
Abstract
Background:
The location of posterior hip impingement at maximal extension in patients with posterior femoroacetabular impingement (FAI) is unclear.
Purpose:
To investigate the frequency and area of impingement at maximal hip extension and at 10° and 20° of extension in female patients with increased femoral version (FV) and posterior hip pain.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Osseous patient-specific 3-dimensional (3D) models were generated of 50 hips (37 female patients, 3D computed tomography) with a positive posterior impingement test and increased FV (defined as >35°). The McKibbin index (combined version) was calculated as the sum of FV and acetabular version (AV). Subgroups of patients with an increased McKibbin index >70° (24 hips) and FV >50° (20 hips) were analyzed. A control group of female participants (10 hips) had normal FV, normal AV, and no valgus deformity (neck-shaft angle, <139°). Validated 3D collision detection software was used for simulation of osseous impingement-free hip extension (no rotation).
Results:
The mean impingement-free maximal hip extension was significantly lower in patients with FV >35° compared with the control group (15° ± 15° vs 55° ± 19°; P < .001). At maximal hip extension, 78% of patients with FV >35° had osseous posterior extra-articular ischiofemoral hip impingement. At 20° of extension, the frequency of posterior extra-articular ischiofemoral impingement was significantly higher for patients with a McKibbin index >70° (83%) and for patients with FV >35° (76%) than for controls (0%) (P < .001 for both). There was a significant correlation between maximal extension (no rotation) and FV (r = 0.46; P < .001) as well as between impingement area at 20° of extension (external rotation [ER], 0°) and McKibbin index (0.61; P < .001). Impingement area at 20° of extension (ER, 0°) was significantly larger for patients with McKibbin index >70° versus <70° (251 vs 44 mm2; P = .001).
Conclusion:
The limited hip extension found in our study could theoretically affect the performance of sports activities such as running, ballet dancing, or lunges. Therefore, although not examined directly in this study, these activities are not advisable for these patients. Preoperative evaluation of FV and the McKibbin index is important in female patients with posterior hip pain before hip preservation surgery (eg, hip arthroscopy).
Keywords
Femoroacetabular impingement (FAI) is increasingly recognized as a cause of hip pain and early-onset osteoarthritis in young and active patients. 19,20 In the initial description of anterior FAI in 2003, 19 only cam, pincer, and mixed-type FAI were described without taking into account abnormalities of femoral version (FV), such as increased or decreased FV. However, it has recently been shown that both increased and decreased FV can significantly impair patient-related outcomes after hip arthroscopy for FAI. 17,18 For patients with valgus hips combined with increased FV, a posterior extra-articular hip impingement 47 conflict has been described. These patients were mostly women and had posterior hip pain and a positive posterior impingement test. 47 Decreased external rotation (ER) and extension were reported for these patients. Both femoral and acetabular version (AV) have a significant influence on hip range of motion (ROM), especially internal rotation (IR) and ER, 11,12 muscular lever arms, 43 and foot position. 9,27 In a recent study, a high prevalence of abnormalities of FV and increased FV and AV abnormalities were reported in symptomatic patients with FAI or hip dysplasia. 31
Physical impairment and sports activity limitations are very common in patients with anterior FAI 16 because flexion and IR are typically decreased in these patients. The diagnosis of FAI is usually based on an anterior impingement test, but objective assessment for ROM and location of impingement is challenging. In a recent systematic review investigating clinical tests for the diagnosis of FAI, the authors concluded that more specific diagnostic tests are needed for FAI. 41 Three-dimensional (3D) computed tomography (CT)–based virtual simulations 8,42,52 enable objective quantification of osseous hip ROM that cannot be studied using standard 2-dimensional imaging. To simulate ROM for complex or combined deformities (such as hip dysplasia or valgus hips with increased FV), the equidistant method 40 has been introduced. It is reportedly superior to previously presented motion algorithms. 40 With this method, increased FV (Figure 1) was described as a cause for posterior extra-articular hip impingement 47 located between the lesser trochanter and the ischial tuberosity. A 2021 study reported posterior extra-articular impingement in the presence of increased AV combined with increased FV. 32

Posterior osseous impingement location at maximal hip extension (no rotation) is shown. Impingement occurred extra-articularly between the ischial tuberosity and the lesser trochanter (red circle signifies first point of contact of bone-to-bone impingement) at 9° of extension (left), 15° of extension (middle), and 4° of extension (right).
The combination of increased FV with increased AV (combined version, also called the McKibbin index) is poorly understood. 47 In addition, it is unclear what kind of activities or sports are limited for patients with posterior impingement. We evaluated patient-specific 3D CT scans to assess limitations of hip extension (no rotation) and potential activities affected by these limitations. The purpose of this study was to use 3D models based on 3D CT scans to investigate the frequency and area of impingement at maximal hip extension and at 10° and 20° of extension in female patients with increased FV and posterior hip pain.
Methods
This study was an ethics committee–approved retrospective controlled comparative analysis of 50 hips in 37 female patients with increased FV (femoral anteversion; defined as FV >35° 55 ), posterior hip pain, and a positive posterior impingement test. All patients with increased FV were symptomatic and reported posterior hip pain at the time of image acquisition, and a positive posterior impingement test 53 and decreased ER were found during clinical examination (Table 1). All patients with posterior impingement were seen in the outpatient clinic of the University Hospital of Bern between January 2014 and December 2016 and were retrospectively reviewed. Inclusion criteria for all hips in the study group were female patients with increased FV in the presence of a nondysplastic acetabulum. Exclusion criteria were a lateral center-edge (LCE) angle <18° 34 or >39° 51 combined with an acetabular index >14°, 55 protrusio acetabuli, severe acetabular overcoverage, and Tönnis osteoarthritis grade ≥1. 54
Clinical Range of Motion of the 37 Female Patients (50 Hips) With Increased Femoral Version (>35° 55 ) a

a Data are displayed as mean ± SD (range). ER, external rotation; IR, internal rotation.
Of the 50 hips with increased FV, there were 24 hips with a McKibbin index >70° and 20 hips with FV >50°. There was some overlap of these 2 subgroups, as most of the patients with increased FV >50° had an increased McKibbin index >70°. The mean age of the patients was 30 years. For all patients with increased FV, the mean FV was 46° ± 10° and the mean AV was 25° ± 5°. All patients were part of a previous investigation. 32
For all hips, the diagnosis was based on the current recommendations of a positive correlation among symptoms, findings during physical examination, and radiographic findings, 46,53 as recommended by the Warwick Agreement. 20 Routine clinical examination included the anterior impingement test (pain in forced flexion, IR, and adduction; also called the FADIR 57 [flexion-adduction-IR] test), posterior impingement test (pain in forced extension and ER; also called the HEER 22 [hyperextension and ER] test), and anterior pain during the FABER (flexion-abduction-ER) test. A positive posterior impingement test and/or positive FABER was used as signs of potential anterior hip instability because some patients exhibited anterior hip pain during the FABER test. Two patients reported anterior hip instability during sports and had osteochondral lesions of the femoral head, and 1 patient exhibited anterior hip dislocation. Previous hip arthroscopy was performed in other institutions in 5 patients. One patient underwent 2 previous hip arthroscopies. Surgical treatment was performed in our institution in 25 hips (50%) of all hips. Proximal femoral derotation osteotomy to decrease FV combined with surgical hip dislocation was performed in 21 hips (42%), and 1 patient underwent hip arthroscopy for cam resection. In total, cam resection was performed for 16 hips.
Also included was a control group of 10 hips without cam or pincer deformity with normal FV (10°-25°) (Table 2) that were selected from the contralateral healthy hips of 146 patients who underwent CT-based computer-assisted total hip arthroplasty (THA) at another institution and who were part of a previous study. 47 All 10 hips were from female patients (mean age, 55 years) (Table 2). The contralateral hips of the patients with the following features were excluded: THA or total knee arthroplasty (n = 10), pain (n = 4), previous hip surgery (n = 3), Tönnis osteoarthritis grade ≥1 (n = 40), LCE angle <25° or >39° (n = 25), pistol grip deformity (n = 13), coxa profunda (n = 13), coxa vara or valga (n = 1), acetabular retroversion (n = 4), rotrusion acetabuli (n = 2), alpha angle >50° (n = 4), FV >25° (n = 5), femoral retroversion FV <10° (n = 2), and male sex (n = 10).
The descriptive and radiographic characteristics of the 3 study groups and the control group are shown in Table 2.
Descriptive and Radiographic Characteristics of the Study and Control Groups a

a Data are displayed as mean ± SD (range) unless otherwise indicated. BMI, body mass index; LCE, lateral center-edge.
Imaging
The measurement of FV was performed on standardized CT scans according to the method published by Murphy et al. 36 The Murphy method showed a smaller variability and higher accuracy 45 compared with biplane radiographs for measurement of FV. 25 AV was calculated on axial CT scans on the level of the center of the femoral head, 55 and the McKibbin index (also called the combined version or COTAV [combined femoral torsion-acetabular version] index 12 ) was calculated adding FV and AV. A cam-type deformity was defined as an alpha angle 38 >50° on lateral radiographs. Pincer-type deformity was defined as an LCE angle >34° 51 with an alpha angle <50°. A mixed-type deformity was defined as the combination of an alpha angle >50° and an LCE angle >34°. In total, 9 hips (18%) exhibited a pincer-type deformity and 54% (27 hips) had cam morphology.
All patients and controls underwent standardized anteroposterior and lateral radiographs and CT scans including the entire pelvis and the distal femoral condyles 39,40 according to a previously described protocol. 49 Some of the patients underwent MR arthrography. An osseous 3D model was generated of the CT of the pelvis and the femur using the Amira Visualization Toolkit (Visage Imaging). The acetabular reference coordinate system was the anterior pelvic plane, defined by both anterosuperior iliac spines and the pubic tubercles. 49,52 The femoral reference coordinate system was defined by the femoral head center, the knee center, and both femoral condyles. 36 For the simulation, the pelvis was in a fixed position, and the femur could move freely. Using the patient-specific 3D models of 50 hips derived from the CT scans, we compared the computed impingement-free ROM and impingement area, as described in previous studies. 6,7
Collision Detection Software
CT-based, patient-specific 3D models of 50 hips were evaluated using a validated 3D collision detection software to quantify the hip ROM and the acetabular and femoral location of impingement. 40,52 The 3D models were available from previous studies. 7,32 Each hip joint was then virtually simulated with the help of previously validated software. 52 This software uses the following tools: automatic rim detection, 39 a best-fitting sphere algorithm for identification of the femoral head center, and the equidistant method for motion analysis. 40 This method was specifically designed for virtual analysis of FAI. 40 Based on a validation study including cartilage, labrum, and joint capsule, an impingement collision can be detected with a mean accuracy of <3°. 40
Using this virtual analysis, we calculated the ROM for the following motions for all patients: flexion, extension, IR, and ER (at 0° and 90° of flexion). Maximal extension (Figure 2) was investigated as the first point of bone-to-bone contact after impingement-free extension. For calculation of location of impingement, 10° and 20° of extension (no rotation) were used. Then, impingement area was calculated at 20° of extension. For calculation of impingement area, the area inside of the red zone displayed in Figure 1 was marked with a brush tool and analyzed, as described in previous studies. 6,7 In a validation study of this software, intra- and interobserver measurements for these parameters for ROM were excellent (>0.9) for all motions except ER at 90° of flexion, where only moderate agreement 35 was described for the interobserver ICC. 52 Then, we evaluated one motion pattern, impingement-free extension (Figure 1). To calculate 10° and 20° of extension (Figure 2), extension was calculated in 1° intervals between 0° of flexion and 20° of extension (no rotation). The software used automatic rim detection 39 and best-fit sphere algorithms for identification of the femoral head center. 33
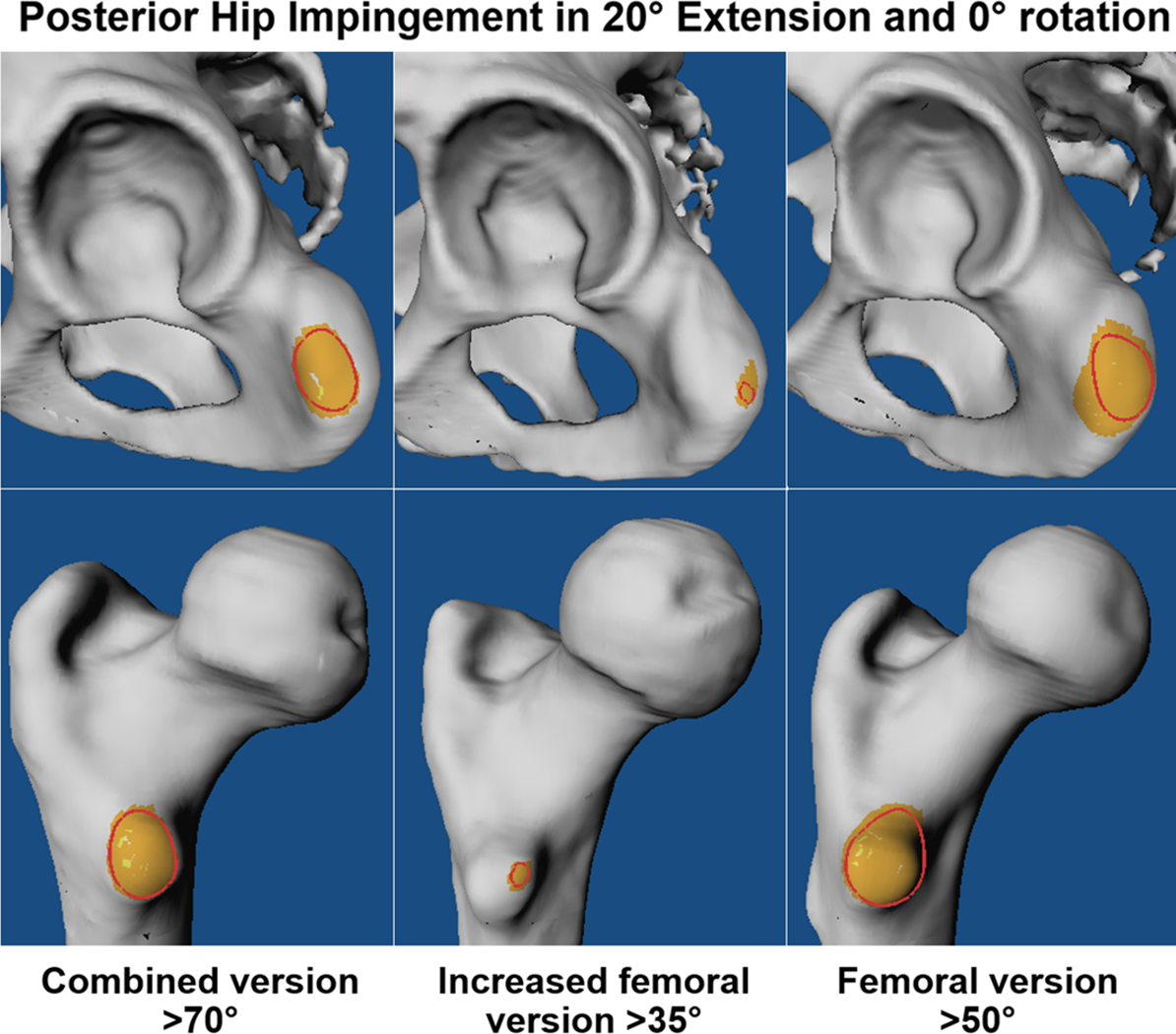
Posterior osseous extra-articular ischiofemoral hip impingement is shown at 20° of hip extension without rotation for the 3 groups (red circle signifies bone-to-bone impingement).
Statistical Analysis
We tested the data for normal distribution with the Kolmogorov-Smirnov test. Because not all the parameters were normally distributed, we used nonparametric tests for comparison. To compare descriptive and radiographic data, ROM, or location of impingement among the 3 study groups, we used a Kruskal-Wallis test; if significant, we used the Mann-Whitney U test to compare each of the 3 combinations of 2 groups. To compare binominal descriptive data and the prevalence of extra-articular impingement among the 3 groups, we used a chi-square test; if significant, we used the Fisher exact test to compare each of the 3 combinations of 2 groups.
Results
Mean impingement-free maximal hip extension was significantly lower in the female patients with FV >35° compared with the female control group (15° ± 15° vs 55° ± 19°; P < .001) (Table 3).
Range of Motion Based on Software for 3D Simulation of Hip Impingement Using Patient-Specific 3D Models for 3 Groups With Posterior Hip Impingement a

a Data are displayed as mean ± SD (range). The level of significance was adjusted for 3 groups (.05/3 = .016) with Bonferroni correction. ER, external rotation; IR, internal rotation; 3D, 3-dimensional.
b Significant difference compared with the control group (P < .05).
At maximal hip extension, 78% of patients with FV >35° had osseous posterior extra-articular ischiofemoral hip impingement (Figure 1) and 22% had posterior intra-articular (Figure 3) hip impingement (located on the posterior femoral neck and posterior-superior acetabulum). The mean impingement-free maximal extension was significantly lower in patients with McKibbin index >70° (11° ± 14°) compared with patients with McKibbin index <70° (19° ± 14°; P = .029) (Table 3).

Intra-articular location of osseous posterior hip impingement is shown at maximal hip extension (no rotation; red circle signifies first point of contact of bone-to-bone impingement). 3D CT, 3-dimensional computed tomography.
At maximal hip extension, most of the female patients with an increased McKibbin index >70° (79%) had osseous posterior extra-articular ischiofemoral hip impingement (Figure 2). Of the patients with FV >50°, the mean impingement-free maximal extension (9° ± 11°) was significantly (P < .001) lower compared with the female control group (55° ± 19°) (Table 3).
There was a significant correlation between maximal hip extension (no rotation) and FV (P < .001; r = 0.46) (Figure 4) as well as McKibbin index (P < .001; r = 0.456). At 20° of extension (no rotation), the frequency of osseous posterior extra-articular ischiofemoral impingement (Figure 2) was significantly (P < .001) higher for patients with an increased McKibbin index >70° (83%) and for patients with FV >35° (76%) compared with the control group (0%). Patients with FV >50° had the highest frequency (85%) of osseous posterior extra-articular ischiofemoral impingement at 20° of extension (no rotation). At 10° of extension (no rotation), posterior extra-articular ischiofemoral impingement was observed in 38% of hips with FV >35° and in 54% of hips with McKibbin index >70°. Patients with FV >50° exhibited the highest frequency (60%) of osseous posterior extra-articular ischiofemoral impingement at 10° of extension (no rotation). The correlation between impingement area at 20° of extension (ER, 0°) and FV and McKibbin index was significant (P < .001; r = 0.47 and r = 0.61).

Correlation between maximal hip extension (no rotation) and femoral version is shown for all female patients (50 hips) with increased femoral version. CT, computed tomography.
The impingement area at 20° of extension (ER, 0°) was significantly (P = .001) larger (251 vs 44 mm2) for patients with a McKibbin index >70° compared with patients with a McKibbin index <70°. The impingement area at 20° of extension (ER, 0°) in the control group was significantly (P < .001) lower compared with patients with a McKibbin index >70°. The impingement area was significantly (P = .01) larger for patients with FV >50° (20 hips) compared with patients with FV between 35° and 50° (246 vs 71 mm2).
Discussion
The aim of this study was to investigate the osseous impingement-free hip extension and impingement area at 20° of extension in patients with increased FV. Osseous patient-specific CT-based 3D models of 50 hip joints with increased FV (>35°) were compared using a previously validated collision detection software 40 for impingement simulation. Most importantly, significantly (P < .001) decreased hip extension compared with the control group was found. At maximal hip extension, most patients with FV >35° had posterior extra-articular ischiofemoral hip impingement. At 20° of extension (ER, 0°), the frequency of posterior extra-articular ischiofemoral impingement was significantly (P < .001) higher for patients with an increased McKibbin index >70° and for patients with FV >35° compared with the control group.
Impingement area (at 20° of extension) correlated with FV and McKibbin index. This underlines the importance of the McKibbin index when evaluating patients with posterior hip pain. Patients with FV >50° exhibited the highest frequency (85%) of impingement at 20° of extension (no rotation). Impingement was mostly located between the ischium and the lesser trochanter at maximal extension (Figure 2).
The results for the osseous ROM simulation match well with the literature for osseous collision detection for patients with increased FV and underline the validity of our data. 5,8,42 For valgus hips with increased FV, a decreased hip extension of 26° and ER in extension of 22° was described. 47 This corresponds to our results with slightly decreased mean hip extension and ER in extension (15° and 15°) (Table 2). Based on different software for collision detection, a slightly lower mean flexion of 110° ± 7° and a lower IR of 19° ± 6° were reported for hips with anterior FAI in 2012. 4 In this study, FV was identified as a contributor to IR, next to cam size and acetabular overcoverage. Comparing the results of the current study of IR at 90° of flexion, increased values were noted (Table 2). Higher values for IR were previously reported for patients with increased FV. 32,47 Another study that evaluated a computer-assisted 3D model of the hip reported a lower flexion of 107° ± 12° and a lower IR of 19° ± 13° in patients with a mean FV of 13° in 2011. 5 However, no information about hip extension was provided in this study. 5 The current study confirms the effect of FV for IR of the hip. Increased FV was associated with increased IR and vice versa. The technique used in the current study has been successfully applied to detect impingement-free ROM and location of impingement for patients with more complex deformities including FAI, 24 hip dysplasia, 49 valgus hips with increased FV, 47 and Legg-Calvé-Perthes disease. 50 This allows direct comparison to these studies.
In addition, the results for the location of impingement (Figure 3) compare well to the results reported for patients with increased FV combined with valgus morphology. 47 Few studies exist that have investigated impingement area in patients with posterior hip impingement. The correlation between impingement area at 20° of extension (ER, 0°) and FV and the correlation between impingement area and McKibbin index were significant (P < .001; r = 0.47 and r = 0.61). These findings are novel and underline that increased impingement area is associated with increasing FV and McKibbin index.
The effect of increased FV in patients undergoing hip arthroscopy has been investigated previously. 18 In 2015, the effects of FV and AV for patient-related outcomes after hip arthroscopy were investigated. 18 Two recent studies reported decreased outcomes for patients with increased FV after hip arthroscopy. 13,15 One study defined increased FV as FV >25° and reported that patients with increased FV had lower rates of clinically significant outcome improvement. 15 Another study evaluated patients with borderline hip dysplasia with FV >20° and reported a lower significantly lower mean modified Harris Hip Score compared with the control group. 13 They concluded that consideration of periacetabular osteotomy or femoral osteotomy could help surgeons to achieve optimal benefits for these patients. 13 This is in accordance with a recent study evaluating treatment for patients with increased FV with femoral derotation osteotomy. 29
This study has several important clinical implications. Small steps (with limited extension) could decrease hip pain for these patients. Restricted hip extension due to posterior hip impingement can affect sports and several activities of daily life (Figures 5A and B). One important activity is level walking, because walking requires 20° of hip extension according to a recent systematic review. 21 This review evaluated necessary hip ROM values using kinematic data of different studies evaluating motion capture systems. 21 Another important activity is running, because running requires 38° of hip extension. 21 Also, sports activities could be affected because of limited extension, especially ballet dancing and ice hockey. According to the systematic review, activities that require 20° of extension or more include ballet dancing, hockey, walking, and running. 21 Activities that require between 20° and 0° of extension include sitting cross-legged, squatting, soccer, lunging, landing, and stepping up and over. 21 The highest extensions were reported 21 for ballet dancing (42.8°), running (37.7°), hockey (20°), and walking (20°). Based on the results found in this study and the results of the recent systematic review, ballet dancing cannot be recommended to patients with increased FV (Figures 5A and B). The comparison with the mentioned review 21 should be interpreted with caution, because their results are based on motion capture systems measuring clinical ROM, which is different from the 3D CT used in the current study. In our study, the mean clinical measurement of hip extension (Table 2) was 10° lower than the hip extension in the simulation using 3D CT (Table 3).
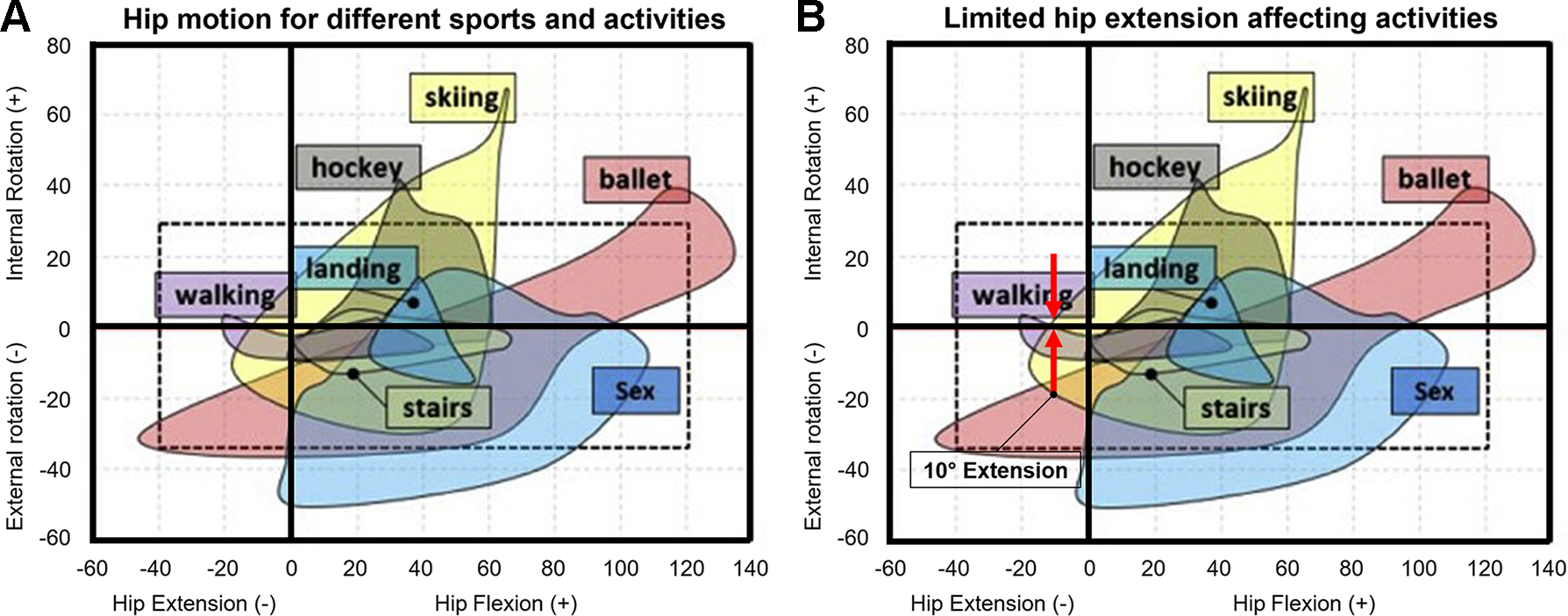
(A) Necessary hip motion for different activities based on a systematic review that evaluated the results of motion capture studies. (B) Limited hip extension affecting different activities based on a systematic review that evaluated the results of motion capture studies. Patients with increased femoral version or increased combined version had posterior impingement at 10° of hip extension without rotation (red arrows, B). Images reprinted from Han et al (2019) 21 with permission from Elsevier.
In comparison with previous studies 10,30,48 with clinical measurement of ROM in hips with FAI or hip dysplasia, the method in the current study had the following advantages: more accurate and anatomically based quantification of ROM because clinical assessment is subject to error, 14 isolated amplitudes of ROM (maximal extension) instead of the identification of motion patterns (posterior impingement test), and detection of the corresponding acetabular and femoral impingement location.
Limitations
One limitation of this study was that the software for collision detection that we used calculates the osseous ROM. The osseous ROM was calculated without considering the acetabular labrum or cartilage or other soft tissue. This is a previously known limitation for computer simulation of hip ROM. 23,37,52 Because other studies analyzed bone-to-bone impingement and the location of bony conflicts, 47,50,52 this limitation should not compromise our findings. Therefore, the clinical ROM (Table 2) was even lower, probably because of the soft tissue impingement (such as the quadratus femoris muscle in ischiofemoral impingement). A recent study reported reduced hip ROM if the acetabular labrum was included in the collision detection analysis. 2 Theoretically, the location of impingement could change by the 0.01 clock position after inclusion of the acetabular labrum. 2 However, this limitation was also described for previously published ROM results using different collision detection software. 5,8 For hips with different pathomorphologies, including hips with valgus morphology combined with increased FV, hips with slipped capital femoral epiphysis, 28 and hips with Legg-Calvé-Perthes disease or post-Perthes deformities, 50 this method has been applied previously. The application of this method to various hip morphologies and deformities underlines the validity of the software for the detection of impingement location applied in the current study. In addition, CT scans have the disadvantage of radiation exposure. MRI could be used in future studies to overcome this limitation. 26 This could be especially important for female patients of childbearing age.
As a second limitation, the patients included in this study were recruited from a university hospital with experience in hip preservation surgery, possibly with limited generalizability. A potential selection bias could be present because of patients with more complexities. Third, we did not report on clinical follow-up. However, this was not the aim of our study, and all patients were symptomatic at the time of image acquisition. Fourth, we used cutoff values of >35° and >50° for hips with increased FV. Different definitions for increased FV exist in the literature. 45 Using another cutoff value could lead to different results. Additionally, in the current study dysplastic hip joints were excluded. A dysplastic hip joint could be combined with increased FV or combined increased FV and AV. Future studies could analyze the effect of increased FV combined with periacetabular osteotomy 30 for the treatment of hip dysplasia. In addition, there was a difference in mean age between the patients and the control group (Table 1). This should not have influenced our results.
The current study analyzed female patients only (Table 1). This is in accordance with a previous study, which reported that ischiofemoral impingement (reduced ischiofemoral distance) was mainly observed in women. 3 Therefore, the conclusions of the current study are applicable to female patients only. This is attributable to the increased frequency of increased FV in women compared with men. It was previously reported that increased FV is more common in women. 31 In addition, physical and mental comorbidities were not evaluated. Osseous 3D models were generated with semiautomatic bone segmentation, which was checked with manual steps. This was necessary to ensure the accuracy of the patient-specific 3D models. Automatic bone segmentation 44,58 could hopefully overcome this limitation in the future.
Finally, we did not evaluate the effect of spinopelvine parameters (eg, pelvic incidence) or different pelvic positioning, such as anterior or posterior pelvic tilting, 56 which can also affect hip ROM (eg, anterior pelvic tilting decreases flexion and increases extension, anterior pelvic tilting could reduce posterior hip impingement). Given the reported difference of 5° less anterior pelvic tilt of male patients with cam-type FAI (at heel strike) in a dual fluoroscopy study, 1 this difference should be considered for clinical applications of the results of the current study.
Conclusion
Most of the patients with an increased McKibbin index >70° and half of the patients with an increased FV >35° have restricted hip extension <20° due to posterior extra-articular ischiofemoral hip impingement. Patients with FV >50° exhibited the highest frequency (85%) of impingement at 20° of extension (no rotation).
Although not studied directly in this study, it can be inferred from this study’s data that limited hip extension could affect the performance of sports activities such as running (eg, with long strides), lunges, and ballet dancing, and such activities are not advisable for these patients. This has implications for sports physicians, physical therapists, and orthopaedic surgeons performing hip preservation surgery (eg, hip arthroscopy). Preoperative evaluation of the McKibbin index is important in female patients with posterior hip pain.
Footnotes
Final revision submitted March 17, 2023; accepted March 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.N.N. has received education payments from Kairos Surgical. T.D.L. has received funding from the Swiss National Science Foundation (grant P2BEP3_195241). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics commission of the Canton of Bern (study No. 2018-00078).