
Abstract
Background:
It is clinically challenging to accurately drill femoral and tibial tunnels to reconstruct the anterior cruciate ligament (ACL). Mixed reality (MR) technology, a further development of virtual reality technology, presents virtual scene information in real time and establishes an interactive feedback information loop among the real world, the virtual world, and the user.
Purpose/Hypothesis:
The purpose of this study was to investigate the structural and early clinical outcomes of ACL reconstruction assisted by MR technology. It was hypothesized that MR technology would improve the accuracy of tunnel localization.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 44 patients at a single institution who underwent arthroscopic single-bundle ACL reconstruction between June 2020 and March 2022. Reconstruction with the aid of MR technology was performed in 21 patients (MR group), and conventional arthroscopic reconstruction was performed in 23 patients. Postoperatively, the parameters related to the bone tunnel positioning were compared by computed tomography imaging with 3-dimensional (3D) reconstruction, and 12-month postoperative clinical outcomes were assessed with the Lysholm and International Knee Documentation Committee scores.
Results:
There was no statistically significant difference in projection angles in the coronal, axial, or sagittal plane between the preoperative virtually created tunnel guide pin and the actual tunnel (P > .05 for all). In the MR group, the center of the femoral tunnel exit was closer to the apex of the lateral femoral condyle along the proximal-distal axis (14.07 ± 4.12 vs 17.49 ± 6.24 mm for the conventional group; P < .05) and the graft bending angle was lower (117.71° ± 8.08° vs 127.81° ± 11.91° for the conventional group; P < .05). The scatterplot of the femoral tunnel location distribution showed that the entrance and exit points in the MR group were more concentrated and closer to the ideal location of the preoperative design than in the conventional group. Patients in both groups had significant preoperative-to-postoperative improvement based on outcome scores (P < .001 for all), with no significant difference between groups.
Conclusion:
ACL reconstruction with the aid of MR technology allowed for more accurate positioning and orientation of the femoral tunnel during surgery when compared with conventional reconstruction.
Keywords
The anterior cruciate ligament (ACL) is an important anatomic structure connecting the tibia to the femur. It plays a vital role in limiting excessive anterior displacement of the tibia and maintaining the stability of the knee joint. 3,21,34 Once the ACL has been damaged or even ruptured, the stability of the knee joint will be seriously compromised. Patients will be at significantly increased risk of secondary meniscal injury, knee osteoarthritis, and even total knee replacement without further treatment. 35
ACL reconstruction remains the gold standard for patients with ACL injuries. 13 With in-depth research into the function and anatomy of the ACL and the development of minimally invasive surgery, the standard procedure for ACL reconstruction has shifted from open to arthroscopic ACL reconstruction. 9 Anatomic femoral tunnel placement allows the reconstructed ACL graft to be located within the natural ACL femoral attachment area, which has been shown to better restore anterior tibial displacement, knee rotational stability, and normal knee kinematics. 14,17 A survey at a recent international meeting revealed that nearly 70% of surgeons utilize the anterior medial portal to drill the anatomic femoral tunnel. 23
Arthroscopic ACL reconstruction is performed with a tunnel guide and anatomic marks to locate and orient the tunnel according to the surgeon’s own experience, which is somewhat arbitrary. 6,19 Commonly used independent drilling methods include the anterior medial portal method and the outside-in method to achieve free positioning of the femoral tunnel entrance. 4 However, the considerable variation in tunnel location and orientation makes it difficult to reconstruct bone tunnels individually and accurately. 32
In recent years, computer navigation systems have been used in ACL reconstruction. Computer navigation systems can assist in locating the bone tunnel of the graft and significantly improve the accuracy of the tunnel location. However, existing studies have not demonstrated a significant improvement in clinical outcomes of ACL reconstruction with computer navigation compared with conventional surgery, and there are shortcomings such as high economic costs, prolonged operative time, and additional medically induced injuries. 7,28,42,43 With the continuous improvement of hardware devices and algorithms, virtual reality (VR), augmented reality (AR), and mixed reality (MR) technologies have been introduced into the medical field. VR technology allows users to immerse themselves in a computer-generated environment fully. AR technology provides computer-generated overlays on real-world surfaces to provide users with 3-dimensional (3D) visual image models. MR technology enhances the realism of the user experience by presenting virtual scene information in real time, creating an information loop of interactive feedback among the real world, the virtual world, and the user. In the orthopaedic direction, VR technology is more often used in orthopaedic computer-assisted surgical systems and training simulators, mainly in the form of preoperative design to enhance surgical accuracy, improve patient prognosis, reduce surgical complications, and train surgeons in surgical technologies. 25,39 According to our search, there are no reports of ACL reconstruction surgery assisted by MR technology.
The aim of the current study was to compare MR-assisted ACL reconstruction with the conventional method of ACL reconstruction, investigate the accuracy of the tunnel location and the early clinical outcome of both methods, and provide new ideas for individualized reconstruction of the ACL. We hypothesized that (1) ACL reconstruction with the aid of MR technology could locate bone tunnels more accurately than standard methods and (2) ACL reconstruction assisted by MR technology could lead to better early clinical outcomes for surgical patients than standard reconstruction.
Methods
This was a retrospective clinical study comparing patients who underwent arthroscopic single-bundle ACL reconstruction with or without the assistance of MR technology between June 2020 and March 2022 by the same surgical team at a class A tertiary hospital. The protocol for this study received ethics committee approval, and all participants provided written informed consent.
Study Patients
A total of 147 patients underwent arthroscopic ACL reconstruction during the study period. We excluded all patients with ACL reconstruction with allogeneic tendon, previous knee surgeries on the affected side, infections, Kellgren-Lawrence knee osteoarthritis grade >2, fractures around the knee joint, and incomplete data in their medical records. According to the selection criteria, 44 patients were included in the study. They were distributed into 2 groups: 21 patients who underwent arthroscopic ACL reconstruction assisted by MR technology (MR group; n = 21) and 23 patients who underwent arthroscopic ACL reconstruction by the conventional surgery method (conventional group; n = 23).
All patients had a minimum of 6 months of follow-up. Other related procedures during ACL reconstruction included partial meniscectomy and meniscal suture repair. The descriptive data of the patients are shown in Table 1.
Baseline Characteristics of the Study Patients a

a Data are expressed as mean ± SD or No. of patients. MR, mixed reality.
Establishment of the MR Model
Preoperatively, all patients in the MR group underwent 64-slice computed tomography (CT) (Philips Brilliance iCT; slice thickness, 0.625 mm; scanning matrix, 512 × 512) of the affected limb. The images were saved in Digital Imaging and Communications in Medicine (DICOM) format, and the DICOM data were imported into Mimics medical software (Version 21.0; Materialise) to create a 3D model. The skin, soft tissue contour, femur, tibia, and fibula were retained in the model, but the patella was removed, and the lower limb was adjusted to 125° of knee flexion.
Creating the Virtual Guide Pin for the Femoral Tunnel
The femoral tunnel entrance was set on the 3D model based on the anatomic research of Bernard et al, 2 Bernard and Hertel, 1 and Fu et al 9 and the position of the original ACL on the femoral side of the patient. Usually, the femoral tunnel entrance center was located at 34% to 36% of the intracondylar height and 28% to 30% of the intracondylar depth on the Bernard quadrant. 1,2,29 Based on the study of the anatomy of the lateral femoral condyle by Osaki et al, 26 the femoral tunnel exit was set to be located at the anterior superior smooth position at the apex of the lateral femoral condyle to avoid the titanium plate covering the soft tissue; appropriate adjustments were made intraoperatively according to the actual situation of the patient. A 2 mm–diameter virtual cylinder was created through the center of the designated femoral tunnel entrance and exit as a virtual tunnel guide pin to guide the intraoperative femoral tunnel drilling.
Creating the Virtual Guide Pin for the Tibial Tunnel
The tibial tunnel entrance was set to start from the tibial tubercle on the medial side of the patellar ligament. The angle between the tunnel and the sagittal plane of the longitudinal axis of the tibia was set at 55° to 60° to obtain a sufficient bone tunnel. The tibial tunnel exit was set to be located in the center of the tibial insertion point of the ACL and slightly behind the center, usually about 1.8 to 2.0 cm medial to the tibial tubercle. A 2 mm–diameter virtual cylinder was created through the center of the designated tibial tunnel entrance and exit as a virtual tunnel guide pin to guide the intraoperative tibial tunnel drilling.
The tunnel virtual guide pins, bones, and soft tissue were distinguished by different colors in the model. The prepared limb model was imported into a HoloLens 2 MR head-mounted display (Microsoft) in msix file format for intraoperative use. Figure 1 shows the preoperative model with the design completed and imported into the HoloLens 2 head-mounted display.

The preoperative holographic models as presented in the Microsoft HoloLens 2 mixed reality head-mounted display. (A) The virtual tibial tunnel and femoral tunnel guide pin entrances. (B) The virtual femoral tunnel guide pin exit.
Surgical Technique and Rehabilitation Protocol
A group of senior orthopaedic surgeons with the same qualifications (including authors Z.W. and Y.X.) performed all operations with patients under nerve block anesthesia in the supine position with arthroscopic assistance.
MR Group
With the patient in the supine position, the affected knee was initially flexed to 90°, and a balloon tourniquet was used. During the operation, arthroscopy was routinely used to explore the knee joint cavity to confirm the ACL injury and clean the ACL stump. Figure 2 shows the surgical procedure of the MR group.
Tunnel Preparation
The knee joint was flexed to 125°. First, the femoral tunnel was prepared. The surgeon wore HoloLens 2 holographic display glasses and then projected the preoperative holographic model onto the affected limb, adjusting the model’s position and achieving registration through fitting skin contours and bony landmarks such as the medial femoral condyle, lateral femoral condyle, tibial tubercle, and fibular head (Figure 2). The femoral guide was introduced through the anterior medial portal. The position and direction of the femoral guide were adjusted according to the position and direction of the virtual femoral tunnel guide pin after registration. The femoral tunnel was drilled after confirming the position and direction of the femoral guide.
The medial 3 to 4 cm of the tibial tubercle, 2 to 3 cm below the tibial plateau, was selected as the entrance of the tibial tunnel, and the tibial tunnel was drilled in the same fashion as the femoral tunnel.

(A) The registration process of the surgeon, who wore Microsoft HoloLens 2 mixed reality holographic display glasses. (B) The projected holographic model and surgical site of the registration completed during the drilling of the femoral tunnel.
Ligament Placement
After completing any concomitant procedures (eg, meniscectomy or suture trimming), a graft of the corresponding size was fabricated and introduced into the bone tunnel. An Endobutton (Smith & Nephew) loop titanium plate was selected to fix the femoral side, and the tibial side was fixed with a hydroxyapatite extrusion screw. Figure 3 shows the operation process of the MR group.

The operation process of the mixed reality (MR) group. (A) Intraoperative exploration of anterior cruciate ligament (ACL) rupture. (B) The femoral attachment point of ACL. (C) The position and direction of the tunnel guide needle. (D) The 3-dimensional model and surgical site of the femoral side to complete the registration. (E) The femoral tunnel obtained with the assistance of MR technology. (F) The model and surgical site of the tibial side to complete the registration. (G) The tibial tunnel obtained with the assistance of MR technology. (H) The graft that completed the ACL reconstruction.
Conventional Group
The patient was in a supine position with 90° of flexion of the knee joint, and a balloon tourniquet was used. During the operation, arthroscopy was routinely used to explore the knee joint cavity to confirm the ACL injury and clean the ACL stump.
Tunnel Preparation
According to personal experience, the surgeon determined the location of the femoral and tibial tunnel openings of the intra-articular ACL by using bony landmarks, prepared the femoral and tibial tunnels directly through the guides, and inserted the corresponding size of the graft.
The treatments of graft and concomitant injuries were the same as those of the MR group, and the fixation methods were the same as those of the MR group.
Rehabilitation
Antibiotics were routinely used for postoperative prophylaxis, and isometric contraction training and ankle pump training were performed on the thigh and calf muscle groups on the bed immediately after surgery to promote muscle strength recovery and prevent complications such as deep vein thrombosis. All patients underwent rehabilitation training under the protection of knee braces, and an individualized rehabilitation plan was formulated according to the surgical method of meniscal injury. The rehabilitation plan was adjusted according to postoperative follow-up.
Postoperative Imaging and Functional Outcomes
Within 1 week after the operation, all patients underwent a 64-slice CT of the affected limb. The images were saved in DICOM format, and the DICOM data were imported into Mimics software to create a 3D model.
Evaluation of Tunnel Position
The same method was used to evaluate the tunnel position parameters in both study groups. All tunnel position parameters were assessed on 3D-reconstructed CT scans through the Mimics software measurement tools. Two radiologists with specific orthopaedic knowledge (J.L. and L.T.) blindly evaluated the patients’ postoperative imaging outcomes.
Projection Angle
The preoperative virtual tunnel guide pins and the postoperative actual tunnels were projected onto the coronal, axial, and sagittal planes, and the projection angles of the actual tunnel and guide pin on each plane were measured according to the methods of Montreuil et al 24 and Inoue et al 15 to compare the angles (Figure 4).

Three-dimensional computed tomography images of the (A) femoral and (B) tibial tunnels showing the projection angles for the preoperative virtual tunnel guide pins and the actual tunnels in the coronal (a and a′), axial (b and b′), and sagittal (c and c′) orthogonal planes. The dashed red line in each image indicates the projection line.
Bone Tunnel Measurement Parameters
To assess bone tunnel positioning, we measured the length of the femoral tunnel, the graft bending angle, and the center positions of the femoral tunnel entrance, femoral tunnel exit, and tibial tunnel exit. The femoral tunnel length was measured in millimeters as the length of the line segment connecting the center of the femoral tunnel entrance and exit. The graft bending angle was measured as the angle between the femoral tunnel and the intra-articular graft in the extended position of the knee joint. The center position of the femoral tunnel entrance was described using the percentage of intracondylar height and intracondylar depth in the Benard quadrant system. 1,2 To locate the center position of the femoral tunnel exit, the quadrant axis was set according to Osaki et al, 26 with the apex of the lateral femoral condyle as the origin, parallel to the long axis of the femur as the proximal-distal axis, and vertical to the long axis of the femur as the anterior-posterior axis. The center position of the tibial tunnel exit at the tibial plateau was described according to Tsuda et al 38 as the percentages of the medial-lateral side and the anterior-posterior side of the tibial plateau.
Evaluation of Functional Outcomes
All patients completed the Lysholm score and the International Knee Documentation Committee (IKDC) score before surgery, 3 months after surgery, and 6 months after surgery to evaluate the functional score of the affected limb. All evaluations were conducted by the same reviewer (J.W.).
Statistical Analysis
Continuous data that conformed to normal distribution were expressed as mean ± SD, and the independent-samples t test was used for comparison between groups. Categorical data were expressed as the number of patients, and the chi-square test was used to compare groups. P < .05 was considered a statistically significant difference. Analysis was performed using SPSS statistical software (Version 21.0; IBM).
SPSS statistical software (Version 21.0) was also used to make scatterplots of the center position of the femoral tunnel entrance, the center position of the femoral tunnel exit, and the center position of the tibial tunnel exit. Post hoc power analysis was performed using GPower Version 3.1 (University of Dusseldorf, Dusseldorf, Germany) to determine the study power.
Results
With an alpha of .05 and a sample size of 44, the post hoc power analysis for between-group comparisons revealed a power of 0.830.
The mean operative times were 135.00 ± 45.14 minutes and 122.91 ± 31.29 minutes for the MR group and conventional group, respectively, and there was no significant difference between the 2 groups (P = .304). There were no complications (eg, rupture of the posterior wall of the lateral femoral condyle, postoperative rebreaking of the graft, impact on the knee joint, meniscal injury secondary to surgery, infection, or neurological dysfunction) in either group. The mean follow-up period was 13.45 months overall (range, 7-29 months), with no significant difference between groups (mean follow-up, 14.71 ± 6.20 months for the MR group and 12.30 ± 4.80 months for the conventional group; P = .164).
Assessment of Bone Tunnel Positioning
Comparison of Projection Angles
The projection angles on the coronal, axial, and sagittal planes were 33.25° ± 4.94°, 33.60° ± 4.13°, and 44.44° ± 6.81°, respectively, for the virtual femoral tunnel guide pin and 36.75° ± 7.30°, 33.17° ± 5.45°, and 40.12° ± 8.23°, respectively, for the actual femoral tunnel. There was no statistically significant difference between the 2 projection angles on any plane (coronal, P = .077; axial, P = .777; sagittal, P = .071).
The projection angles on the coronal, axial, and sagittal planes were 79.68° ± 3.12°, 58.42° ± 9.36°, and 67.65° ± 4.64°, respectively, for the virtual tibial tunnel guide pin and 79.67° ± 4.52°, 58.43° ± 13.91°, and 67.63° ± 3.94°, respectively, for the actual tibial tunnel. There was no statistically significant difference between the 2 projection angles on any plane (coronal, P = .993; axial, P = .996; sagittal, P = .989).
Comparison of Bone Tunnel Measurements
Table 2 summarizes the bone tunnel measurements for the study groups. The graft bending angle of the MR group was significantly less than that of the conventional group (117.71° ± 8.08° vs 127.81° ± 11.91°, respectively; P = .002).
Comparison of Bone Tunnel Measurements Between Groups a

a Data are expressed as mean ± SD. Boldface P values indicate a statistically significant difference between groups (P < .05). MR, mixed reality.
b Measured as the percentage of intracondylar height and depth according to the Benard quadrant system. 1,2
c Measured as the distance from the apex of the lateral femoral condyle, parallel (proximal-distal) and vertical (anterior-posterior) to the long axis of the femur. 26
d Measured as the percentage of the anterior-posterior and medial-lateral sides of the tibial plateau. 38
There were no significant differences between the 2 groups in the position of the femoral tunnel entrance. However, according to the 3D model and scatterplot, the femoral tunnel entrance centers were more concentrated in the MR group and more divergent in the conventional group (Figure 5).

Three-dimensional models showing the distribution of the center position of the femoral tunnel entrance in the (A) mixed reality (MR) group and (B) conventional group. The red circle in panel A shows the ideal entrance center position of the MR model guide pin, and the blue circles show the actual center positions of the femoral tunnel entrance. (C) Scatterplot of the center position of the femoral tunnel entrance in the MR and conventional groups.
There was a statistically significant difference between the MD and conventional groups in the center of the femoral tunnel exit on the proximal-distal axis (14.07 ± 4.12 vs 17.49 ± 6.24, respectively; P = .04). There was no significant difference in the distance on the anterior-posterior axis; however, in 7 patients in the conventional group, the center of the femoral tunnel exit was located at the femur posterior to the apex of the lateral condyle. The 3D model and scatterplot showed that the femoral tunnel exit centers were more concentrated in the MR group and more divergent in the conventional group (Figure 6).

Three-dimensional models showing the distribution of the center position of the femoral tunnel exit in the (A) mixed reality (MR) group and (B) conventional group. The red circle in panel A shows the ideal exit center position of the MR model guide pin, and the blue circles show the actual center positions of the femoral tunnel exit. (C) Scatterplot of the center position of the femoral tunnel exit in the MR and conventional groups. AP, anterior-posterior; PD, proximal-distal.
There is no significant difference between the 2 groups on the center of the tibial tunnel exit along the anterior-posterior or medial-lateral axis. The 3D model and scatterplot of the center of the tibial tunnel exit are shown in Figure 7.

Three-dimensional models showing the distribution of the center position of the tibial tunnel exit in the (A) mixed reality (MR) group and (B) conventional group. The red circle in panel A shows the ideal exit center position of the MR model guide pin, and the blue circles show the actual center positions of the tibial tunnel exit. (C) Scatterplot of the center position of the tibial tunnel exit in the MR and conventional groups. AP, anterior-posterior; ML, medial-lateral.
Early Clinical Outcomes
At 12 months postoperatively, there were no significant differences in outcome scores between the MR group and the conventional group at any time point, and both groups saw significant preoperative-to-postoperative improvement in Lysholm and IKDC scores (P < .001 for all) (Table 3).
Comparison of Preoperative and Postoperative Outcomes Between Groups a
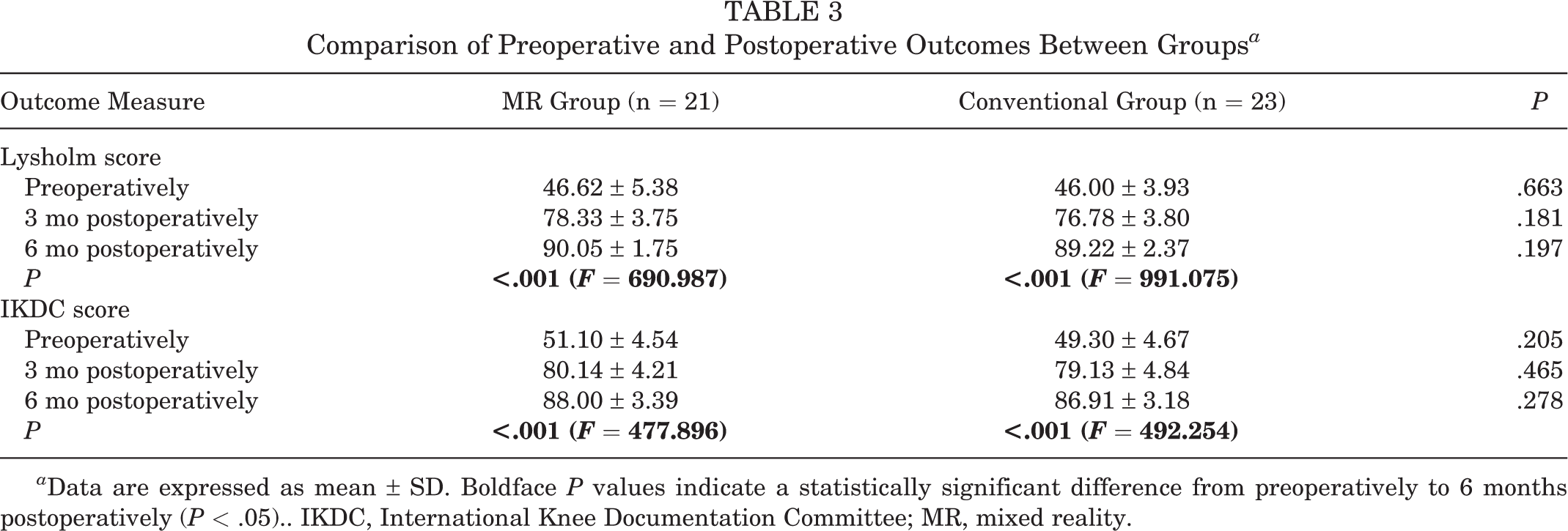
a Data are expressed as mean ± SD. Boldface P values indicate a statistically significant difference from preoperatively to 6 months postoperatively (P < .05).. IKDC, International Knee Documentation Committee; MR, mixed reality.
Discussion
In this study, significant improvement in femoral tunnel placement was found after MR technology–assisted ACL reconstruction compared with the conventional procedure. Both the scatterplot of tunnel location and the standard deviation of the quantitative location index indicated that the femoral tunnel exits in the MR group were more focused and closer to the ideal location planned preoperatively than those of the conventional group. Although this difference did not result in significant between-group differences in short-term functional outcomes, the primary goal of ACL surgery is the long-term stability of the knee and the prevention of osteoarthritis. More anatomic placement of the tunnel may show its benefits over a more extended follow-up period. 8
Regarding the center position of the femoral tunnel exit, patients in the MR group all had their femoral tunnel exit located in a smooth position anteriorly above the apex of the lateral femoral condyle, whereas 7 patients in the conventional surgery group had the femoral tunnel exit center located posteriorly above the apex of the lateral femoral condyle. Anatomic studies suggest that the area just above the lateral femoral condyle may be the attachment point of the lateral head of the gastrocnemius tendon (ie, the femoral tunnel may be drilled out from beneath the soft tissue), thus causing the lateral femoral fixation to overlap the soft tissue and increasing the risk of postoperative pain and eventual fixation failure. 26 We believe that ACL reconstruction assisted by MR technology can calibrate the deviation of the surgeon’s experience to a certain extent and provide a more intuitive drilling angle correction; in addition, the head-mounted display has no contact with the surgical area, which does not increase the risk of infection. It can also be used as an effective means for primary physicians to improve their surgical skills.
We found no statistically significant difference between the MR group and the conventional group in the tunnel position at the medial surface of the lateral femoral condyle and the tibial plateau. This finding is understandable, since we can perform arthroscopically with the guide positioning at these positions, especially on the tibial side, where the tibial guide locates the exit and entrance of the tunnel at the same time, and we can observe both arthroscopically and under direct vision. Thus, there is generally less variability in the tibial tunnel position.
According to previous reports, the precise positioning of the bone tunnel to achieve anatomic reconstruction is a decisive factor for long-term survival after ACL reconstruction and an ongoing challenge for orthopaedic surgeons. 10,36,41 Several studies have shown that during the creation of the femoral tunnel via the tibial borehole, the femoral tunnel is limited by the position of the tibial tunnel and does not allow for free positioning of the femoral tunnel entrance, making it difficult to achieve the large tilt of the graft in ACL anatomic reconstruction. 30,31,33 As a result, the reconstructed knee does not have good rotational stability, and the incidence of long-term osteoarthritis is higher.
Computer navigation systems have been used extensively in the spine, trauma, and joint fields, 27,37 and they have also been found to be accurate and reliable adjuncts to arthroscopic ACL reconstruction surgery, primarily for knee kinematic assessment and improving the accuracy of tunnel positioning. 7,16,22 In a previous case-control study on computer navigation system–assisted ACL reconstruction, we found that although there was no significant difference in postoperative knee stability or function between the computer navigation system–assisted and manual positioning groups, computer navigation–assisted ACL reconstruction allowed the femoral tunnel to be positioned closer to the anatomic position. 28 The navigation system is highly accurate, stable, and effective in reducing the risk of notch impingement and the impact of individual anatomic differences on the procedure. However, there are also problems such as calculation errors in the system; its high price; the increased length of the procedure because of preparation work, such as registration of the equipment and matching of information; the fixed position of the equipment; and the need for precise positioning of the equipment in relation to the patient’s space so as not to affect the surgeon. 5,20,42
In orthopaedics, VR and AR are more often used for teaching and preoperative planning, while MR is more promising for intraoperative guidance. 11,39 MR provides the surgeon with access to patient data in a sterile environment, providing intraoperative guidance while minimizing radiation exposure for both the patient and the surgeon. 18 In 2018, Gregory et al 12 reported a case of standard reverse shoulder arthroplasty performed with the assistance of the HoloLens MR system, which took no more time to complete than a conventional procedure, with postoperative CT assessment showing correct prosthesis position and no complications at the patient’s clinical visit 45 days after the procedure. In 2019, Wei et al 40 conducted a prospective study comparing the clinical outcomes of MR technology–assisted versus conventional percutaneous posterior convex vertebroplasty under C-arm fluoroscopy for osteoporotic vertebral compression fractures with intravertebral vacuum fracture. The clinical outcome of the MR technology–assisted group was found to be more satisfactory.
In our study, MR technology was applied to reconstruct the ACL to achieve accurate placement of the bone tunnel. Based on our search results, this article may be the first literature report on the application of MR technology in ACL reconstruction surgery. Preoperatively, a 3D model of the affected limb was reconstructed from the patient’s CT data. A preoperative simulation was performed to determine the best location for the bone tunnel entrance and exit and to set up the virtual tunnel guide pin. The surgeon wore HoloLens 2 holographic glasses during surgery to obtain information about the preoperatively designed 3D model. The virtual digital image was accurately matched to the patient’s surgical site for registration, and the bone tunnel was drilled under the guidance of the virtual tunnel guide pin, resulting in a new surgical approach that improved the accuracy of tunnel reconstruction. Patient anatomy and surgical instruments can be aligned correctly in spatial relations with the presented methodology. Combining 3D reconstruction and MR technology is a new mode of production, with visualization, plasticity, and rapid printing advantages. It can help surgeons to achieve accurate navigation and position in orthopaedic surgery.
Limitations
There are limitations to this study. First, the evaluators were not always blinded to the surgical procedure performed because of the retrospective nature. Second, our favorable results may be because of the senior surgeons' experience. Third, the manual registration method through body surface or bone markers still has limitations. New algorithms need to be further developed to achieve automatic registration of models to improve accuracy further. Finally, although our study aimed to focus on issues related to the tunneling parameters of MR technology–assisted reconstruction, further biomechanical studies are needed, along with conducting a prospective randomized controlled study, expanded sample size, and longer follow-up, so that a more reliable conclusion about the hypothesis raised can be made.
Conclusion
MR technology–assisted reconstruction of the ACL allowed for accurate positioning and orientation of the femoral tunnel during surgery, effectively improving the accuracy of femoral tunnel reconstruction without significantly increasing the operative time, making it a viable option for individualized ACL reconstruction.
Footnotes
Acknowledgment
The authors thank all editors and reviewers for their comments, suggestions, and efforts in reviewing this article. Their comments and suggestions were valuable for revising and improving the article and guiding the research.
Final revision submitted February 21, 2023; accepted April 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Talents’ Innovation Ability Training Program of the Army Medical Center of the People’s Liberation Army of China (Clinical Medicine Technological Innovation Ability Training Project, grant No. 2019CXLCC017) and the Key Talents Support Project of the Army Medical University (grant No. B-3261). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Army Medical Center of the People’s Liberation Army of China (reference No. 2020-88).