous patient samples, 60 as well as a lower likelihood of return to work in patients undergoing arthroscopic rotator cuff repair. 16 With a large body of evidence and a shift toward value-based care, providers may benefit from assessing and addressing biopsychosocial factors associated with postsurgical outcomes but must balance the risk of patient assessment burden and time constraints placed on staff working in high-volume clinics.
The goals of the present study were twofold. First, using the Patient-Reported Outcome Measurement Information System (PROMIS), 42 we sought to determine which set of patient-reported outcomes accounted for the greatest variance in the PROMIS T-scores for the Satisfaction with Social Roles and Activities measure from presurgery through 6-month follow-up. Once the optimal set of predictors was identified, our second goal was to examine the relationship between predictors and outcome using a robust analytic approach. We hypothesized that the PROMIS Anxiety, Depression, Sleep Disturbance, and Pain Behavior measures as well as pain intensity would be uniquely associated with the PROMIS Satisfaction with Social Roles and Activities measure, such that elevated symptoms would be associated with lower Satisfaction with Social Roles and Activities T-scores across all time points.
Methods
Participants and Procedures
Data were collected as part of 2 prospective longitudinal observational studies that were combined under a single protocol and approved by our institutional review board. Adult (aged ≥18 years) active-duty US servicemembers undergoing shoulder or knee orthopaedic sports procedures were included in the present analysis. Recruitment occurred from August 2016 to October 2020. Patients were not eligible to participate if they were unable to understand and complete study consent and procedures. After providing written informed consent and Health Insurance Portability and Accountability Act (HIPAA) authorization, enrolled participants were emailed links to complete online surveys before surgery and again at 6 weeks, 3 months, and 6 months after surgery. The data of participants who completed at least 2 assessments were included in the analyses.
Variables of Interest
The PROMIS computer-adaptive testing (CAT) item banks included Satisfaction with Social Roles and Activities, Anxiety, Depression, Sleep Disturbance, and Pain Behavior. 10,20,45,48,53 Timestamps corresponding to the completion of each PROMIS CAT item bank were also available, although the timestamp was at the minute (not second) level and participants could pause (or stop) responding, resulting in a long duration. On average across time points, most participants completed the Satisfaction with Social Roles and Activities (72%), Anxiety (94%), Depression (91%), Sleep Disturbance (87%), and Pain Behavior (74%) CAT item banks in ≤2 minutes.
The PROMIS CAT item banks yield a T-score (mean ± SD, 50 ± 10; range, 0-100) normed on a general US population. These scores are calibrated using item response theory 9 and validated rigorously, to include content validity (eg, established via extensive patient interviews and expert review panels), cross-sectional validity (eg, concurrent validity between individuals with and without comorbidities and disabilities), responsiveness to change, and clinical validity (eg, evaluation of multiple domains across a variety of clinical contexts). With CAT, each question is determined by the response to the prior question. The measure terminates when the standard error of responses reaches a prespecified level, indicating reliable responses. If the standard error level is not obtained, then the scale terminates after the maximum allowed questions. Across multiple orthopaedic studies, PROMIS CAT item banks terminate after 4 to 5 questions, on average. 7,18,22,52
Further information on CAT, item banks and short forms in English and many other languages, and publications that cite PROMIS measures are publicly available online. 42 To further aid clinical interpretability and utilization, ProsettaStone.com provides calibrated linking tables that “link” legacy measure scores (eg, Short Form-36; Oswestry Disability Index, Knee and Hip Disability and Osteoarthritis Outcome Score–Physical Function Short Form; Quick Disabilities of Arm, Shoulder and Hand; Roland-Morris Disability Questionnaire) that are statistically similar to PROMIS scores (eg, PROMIS Physical Function). 25,26,51,55 Previous evidence indicates that the minimal clinically important difference (MCID) of various PROMIS item banks and short form scales varies by clinical population, PROMIS item bank, method of MCID calculation, and assessment timing (eg, change from lowest function, such as acutely after fracture to follow-up). 15,23,24,28,31,43,50,61 Therefore, analyses also described the number and proportion of participants reporting a 5-point change in each PROMIS item bank, which is indicative of half a standard deviation of change and a conservative estimation of MCID.
The Defense and Veterans Pain Rating Scale 46 was used to assess average pain over the previous 24 hours within the context of functioning (range, 0-10). Additional potential covariates included time point, as well as data collected from health records: surgery type, study, age, body mass index, administration of a peripheral nerve block at the time of surgery and location of the block, history of sleep apnea, and smoking or tobacco use (yes/no). Sleep apnea was included because of its potential relationship with PROMIS Sleep.
Analytic Plan
Analyses were conducted in 3 steps. First, univariate and bivariate analyses described the overall sample, as well as differences by surgical groups. The compareGroups R package 54 was used to construct a descriptive table. Bivariate tests also examined the relationships between patient-reported outcomes (PROMIS Anxiety, Depression, Sleep Disturbance, Pain Interference, Pain Behavior, and average pain in the previous 24 hours), patient characteristics, and care-related factors with presurgical PROMIS Satisfaction with Social Roles and Activities.
Second, analyses identified the best-fitting set of covariates for inclusion in a generalized additive mixed model (GAMM) evaluating PROMIS Satisfaction with Social Roles and Activities. This step was conducted using the buildmer R package, 56 in which all factors significantly associated with presurgical PROMIS Satisfaction with Social Roles and Activities and each patient-reported outcome × time point interaction term were considered for inclusion as covariates. The interaction terms were included to determine whether the relationship (slope) between a patient-reported outcome and PROMIS Satisfaction with Social Roles and Activities varied from before surgery to 6-month follow-up.
Third, the best-fitting set of covariates was then examined in a final GAMM using the gamm4 R package. 59 The GAMM, a type of regression, was selected for its ability to model relationships between nonnormally distributed predictors and outcomes, nonnormally distributed relationships, and the random effect for each participant. To ensure adequate uniqueness of each predictor, multicollinearity was evaluated using the performance R package, 37 which computed the variance inflation factor of each covariate. A variance inflation factor <5 indicates the correlation between covariates is low and therefore acceptable. The sjPlot R package 38 provided the GAMM results in a presentable table. Estimated conditional means of covariates were extracted with the ggeffects R package, 36 then plotted using the ggplot2 57 and ggpubr 29 R packages. Proportions of participants reporting at least a 5-point change in PROMIS CAT item banks (eg, half a standard deviation change in scores) significantly associated with the outcome were visualized using the ggalt R package. 49 Statistical significance was indicated by P < .05.
Results
Univariate and Bivariate Statistics
Participant characteristics for the analyzed sample (N = 223) are shown in Table 1. Most participants were White (67%) and assigned male (81%), with a median age of 39 years (range, 18-74 years; IQR, 30-49 years). Of the 130 (58%) participants who underwent shoulder surgery, most underwent arthroscopic procedures (67%) in a beach-chair position (82%) and received a brachial plexus interscalene peripheral nerve block (78%). However, 20 (15%) participants received a block, but the block location was not documented in the medical record. Participants could undergo ≥1 shoulder procedures, which included biceps tenodesis and distal clavicle resection (49%), labrum repair (48%), and/or rotator cuff repair (43%). Participants undergoing knee surgery (n = 93, 42%) could also receive ≥1 procedures, including a meniscus procedure (59%; 47% debridement and 12% repair), acute cruciate ligament reconstruction (41%; 26% allograft and 15% autograft), and cartilage procedures (24%; 20% chondroplasty and 4% osteochondral autograft transfer system or autologous chondrocyte implantation). Most patients who underwent a knee surgery received at least 1 (58%) or 2 (9%) peripheral nerve blocks, the most common being adductor canal (59%), followed by sciatic (9%) and femoral (8%) nerve blocks.
Sample Characteristics Overall and by Surgery Group Before Surgery a

a Data are reported as median [IQR] or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). PROMIS, Patient-Reported Outcomes Measurement Information System.
b Due to low sample size (eg, cell size < 5), these race and ethnicity categories were combined in this table.
c As assigned in medical record.
Survey completion rates decreased across time points (presurgical = 309, 58% shoulder; week 6 = 260, 57% shoulder; month 3 = 194, 61% shoulder; month 6 = 191, 62% shoulder). Of the 309 participants who completed at least 1 assessment, 223 completed assessments at ≥2 time points and were included in subsequent analyses. Bivariate analyses indicated that participants who completed only 1 time point (n = 86) did not significantly vary from those who completed more than 1 time point across several factors, including previous 24-hour average pain, PROMIS Pain Behavior, PROMIS Pain Interference, PROMIS Sleep Disturbance, PROMIS Satisfaction with Social Roles and Activities, age, body mass index, surgery type, and race and ethnicity (all P > .05). However, participants included in the analyses, relative to those who were not, had lower median PROMIS Anxiety (49.2 [IQR, 40.9-54.1] vs 50.0 [IQR, 50.0-54.0], respectively) and Depression (44.9 [IQR, 34.2-51.0] vs 50.0 [IQR, 50.0-54.0], respectively) T-scores.
Covariate Selection
Next, the algorithmic approach to covariate selection indicated the best-fitting GAMM accounted for 42% of the variance in PROMIS Satisfaction with Social Roles and Activities. Model covariates included time point (linear, quadratic, and cubic terms), peripheral nerve block, PROMIS Anxiety, PROMIS Sleep Disturbance, PROMIS Pain Behavior, and pain intensity in the previous 24 hours. None of the patient-reported outcome × time point interaction terms were included in the best-fitting GAMM.
Outcome Model
Identified covariates were included in a GAMM predicting Satisfaction with Social Roles and Activities, with results reported in Table 2. In the GAMM, all covariates were significantly associated with PROMIS Satisfaction with Social Roles and Activities, aside from the cubic time term and peripheral nerve block. Smoothed (nonlinear) covariates are depicted in Figure 1.
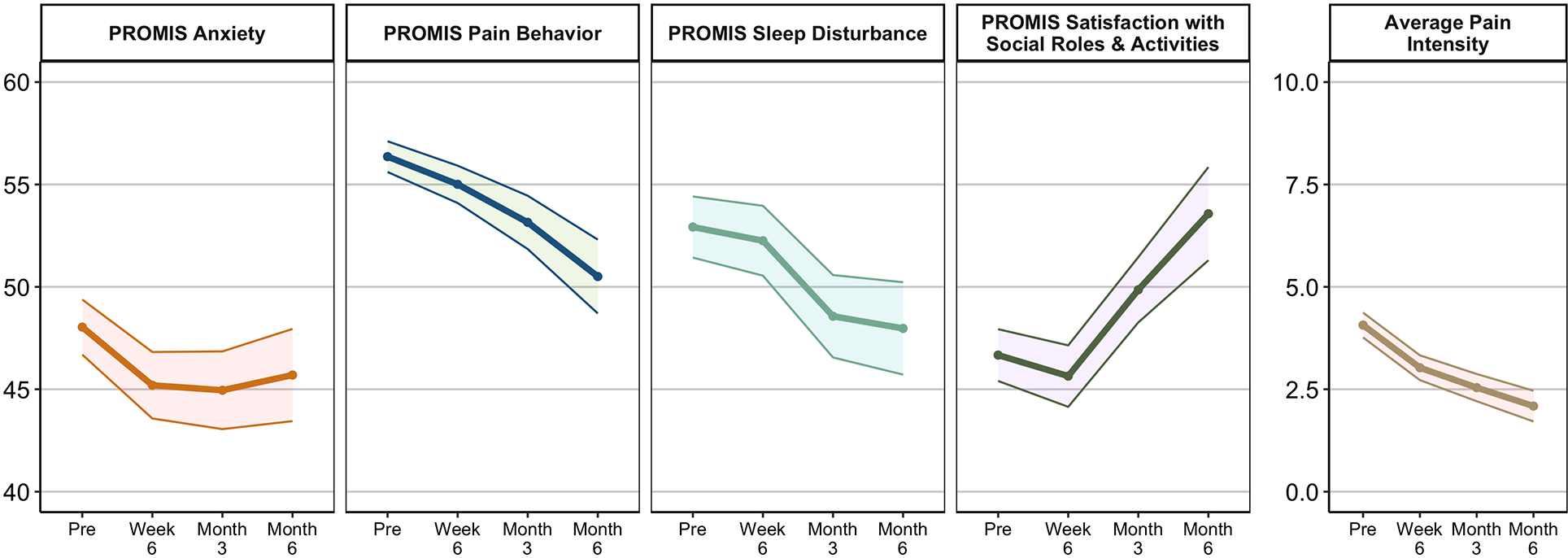
Mean patient-reported outcomes across time points. Shaded areas indicate 95% CIs. PROMIS, Patient-Reported Outcomes Measurement Information System.
Results From the Generalized Additive Mixed Model Predicting PROMIS Satisfaction With Social Roles and Activities From Presurgery to 6 Months Postsurgery a
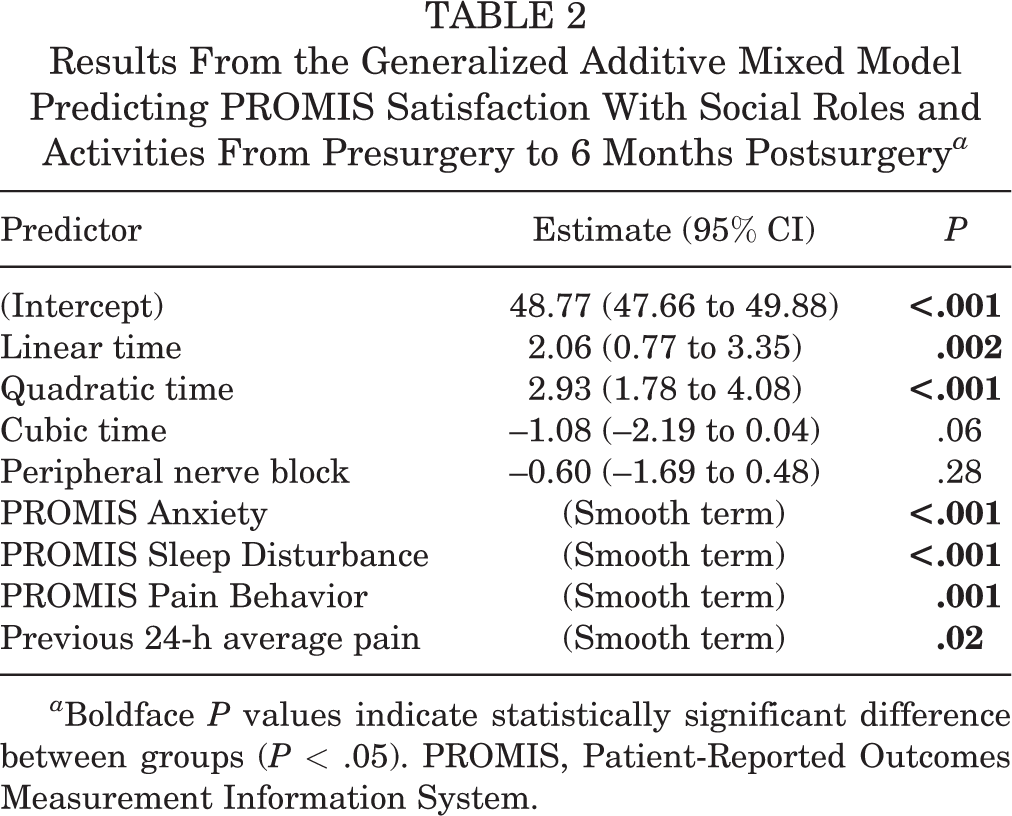
a Boldface P values indicate statistically significant difference between groups (P < .05). PROMIS, Patient-Reported Outcomes Measurement Information System.
For descriptive purposes, the proportion of participants reporting at least a 5-point change in PROMIS item banks between presurgery and each follow-up is reported in Figure 2. For example, while 30% of participants reported worsening PROMIS Satisfaction with Social Roles and Activities scores at 6 weeks postoperatively, the highest proportion of any PROMIS item bank captured in this study, more than half reported clinically meaningful improvements in social satisfaction by 6 months. To further aid in changes from the presurgical time point, the frequencies and percentages of participants who had reported improvements, reductions, or stagnancy in patient-reported outcomes at each time point, relative to their presurgical report, are available separately in Supplemental Table S1 (participants stratified by presurgical symptom levels; eg, elevated vs not elevated).

Proportion of participants reporting worsening (shown in red) and improving (shown in green) PROMIS Anxiety, Sleep Disturbance, Pain Behavior, and Satisfaction with Social Roles and Activities scores, as indicated by a 5-point change from presurgery to each follow-up time point. PROMIS, Patient-Reported Outcomes Measurement Information System.
Discussion
In the present study, 3 PROMIS CAT item banks (Anxiety, Sleep Disturbance, Pain Behavior) and previous 24-hour pain intensity were associated with PROMIS Satisfaction with Social Roles and Activities from presurgery through 6-month follow-up, whereas patient characteristics, surgery type, and patient-reported outcome × time point interactions did not provide meaningful contributions to the model. Taken together, modifiable patient experiences, such as those related to anxiety, sleep, and pain, may change in step with or result in changes to social functioning in patients undergoing orthopaedic surgeries. Given the contributions of social functioning to overall quality of life, physical and mental health, and patient satisfaction but lack of routine assessment, 19,32 the present findings suggest that the incorporation of multidimensional patient-reported outcomes, to include Satisfaction with Social Roles and Activities, could be important to both patient-centered research and health care improvement. 3
An individual’s feeling of social connectedness is associated with decreased risk for all-cause mortality, improved biopsychosocial functioning, and overall quality of life. 6,14,27 To date, much of the research understanding patient-reported factors that contribute to changes in PROMIS Satisfaction with Social Roles and Activities has been conducted in samples of individuals living with physical disabilities, cancer, or chronic pain. 6,11,14,30,32 Uniquely, this study examined changes in PROMIS Satisfaction with Social Roles and Activities throughout postsurgical recovery and rehabilitation in individuals undergoing high-volume orthopaedic surgeries who are routinely seen in clinical practice. In particular, the present study also found that the proportion of participants reporting clinically meaningful improvements increased across time, with approximately half of the sample surpassing the prespecified and conservative MCID threshold (+5 points). Including PROMIS Satisfaction with Social Roles and Activities in routine clinical care may be an additional means of evaluating progress toward functional goals at postsurgical visits (eg, 3-month, 6-month, and 12-month follow-ups) or identifying areas of regression for patients who develop persistent postsurgical pain and functional limitations that negatively affect their social functioning.
Research regarding the validity and predictive capabilities of PROMIS measures within orthopaedic care settings has expanded over the past several years, 58 with some evidence demonstrating their utility in shared decision-making regarding postsurgical opioid prescribing 8 and value dashboards for orthopaedic surgeons. 47 Treatment pathways informed by multidimensional PROMIS responses, to include Satisfaction with Social Roles and Activities, have also shown some potential to stratify patients by multidimensional symptom severity. 33 Such stratification tools could inform treatment pathways, identify specific interventions, and monitor treatment response. For example, a study in an oncological care setting found that purposeful PROMIS screening via the patient portal and programmed physician and behavioral health provider alerts in the electronic health record could be used to enhance more tailored, patient-centered care. 44 Given the potential impact of psychological and social functioning on pain and patient satisfaction, 40 future patient-engaged research 12,41 is needed to identify whether PROMIS Satisfaction with Social Roles and Activities should and could be meaningfully incorporated into clinical care pathway algorithms and decision support tools.
Limitations
Study limitations were present and provided impetus for future research. Causality cannot be established due to the observational study design. Although a large proportion of the outcome variance was accounted for in the GAMM, many factors not assessed in the present study may be associated with postsurgical outcomes (eg, pain catastrophizing, duration of symptoms before surgery, return to duty). As such, it is unclear the extent to which some participants experienced worsening symptoms at later time periods due to returning to duty or other impacting factors outside of the postsurgical sequelae. This limitation highlights the importance of multidimensional assessment as a means of contextualizing the patient’s experience to include extenuating and environmental factors. This study did not seek to differentiate between different surgical sites, procedures, and approaches, but instead, the random effect of each participant was included to account for the correlated longitudinal assessments. Therefore, studies comparing surgical populations and procedural approaches or techniques, as well as nuances of patient experiences by surgical site, may benefit from a multidimensional assessment approach. In addition, the selection of the MCID threshold may limit interpretability, as the MCID varies across surgical populations and assessment timing.
The present study had several limitations to generalizability. The active-duty servicemembers undergoing shoulder and knee sports orthopaedic surgery at a single facility and the procedures and approaches included in this sample may not be representative of other orthopaedic surgery samples. While the data had limited information on other medical conditions (eg, sleep apnea), the active-duty sample may not generalize to nonmilitary samples. Those included in the study had worse PROMIS Depression and Anxiety T-scores relative to enrolled participants who did not complete at least 2 assessments, and less than half of participants completed the 6-month follow-up. While the analytic approach used all available data (eg, participant data were retained for all completed time points, even if missing at any other time point), analyses cannot completely address the decreasing response rates across time points. As such, the generalizability is limited, and study results require replication and extension given lower response rates. Despite these limitations, the longitudinal study design, incorporation of GAMM, and utilization of PROMIS measures currently used in clinical practice settings provide support for the utility of measuring and assessing changes in social satisfaction throughout postsurgical recovery to inform the timely delivery of interdisciplinary care team-based interventions.
Conclusion
In this study, changes in anxiety, sleep disturbance, pain behavior, and previous 24-hour pain intensity contributed to satisfaction with social roles up to 6 months after orthopaedic surgery. These findings underscore the potential value of multifaceted patient-reported outcome assessed during postsurgical rehabilitation to inform timely implementation of targeted, interdisciplinary interventions, including those that enhance social function.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231184834#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231184834 - Longitudinal Predictors of PROMIS Satisfaction With Social Roles and Activities After Shoulder and Knee Sports Orthopaedic Surgery in United States Military Servicemembers: An Observational Study
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231184834 for Longitudinal Predictors of PROMIS Satisfaction With Social Roles and Activities After Shoulder and Knee Sports Orthopaedic Surgery in United States Military Servicemembers: An Observational Study by Krista B. Highland, Michael Kent, Nicholas McNiffe, Jeanne C. Patzkowski, Michael S. Patzkowski, Alexandra Kane and Nicholas A. Giordano in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted March 10, 2023; accepted April 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The institution of multiple authors (K.B.H., A.K.) received funding for this Collaborative Health Initiative Research Program (CHIRP) project by the Uniformed Services University through the Henry M. Jackson Foundation for the Advancement of Military Medicine Inc on agreement (CHIRP-91-8843-01). J.C.P. has received education support from Medinc of Texas. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Walter Reed National Military Medical Center (ref No. WRNMMC-2018-0132).
The views expressed are solely those of the authors and do not reflect the official policy or position of the Uniformed Services University, US Army, US Navy, US Air Force, the Department of Defense, the US Government, or the Henry M. Jackson Foundation for the Advancement of Military Medicine Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.